Most important takeaways…
- Federal Medicare law still bars NPs from signing the Certificate of Terminal Illness.
- Over 30% of Medicare hospice patients enroll seven days or fewer before death.
- Non-cancer diagnoses like dementia and heart failure complicate timely hospice referrals.
Nurse practitioners diagnose chronic kidney disease, complete advance directives, prescribe opioids for pain management, and coordinate complex care for geriatric patients. Yet when a 96-year-old woman with stage IV kidney disease, dementia, and a suspicious breast mass needed hospice care, her nurse practitioner could not sign the one document required to unlock the benefit. Diane Pagan, a nurse practitioner and founder of Senior Moments Care in Westchester, New York, detailed this legal barrier in a July 2026 article in The Examiner News.1 Her patient Marie qualified for hospice, and a home hospice agency accepted the referral, but Medicare law demanded a physician signature on the Certificate of Terminal Illness before care could begin.
This gap between clinical authority and regulatory permission is not unique to one patient or one state. It reflects a federal Medicare statute written more than four decades ago, before nurse practitioner advancement opportunities expanded to include full practice authority in over two dozen states. The barrier creates delays, increases family distress, and can prevent terminally ill patients from accessing timely comfort care when time is most precious.
The CTI Barrier: Why NPs Still Can't Certify Terminal Illness
To enroll a Medicare patient in hospice care, a physician must sign a form called the Certificate of Terminal Illness (CTI). That single signature triggers the benefit, allowing a dying patient to shift from curative treatments to comfort-focused care. For nurse practitioners who have managed a patient's complex conditions for months or years, the CTI requirement represents a frustrating administrative wall. Despite diagnosing the terminal illness, managing pain, and holding deep discussions about end-of-life goals with the patient and family, the NP cannot legally complete the one document that opens the hospice door.
How the CTI Works , And Who Is Excluded
The CTI is a Medicare requirement that confirms a patient has a life expectancy of six months or less if the disease follows its normal course. Without it, hospice agencies cannot bill Medicare for services, and the patient cannot receive the full interdisciplinary support hospice provides. The rule appears in the Medicare hospice conditions of participation, and its language specifies that only a physician, defined as a doctor of medicine or osteopathy, may certify the terminal prognosis. Nurse practitioners, clinical nurse specialists, and physician assistants are not listed as eligible certifying practitioners for the initial hospice admission, even though NPs can order home health services, sign plans of care, and diagnose life-limiting illnesses in many states.
This exclusion creates delays. When an NP identifies a patient who is ready for hospice, they must locate a collaborating or facility-based physician to review the case and sign the CTI. That physician may have little familiarity with the patient, and the extra step can add hours or days to an already urgent process. Meanwhile, the patient continues to receive treatments that may no longer align with their comfort goals.
Why the Disconnect Persists
The restriction is rooted in federal Medicare law written over four decades ago, at a time when nurse practitioners played a much smaller role in primary and specialty care. The statute has not been updated to reflect the modern scope of NP practice, which includes full practice authority to diagnose, prescribe, and manage chronic and terminal conditions in many states. Professional organizations like the American Association of Nurse Practitioners (AANP) and the American Academy of Hospice and Palliative Medicine (AAHPM) have long argued that this limitation is an outdated artifact that no longer serves patients.
Federal legislation has been introduced in recent congressional sessions to amend the Social Security Act and allow NPs and other advanced practice providers to certify terminal illness. These bills typically gain bipartisan support but face the slow pace of healthcare policy reform. In addition, the Centers for Medicare and Medicaid Services (CMS) periodically reviews hospice conditions of participation through rulemaking processes, and advocacy groups submit comments urging the expansion of certifying practitioners to include NPs.
What NPs Can Do While Waiting for Policy Change
- Stay informed through advocacy channels: Regularly visit the AANP government affairs page and AAHPM legislative tracker to learn about current bills. Setting up keyword alerts on Congress.gov for terms like "nurse practitioner hospice certification" can help track movement.
- Submit comments on proposed rules: When CMS opens a public comment period on hospice regulations, NPs can share real-world accounts of how the CTI restriction delays care. Personal stories carry weight. A nurse practitioner health policy toolkit can walk you through the process of submitting formal comments and contacting legislators effectively.
