Most important takeaways…
- As of 2026, 27 states plus the District of Columbia grant nurse practitioners full practice authority.
- Transition-to-practice requirements in some FPA states can delay full independence by one to five years.
- NP salaries correlate more closely with geography and metro area than with practice authority level alone.
- Both NPs and PAs receive Medicare reimbursement at 85% of the physician rate in 2026.
As of 2026, 27 states plus Washington, D.C. grant nurse practitioners full practice authority, meaning NPs can evaluate patients, diagnose conditions, order tests, and prescribe medications without a physician collaboration agreement. The remaining 23 states impose reduced or restricted practice rules that require some form of physician oversight, often through written collaborative agreements that carry monthly fees ranging from a few hundred to several thousand dollars.
That regulatory split creates real tension for working nurses weighing where to live, where to license, and whether to pursue clinic ownership. Salary differences between full practice authority states and supervised states do not always favor the autonomous ones, and transition-to-practice hours can delay independent work by one to five years even after a state grants FPA status. Practice authority, in short, is a geography question as much as a credential question, and exploring nurse practitioner specialties and careers can help you match your clinical interests to the states where your autonomy will be strongest.
What Is Nurse Practitioner Practice Authority?
Practicing under a supervising physician versus running your own clinic: those two realities sit at opposite ends of what regulators call nurse practitioner practice authority. The difference is not just professional preference. It is written into state law, and it shapes nearly every workday decision an NP makes.
The Three Pillars of Practice Authority
Practice authority is the combination of three things a state grants (or withholds) for advanced practice registered nurses:
- Scope of practice: the specific clinical services you are legally allowed to provide, from diagnosing conditions to ordering imaging.
- Prescriptive authority: whether you can prescribe medications independently, including controlled substances in Schedules II through V.
- Physician oversight requirements: whether your work must be supervised, collaborated on, or signed off by a physician, and how formally that relationship must be documented.
When all three pillars allow the NP to evaluate, diagnose, order tests, and prescribe without a mandated physician relationship, the state is considered a Full Practice Authority jurisdiction. You will see this written on job postings and license applications as APRN-FPA, short for Advanced Practice Registered Nurse with Full Practice Authority. The acronym matters: recruiters in independent practice states use it as shorthand, and seeing it in a job description usually signals that the role expects you to operate autonomously from day one. To understand how these rules are evolving, our overview of NP scope of practice: what's changing is a helpful companion to this guide.
Set by States, Not Washington
There is no single federal standard for NP practice authority. Each state legislature, working through its board of nursing, sets the rules, which is why a family NP in Oregon can open a clinic while one in Texas needs a documented physician collaboration. Two national bodies track and lobby on these laws: the American Association of Nurse Practitioners (AANP) and the National Council of State Boards of Nursing (NCSBN). Their state-by-state maps are the standard references the rest of this guide draws on.
In states with full practice authority, a nurse practitioner as a primary care provider can hang their own shingle, sign orders without a co-signature, and write prescriptions for controlled substances under their own DEA number. In other words, practice authority sets the ceiling on your independence.
Full Practice Authority Vs. Independent Practice: What's the Difference?
The terms "full practice authority" and "independent practice" are often used interchangeably, but they represent different regulatory concepts that profoundly influence your scope of work, earning potential, and even where you can live. Understanding the nuance is critical when you're comparing licensure requirements, evaluating job offers, or planning a relocation.
The Two Frameworks: AANP vs. NCSBN
Nurse practitioner practice authority is shaped by two distinct classification systems. The American Association of Nurse Practitioners (AANP) defines three tiers: full, reduced, and restricted practice.1 Under full practice authority, NPs can evaluate patients, diagnose, order and interpret diagnostic tests, and initiate and manage treatments, including prescribing controlled substances, without a collaborative agreement or physician supervision.2 The AANP counts states with transitional requirements, such as a period of supervised practice before full independence, as full practice authority states.3
The National Council of State Boards of Nursing (NCSBN) follows the APRN Consensus Model, which breaks independent practice into three axes: independent practice, independent prescribing, and full licensure.4 Notably, the NCSBN does not count transitional full practice authority as truly independent. A state that requires new NPs to complete 2,000 to 4,000 hours of supervised practice before operating independently would be classified as full authority by the AANP but not by the NCSBN.5
When the Labels Diverge
The real-world application often blurs the labels. A state may grant full practice authority in name yet still tightly regulate prescriptive authority for certain schedules. For example, a state might allow NPs to practice without physician oversight but restrict their ability to prescribe Schedule II medications independently, requiring a collaborative agreement for those drugs. Conversely, a state designated as reduced practice might afford NPs a great deal of day-to-day autonomy in diagnosis and treatment, with physician involvement only required for a small fraction of cases.