- Support state-level scope-of-practice alignment: Organizations like the National Council of State Boards of Nursing publish updates on state licensure changes. While the CTI is a federal rule, state-level full practice authority strengthens the argument that NPs are qualified to certify.
- Develop strong referral workflows: In the interim, build relationships with physicians who are willing to co-sign CTI forms quickly, and educate your workplace on the importance of streamlining this step so patients do not fall through the cracks.
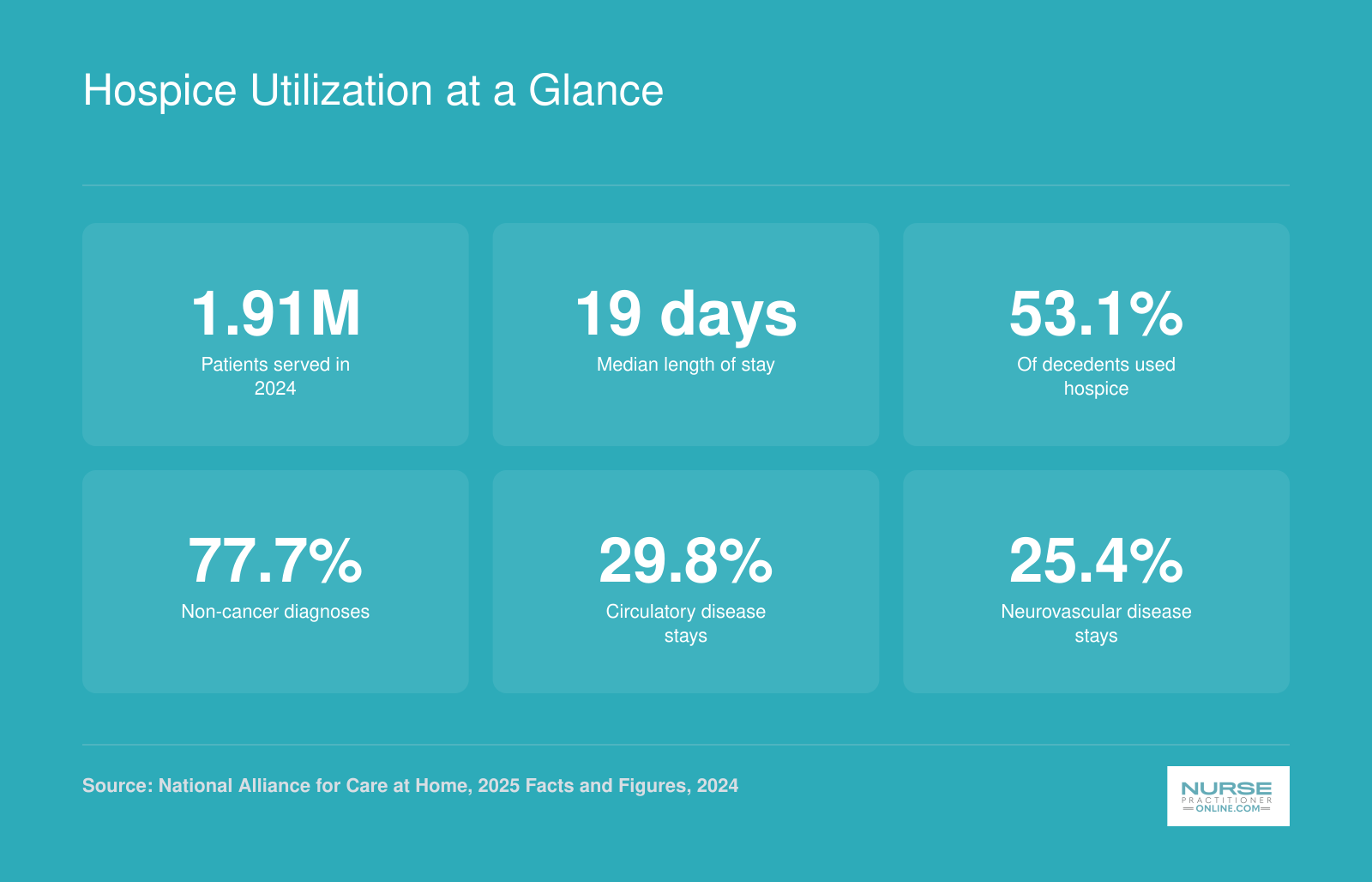
Hospice Utilization at a Glance
These national figures reveal just how deeply systemic barriers shape hospice access. When nurse practitioners cannot certify terminal illness, when referrals come late, and when non-cancer diagnoses complicate prognostication, the consequences show up in the data.
Policy and Regulatory Barriers to Hospice Enrollment
The Medicare hospice benefit, written into law in 1982, requires a physician to certify that a patient has a prognosis of six months or less if the illness runs its typical course. This prognosis rule forces NPs and physicians alike into a clinical guessing game that undermines timely referrals, particularly for patients with non-cancer diagnoses whose trajectories are notoriously unpredictable. Heart failure, dementia, chronic obstructive pulmonary disease, and advanced kidney disease can all plateau for months or decline suddenly, making six-month survival estimates unreliable at best and ethically fraught at worst. Providers hesitate to certify, patients miss the hospice window, and many die in hospitals rather than at home.
The All-or-Nothing Dilemma Under Traditional Medicare
Medicare's hospice benefit imposes a second barrier: patients must forgo curative treatment to enroll. This all-or-nothing framework forces families to choose between aggressive intervention and comfort care, a false binary that deters enrollment even when hospice would improve quality of life. A patient with stage IV heart failure, for example, may still benefit from diuretic adjustments or transfusions, but under traditional Medicare hospice rules, accepting those treatments can disqualify them from receiving home nursing, chaplaincy, and medication management through the hospice benefit. Many patients and families decline hospice rather than give up treatments they perceive as life-sustaining, even when those treatments offer marginal benefit. Understanding hospice versus palliative care can help NPs frame these conversations more clearly for patients and families weighing their options.
Medicaid Concurrent Care and Commercial Insurance Variations
Payer type fundamentally shapes access. Under the Affordable Care Act's Section 2302, Medicaid programs serving children can offer concurrent care, allowing patients to receive both hospice services and curative treatment. Some states have extended concurrent-care models to adults through Medicaid waivers, permitting patients to continue chemotherapy, dialysis, or other disease-directed therapies while enrolled in hospice. Commercial insurers vary widely: some mirror Medicare's restrictions, others permit concurrent care as a plan benefit, and a few offer hospice-like palliative programs that sidestep the terminal certification requirement altogether. This patchwork creates real confusion for palliative care nurse practitioners navigating referrals across patient populations.
State-Level Variation and NP Action Steps
State regulations add another layer. A handful of states allow Medicaid beneficiaries to receive palliative and curative services simultaneously, while others adhere strictly to Medicare's either-or model. NPs must know their patient's payer and their state's concurrent-care rules before initiating the hospice conversation. Start by asking: Is this patient on Medicare, Medicaid, or commercial insurance? Does your state Medicaid program allow concurrent care for adults? Does the hospice agency you refer to accept patients under a concurrent-care model? Answering these questions up front prevents the disheartening scenario of a willing patient, a willing family, and an NP who cannot deliver the benefit because the regulatory framework will not permit it.
Clinical and Diagnostic Barriers by Condition
Non-cancer diagnoses present the greatest challenge for hospice certification because disease trajectories are less predictable than those of malignancies. While oncology patients often show clear decline patterns, conditions like heart failure, dementia, chronic obstructive pulmonary disease, and chronic kidney disease fluctuate in ways that make prognosis difficult to document within the six-month terminal timeframe Medicare requires.
Understanding Diagnosis-Specific Criteria
Medicare contractors publish Local Coverage Determinations that outline the clinical markers a patient must meet before hospice admission is approved. These criteria vary by diagnosis and can be highly technical. For heart failure, guidelines typically reference New York Heart Association functional classifications and require documentation of optimal treatment failure. Dementia criteria often involve functional assessment scales measuring activities of daily living, mobility, and communication. COPD and chronic kidney disease each have their own benchmarks tied to lab values, oxygen dependence, and symptom burden.
Because these criteria change and vary by Medicare Administrative Contractor region, nurse practitioners should consult the Medicare Coverage Database directly. This database, maintained by the Centers for Medicare and Medicaid Services, allows you to search by diagnosis and region to find the exact eligibility language your documentation must address.
Finding Authoritative Clinical Guidance
Several resources can help you navigate condition-specific hospice barriers:
- CMS Medicare Coverage Database: Search for hospice LCDs by state and diagnosis to understand what documentation surveyors expect.