Ambiguity also arises from business and setting constraints. Even in a full practice authority state, hospital bylaws or institutional policies can require physician co-signatures or supervision. Understanding whether the state's "independent" label truly covers all aspects of your intended practice is essential, especially if you're weighing whether to pursue a nurse practitioner post-master's certificate to expand into a new specialty.
What to Look for in Your Practice
When comparing job offers or deciding where to relocate, don't stop at the practice authority label. Dig into the specific details: Does the state's full practice authority include prescriptive authority for all controlled substance schedules? Are there any transition-to-practice hour requirements that could delay your full independence by two to three years? What do institutional policies demand beyond state law?
A position in a full practice authority state with a seamless prescriptive scope and minimal administrative hurdles often translates to higher earning potential and greater professional satisfaction. For a data-driven look at how these factors stack up geographically, see our guide to the best states for nurse practitioners in 2025. On the other hand, a seeming "full authority" state that still ties you to a physician for certain prescriptions can limit your practice in unexpected ways. Always verify the current regulations with your state board of nursing before making a career move.
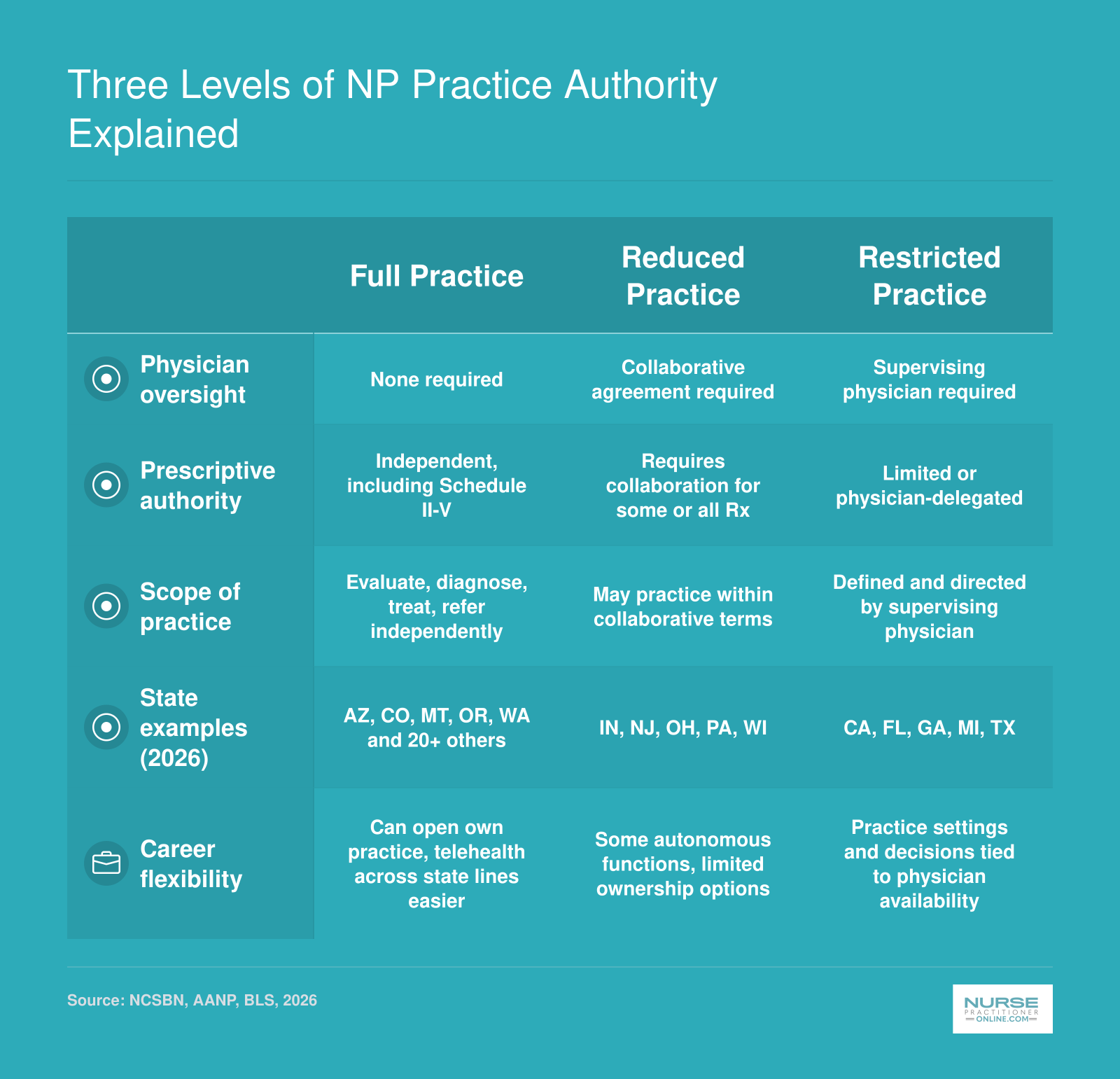
Three Levels of NP Practice Authority Explained
Nurse practitioner practice authority falls into three categories defined by the National Council of State Boards of Nursing (NCSBN). Understanding these levels helps you evaluate how your state's regulations shape your clinical autonomy, prescriptive rights, and career flexibility. Check the NCSBN website, your state Board of Nursing, the BLS Occupational Outlook Handbook, and the AANP's state practice environment map for the most current details.
Related Articles
Full Practice Authority States for Nurse Practitioners (2026 List)
As of 2026, 27 states plus the District of Columbia grant nurse practitioners full practice authority (FPA).1 That number has grown steadily over the past decade, and several states that joined the list between 2020 and 2024 still carry transition-to-practice requirements that are easy to overlook when comparing states side by side.
Understanding which states have FPA is only half the picture. Knowing whether your target state also requires a supervised or collaborative practice period before you can work independently is the detail that can reshape your career timeline by months or even years.