- National Hospice and Palliative Care Organization: Offers clinical practice guidelines and policy updates on eligibility criteria across diagnoses.
- American Academy of Hospice and Palliative Medicine: Provides condition-specific resources and position statements on prognostication challenges.
- Disease-specific professional associations: Organizations like the Heart Failure Society of America and the Alzheimer's Association publish guidance on end-stage disease recognition that aligns with hospice eligibility frameworks.
Common Documentation Pitfalls
Many hospice referrals are delayed or denied because clinical documentation does not explicitly connect the patient's presentation to LCD criteria. A patient may clearly be declining, but if the chart lacks specific functional assessments, lab values, or medication histories that match the published criteria, the hospice agency cannot accept the referral.
Nurse practitioners can strengthen referrals by learning which assessment tools are referenced in LCDs for their patient populations. For dementia patients, this often means documenting functional decline on validated scales. For cardiac patients, it means recording ejection fractions, medication regimens, and hospitalization frequency. Chronic kidney disease referrals may require recent GFR values and documentation of dialysis decisions. Building strong nurse practitioner patient care teams early in a patient's decline makes this documentation far easier to gather consistently.
Building a Personal Reference Library
Rather than searching for criteria during a time-sensitive referral, consider building a quick-reference document for conditions you encounter frequently. Pull relevant LCD language from the Medicare Coverage Database, note which assessment tools satisfy each criterion, and keep templates for the narrative portions of hospice referrals. This preparation reduces delays when a patient like Marie needs immediate access to comfort care. Nurse practitioner tools and apps designed for clinical practice can help you organize these references and keep them accessible at the point of care.
Understanding these condition-specific barriers is essential groundwork. Once you know what the system requires, you can document more effectively from the first visit and advocate for your patients when their disease trajectory does not fit neatly into regulatory boxes.
Barriers by Care Setting: Home, Inpatient, and Nursing Facility
The care setting where a patient resides shapes hospice access in profound ways, and nurse practitioners must understand these distinctions to advocate effectively for their patients. Each environment presents unique logistical, financial, and interpersonal barriers that can delay or prevent hospice enrollment, even when the patient clearly meets clinical criteria.
Home Hospice Requirements
Home hospice remains the most common setting for end-of-life care, but it comes with prerequisites that not every patient can meet. Medicare requires a willing and able caregiver to be present, which excludes patients who live alone or whose family members work full-time and cannot provide consistent support. The home environment must also be safe enough for hospice staff to deliver care, meaning patients in unstable housing situations or homes with significant safety hazards may face enrollment barriers.
For NPs who provide home-based primary care, as Diane Pagan does through her Senior Moments Care practice in Westchester, these requirements can create heartbreaking gaps. You may have a patient whose daughter desperately wants comfort measures at home, but if that daughter cannot take leave from work or if the home lacks basic accessibility features, hospice agencies may hesitate to admit. Learning how to collaborate with hospice nurses and families ahead of time can reduce these delays when a patient's needs become urgent.
Nursing Facility Complications
Hospice care in skilled nursing facilities involves a tangled web of payment and personnel issues. When a patient receiving Medicare Part A skilled nursing benefits elects hospice, the payment structure shifts in ways that create confusion and sometimes resistance. The nursing facility continues receiving a reduced per diem rate while the hospice agency bills separately for hospice services, and this dual-payer arrangement can generate billing disputes.
Beyond finances, facility staff may resist hospice involvement due to competing care philosophies, unfamiliarity with hospice protocols, or concerns about additional oversight. NPs working with nursing facility patients should anticipate the need to educate facility leadership and coordinate closely with both teams. A working knowledge of primary care billing and coding can help you navigate these dual-payer conversations with confidence.
Inpatient Hospice Limitations
Inpatient hospice beds are scarce resources, typically reserved for patients experiencing acute symptom crises that cannot be managed at home or in a nursing facility. This scarcity means patients who might benefit from a brief inpatient stay for pain management or symptom stabilization may wait days for a bed to open.
Rural Access Gaps
Rural patients face compounding geographic barriers. Many hospice agencies limit their service areas to urban and suburban zones where travel distances remain manageable, leaving remote communities without coverage. Nurse practitioners in rural healthcare feel these limitations acutely because they often serve as the primary or sole provider for complex geriatric patients.