The 2026 FPA State List
The table below covers all confirmed full practice authority states as of 2026. The transition-to-practice column is the one most lists leave out, and it matters.
| State | Transition-to-Practice Required | Details | FPA Since |
|---|---|---|---|
| Alaska | No | No statutory requirement | 1994 |
| Arizona | No | No statutory requirement | , |
| Colorado | No | No statutory requirement | , |
| Connecticut | Yes | 2,000 hours over 3-year collaborative period | , |
| Hawaii | No | No statutory requirement | , |
| Idaho | No | No statutory requirement | , |
| Iowa | No | No statutory requirement | 1994 |
| Kansas | Yes | Transition period likely required; verify with state board | , |
| Maine | No | No statutory requirement | , |
| Montana | No | No statutory requirement | 1994 |
| New Mexico | No | No statutory requirement | 1994 |
| New York | Yes | Time-limited collaboration period required; hours not specified in national summaries | , |
| North Dakota | No | No statutory requirement | , |
| Oregon | No | No statutory requirement | 1994 |
| Rhode Island | No | No statutory requirement | , |
| Vermont | No | No statutory requirement | , |
| Washington | No | No statutory requirement | , |
| Wyoming | No | No statutory requirement | , |
Note: The table above lists confirmed states from available national summaries. The remaining FPA states are not yet fully catalogued in publicly available national summaries at the time of publication. Always verify current requirements directly with your state board of nursing, since legislation can change between publication cycles.
What the Transition Column Reveals
States that adopted FPA recently, particularly those that converted from reduced or restricted practice models, sometimes attached transition-to-practice requirements as a compromise during the legislative process. Connecticut is the clearest example: NPs there have full practice authority on paper, but new graduates must complete 2,000 supervised hours across a three-year collaborative arrangement before practicing independently.2
New York and Kansas are in a similar position.2 National summaries confirm that some form of transition period applies, but the specific hour requirements are not yet spelled out at the national summary level. If you are considering either state, go directly to the state board for the most current rules before making any decisions. For broader context on how these legislative shifts are unfolding, see our analysis of full practice authority here to stay.