A practical strategy for all NPs: identify hospice agencies in your service area now, before a crisis arises. Learn their admission criteria, geographic boundaries, and any setting-specific restrictions. This preparation allows you to guide patients and families toward realistic options rather than scrambling when time is short.
Questions to Ask Yourself
Cultural, Language, and Health Equity Barriers
Two patients with the same terminal diagnosis may face vastly different paths to hospice care based solely on race, ethnicity, language, or sexual orientation. Hispanic adults nationwide have 0.76 times the odds of enrolling in hospice compared to White patients (confidence interval 0.60 to 0.96), with enrollment probabilities for the lowest socioeconomic groups hovering around 40 percent (35 to 45 percent).1 Asian, Black, and Native American patients similarly enroll at lower rates, though after adjusting for clinical and demographic variables, disparities for non-Hispanic Black adults did not reach statistical significance in 2025 datasets.1 These numbers translate into thousands of patients dying each year without access to comfort-focused care they clinically qualified for.
Roots of Mistrust and Cultural Difference
Medical mistrust, rooted in well-documented historical harms such as the Tuskegee study and ongoing experiences of discrimination, drives many minority patients and families to decline hospice referrals.2 Language barriers compound the problem: when informed consent discussions occur through untrained family interpreters or not at all, patients cannot weigh hospice benefits and limitations meaningfully. Culturally specific beliefs about death, dying, and family roles further shape decision-making. Some cultures prioritize aggressive life-prolonging treatment as a sign of family devotion, while others emphasize peaceful home death but distrust institutional care systems.
LGBTQ+ Patients Face Distinct Obstacles
LGBTQ+ hospice patients report poorer care experiences nationwide, a finding mirrored in 2022 federal quality data.3 Many fear discrimination from hospice staff, worry about privacy violations if they disclose identity, or lack legal documentation for same-sex partners to serve as surrogate decision-makers in states where advance directive forms remain outdated. Transgender patients may encounter deadnaming or misgendering during deeply vulnerable moments at the end of life. These barriers lead some LGBTQ+ older adults to delay or refuse hospice entirely, choosing isolation over the risk of stigma.
What NPs Can Do Today
Effective interventions exist and belong in every NP practice. Use trained medical interpreters for all advance care planning conversations, not family members who may filter or reinterpret sensitive topics. Screen for social determinants early in the diagnostic trajectory: housing instability, food insecurity, and lack of caregiver support predict hospice underutilization. Partner with community health workers who share patients' language and cultural background to build trust and bridge system navigation gaps. Ask explicitly about cultural, spiritual, and religious preferences during advance care planning, framing hospice as a customizable service rather than a one-size-fits-all package.
Systemic fixes require institutional commitment: routine hospice referral workflows embedded in electronic records, diverse staffing, ongoing cultural humility training, and gender-neutral intake materials.4 Hospices that partner with churches, community leaders, and tribal organizations on Native American reservations see measurably higher minority enrollment.5 NPs who advocate for these changes within their organizations improve access not just for one patient at a time, but for entire populations historically left behind. The public health nurse practitioner role is well positioned to lead this kind of community-level outreach and equity work.
Related Articles
Patient and Family Decision-Making Barriers
Even when a nurse practitioner identifies a patient who clearly qualifies for hospice, the biggest obstacle may not be regulatory or clinical. It may be the people sitting around the kitchen table. Family dynamics, deeply held misconceptions, and caregiver guilt can stall or derail a hospice referral just as effectively as any policy barrier, and NPs need practical strategies for navigating these conversations with confidence and compassion.
Misconceptions That Block Hospice Enrollment
Families often carry beliefs about hospice that are firmly held but factually wrong. The most common include:
- "Hospice means giving up." Many families equate hospice with abandoning hope, when in reality it redirects the focus toward comfort, dignity, and quality of life.
- "Hospice hastens death." Research consistently shows that hospice patients often live as long as, and sometimes longer than, comparable patients receiving aggressive treatment.
- "Hospice is only for the last few days." Medicare's hospice benefit covers up to six months and can be recertified. Patients who enroll earlier tend to experience better symptom management and greater family satisfaction.
- "You can never go back to the hospital." Patients can revoke the hospice benefit at any time to pursue curative treatment, and certain conditions allow for short inpatient stays under hospice care.
These myths circulate in families, faith communities, and even among other healthcare providers. Correcting them early and often is part of the NP's role in hospice advocacy.
Caregiver Burden and Guilt
Family caregivers, particularly adult daughters and spouses, may resist a hospice referral because they interpret it as personal failure. After months or years of managing medications, appointments, and daily care, agreeing to hospice can feel like admitting they could not do enough. Others are simply too exhausted to process new paperwork, meet with yet another care team, or make one more life-altering decision. NPs should recognize decision fatigue in nurse practitioners and caregivers alike as a legitimate barrier and, where possible, simplify the enrollment process by coordinating directly with the hospice agency on behalf of the family.
Family Conflict Over Goals of Care
Disagreement among adult children is one of the most common reasons hospice referrals stall. One sibling may want "everything done," while another advocates for comfort care. Geographic distance complicates things further: the child who lives closest and provides daily care may feel overruled by a sibling who flies in for a weekend and demands a different plan. These conflicts can paralyze decision-making entirely, leaving the patient in limbo. NPs are often the most trusted clinician in the room, and drawing on conflict management in healthcare skills to gently clarify the medical reality without taking sides can break the impasse.
A Communication Framework for NPs
The most effective hospice conversations happen well before the crisis. Waiting until a patient is actively declining compresses the decision into a moment of panic and grief. Instead, normalize the topic early by weaving it into routine visits for patients with progressive illness.
A widely used framework is the "I wish, I worry, I wonder" approach:
- "I wish the medications were doing more to slow this disease."
- "I worry that another hospitalization could cause more suffering than benefit."
- "I wonder if it might be time to talk about what comfort-focused care could look like at home."
This language softens the conversation without being dishonest. It opens the door rather than pushing the family through it.
Another powerful tool is the time-limited hospice trial. Framing enrollment as "let's try this for two weeks and see how it feels" reduces the sense of finality that terrifies many families. Once they experience the support, the around-the-clock symptom management, and the emotional relief that hospice provides, most families choose to continue. Offering a trial reframes hospice from an irreversible decision into a reversible experiment, which is exactly what it is under Medicare rules.
Nurse practitioners who master these conversations do not just improve hospice enrollment numbers. They change the trajectory of a family's grief, replacing regret with the knowledge that their loved one's final chapter was guided by compassion and clarity.
Did you know? According to the National Hospice and Palliative Care Organization, over 30% of Medicare hospice patients enrolled in hospice for seven days or fewer before death in 2021. This underscores the urgency of initiating goals-of-care conversations early.
Strategies NPs Can Use to Overcome Hospice Barriers
Barriers to hospice enrollment are real, but they are not insurmountable. By building proactive systems into your practice, you can help more patients access comfort care when they need it most.
Start With the Surprise Question
Do not wait until a patient is actively dying to consider hospice. Instead, use the "surprise question" as a screening trigger: Would you be surprised if this patient died in the next 12 months? If the answer is no, it is time to begin hospice conversations and referral planning. This simple benchmark shifts your mindset from reactive to proactive and gives patients more time to benefit from palliative support.
Build a Hospice Referral Checklist Into Your EHR
Create a standardized hospice referral template for patients with qualifying diagnoses such as advanced dementia, stage IV chronic kidney disease, end-stage heart failure, or metastatic cancer. Your checklist should include:
- Completion of a Medical Order for Life Sustaining Treatment (MOLST) or similar form
- Documentation of prognosis discussions with patient and family
- Pre-identified collaborating physicians who can co-sign the Certificate of Terminal Illness (CTI)
- Contact information for 2 to 3 local hospice agencies your practice has vetted
Having this workflow embedded in your electronic health record ensures that hospice planning happens consistently, not just when someone remembers to bring it up.
Establish Physician Co-Signature Agreements Now
Until federal legislation allows nurse practitioner scope of practice to include signing the CTI independently, you need a reliable physician partner. Do not leave this to chance. Approach your collaborating physicians before you have a patient in crisis and establish a standing agreement for CTI co-signatures. Discuss turnaround expectations, preferred communication methods, and what documentation you will provide. When these agreements are already in place, the CTI becomes a formality rather than a last-minute scramble that delays hospice admission.
Use a Conversational Script for Family Discussions
Many families feel blindsided when hospice is mentioned. A gentle, human introduction can ease that transition. Consider language like this:
"I want to talk with you about what the next weeks and months might look like. Based on what I'm seeing, I think we should focus on keeping [patient name] as comfortable as possible. Hospice can help us do that, and it doesn't mean we're giving up. It means we're shifting our goals to quality of life and support for your whole family."
This script invites dialogue rather than announcing a decision. It acknowledges emotion while providing clear information.
Coordinate With Hospice Agencies Before You Need Them
Establish standing relationships with 2 to 3 hospice agencies in your area. Create a shared document for your care team that includes each agency's admission criteria, geographic coverage, contact information, and any specialties such as pediatric hospice or dementia-focused programs. Assign a specific team member, whether a nurse practitioner as primary care provider, a care coordinator, or a medical assistant, to follow up on every referral within 48 hours. This prevents patients from falling through the cracks during the intake process.
These strategies will not eliminate every barrier, but they will help you navigate a flawed system while advocating for the policy changes that are long overdue.
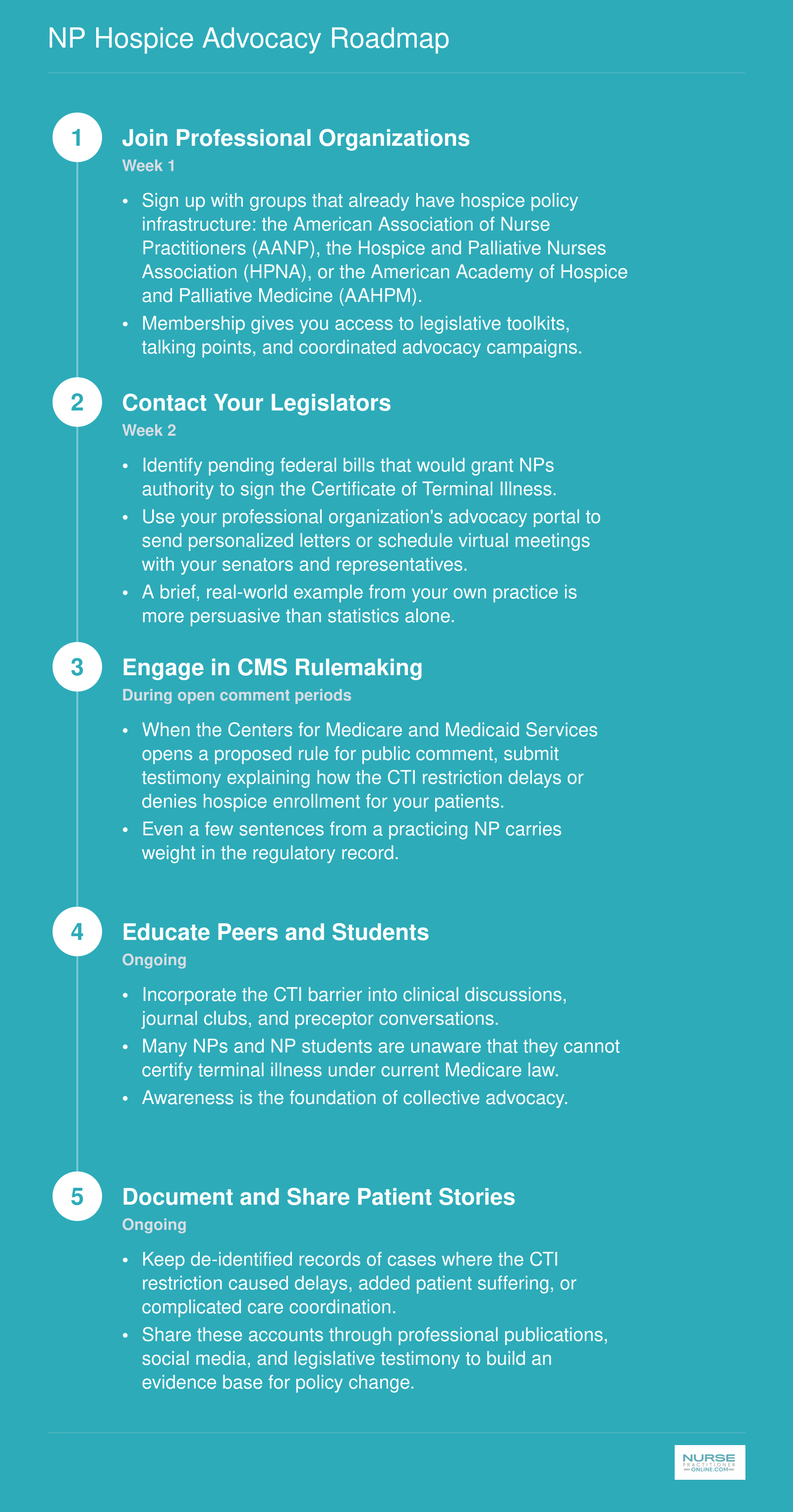
NP Hospice Advocacy Roadmap
Policy change does not happen on its own. It takes organized, persistent action from the clinicians who see the consequences of outdated rules every day. Here is a five-step pathway any nurse practitioner can begin this month to help dismantle barriers to hospice access.
Common Questions About NPs and Hospice Care
Navigating hospice referrals raises practical and policy questions that every nurse practitioner should be able to answer confidently. Below are the questions we hear most often, with concise answers that point you to the deeper discussions found throughout this guide.
- Can a nurse practitioner sign a hospice order?
- NPs can order many aspects of hospice care, but under current federal Medicare rules they cannot sign the Certificate of Terminal Illness (CTI) required for hospice admission. Only a physician (MD or DO) can certify a patient as terminally ill. This restriction, rooted in legislation written over 40 years ago, creates delays even when the NP is the patient's primary provider. See the CTI Barrier section above for a full breakdown.
- What are the most common barriers to hospice care?
- Barriers span several categories: regulatory limits like the CTI restriction, prognostic uncertainty for conditions such as dementia and heart failure, cultural or language gaps, cost misconceptions, and reluctance among patients and families to discuss end of life. The Policy and Regulatory Barriers section and the Clinical and Diagnostic Barriers section of this article explore each category in detail.
- Why is hospice underutilized in the United States?
- Hospice remains underutilized because of late referrals, restrictive eligibility rules, provider hesitancy around prognostication, and widespread misunderstanding of what hospice provides. Many patients enroll only in their final days, limiting the comfort and support hospice can offer. Understanding the evolving role of nurse practitioners in care delivery helps clarify why these gaps persist. The Hospice Utilization at a Glance infographic earlier in this guide puts current utilization trends into perspective.
- What are the barriers to hospice care for dementia patients?
- Dementia poses unique challenges because its trajectory is unpredictable, making it difficult to certify a six-month prognosis. Patients may lack decision-making capacity, and families often struggle to recognize when curative treatment is no longer beneficial. The Clinical and Diagnostic Barriers by Condition section discusses dementia-specific obstacles and strategies NPs can use to facilitate earlier conversations.
- How does Medicare affect hospice eligibility and access?
- Medicare covers hospice under the Medicare Hospice Benefit, but eligibility requires physician certification of a terminal prognosis of six months or less. Patients must also elect to forgo curative treatment for the terminal diagnosis. These rules, combined with the NP CTI exclusion, create enrollment bottlenecks explored in the Policy and Regulatory Barriers section of this guide. The broader NP role in modern healthcare makes this policy gap even more striking.
- What role do nurse practitioners play in end-of-life care?
- NPs diagnose, prescribe, manage symptoms, coordinate care teams, and guide families through difficult decisions. In many home-based and geriatric settings, the NP is the primary clinician. Despite this scope, the inability to sign the CTI limits NP authority at the critical moment of hospice enrollment. The Strategies NPs Can Use to Overcome Hospice Barriers section outlines advocacy and workflow approaches to close this gap.
The barriers standing between your patients and hospice care are real, but they are not permanent. Federal law written in 1982 still prevents nurse practitioners from signing the Certificate of Terminal Illness, even as NPs diagnose terminal conditions, prescribe opioids, and complete MOLST forms without restriction. That gap costs patients comfort and costs families peace.
You do not have to wait for Washington to act before making a difference. Contact your congressional representative about pending CTI legislation, build your hospice referral workflow this week, and start the goals-of-care conversation one visit earlier than feels comfortable. Those three steps, taken together, move patients away from the troubling reality that states with the greatest need for nurse practitioners are often the same communities where hospice access is thinnest, and toward the dignified death every patient deserves. If you are newer to navigating these complex end-of-life systems, what experienced NPs wish they had known earlier in practice can sharpen your instincts for advocacy and referral planning.