Why the Effective Date Matters
States that adopted FPA as far back as 1994, including Alaska, Iowa, Montana, New Mexico, and Oregon, have had roughly three decades to build NP-led practice infrastructure: solo clinics, rural health networks, and independent billing relationships with insurers.3 That history tends to translate into a smoother path for NPs who want to open independent practices or take on clinical leadership roles as primary care nurse practitioners without needing physician co-signatures on routine administrative tasks.
Newer FPA states are still working through those systems, which is worth factoring in if your goal is to run your own practice rather than simply work without a formal collaboration agreement.
Questions to Ask Yourself
Reduced and Restricted Practice States for Nurse Practitioners
More than half of U.S. states still require nurse practitioners to work under some form of physician oversight, either through collaborative agreements or direct supervision models that limit how independently you can assess, diagnose, and treat patients.1
What Reduced and Restricted Practice Mean for Your Daily Work
Reduced practice states allow you to diagnose and treat patients independently in most situations, but you must maintain a formal collaborative agreement with a physician. In practical terms, this means you can see patients on your own, order labs and imaging, prescribe most medications, and manage chronic conditions without a physician reviewing every decision. However, you need a written agreement with a collaborating physician who agrees to be available for consultation, and the arrangement often comes with an annual fee you pay to the physician.
Restricted practice states go further in limiting your autonomy. You work under physician supervision, delegation, or team management structures that require a physician to be available to direct your practice, review charts, co-sign prescriptions, or directly oversee certain procedures. In these states, you function more as an extension of the physician's practice rather than as an independent provider, even after years of experience.
Current Reduced and Restricted Practice States (2026)
| State | Practice Level | Oversight Requirement | Typical Impact |
|---|---|---|---|
| Alabama | Reduced | Collaborative Agreement | Physician collaboration required; limited Schedule II prescribing in some settings |
| Illinois | Reduced | Collaborative Agreement | Written collaborative agreement mandatory; some controlled substance restrictions |
| Kentucky | Reduced | Collaborative Agreement | Collaboration required for controlled substances |
| New Jersey | Reduced | Collaborative Agreement | Joint protocol required; physician must be available |
| Ohio | Reduced | Collaborative Agreement | Standard care arrangement with physician |
| Pennsylvania | Reduced | Collaborative Agreement | Collaboration for all practice; prescriptive authority tied to agreement |
| Wisconsin | Reduced | Collaborative Agreement | Physician consultation required |
| California | Restricted | Supervision/Delegation/Team Management | Standardized procedures required; physician supervision for many functions |
| Florida | Restricted | Supervision/Delegation/Team Management | Physician supervision required; limited independent prescribing |
| Georgia | Restricted | Supervision/Delegation/Team Management | Direct physician supervision in most settings |
| Missouri | Restricted | Supervision/Delegation/Team Management | Collaborative practice arrangement with significant oversight |
| North Carolina | Restricted | Supervision/Delegation/Team Management | Physician supervision required for most clinical activities |
| Oklahoma | Restricted | Supervision/Delegation/Team Management | Physician supervision mandatory |
| Texas | Restricted | Supervision/Delegation/Team Management | Prescriptive authority through physician delegation |
| Virginia | Restricted | Supervision/Delegation/Team Management | Practice agreement required; physician oversight of diagnosis and treatment |
How Oversight Affects Your Career Flexibility
In reduced practice states, finding and maintaining a collaborative physician can add $3,000 to $8,000 annually to your practice costs if you work in an independent clinic or locum role. Many NPs in these states report that the collaborative requirement feels like a formality after the first few years, but it remains a legal necessity and a barrier to opening your own practice without physician partnership.
Restricted practice states present greater challenges for career mobility. If you want to open a retail clinic, work in a rural telehealth role, or serve as the sole provider in an underserved community, these models become legally impossible without an on-site or closely affiliated physician. The supervision requirement also affects hiring, as employers in restricted states often need to budget for physician oversight hours in addition to your salary, making NP positions less attractive from a cost perspective compared to states with the most need for nurse practitioners. For a broader look at how these regulations are shifting, see our nurse practitioner practice authority state-by-state analysis.
Transition-To-Practice Requirements by State
Transition-to-practice requirements are supervised clinical hours that newly licensed nurse practitioners must complete before they can practice independently, even in states that grant full practice authority. These requirements exist because many state legislatures view a structured mentorship period as essential for new graduates to build clinical confidence and competency before working without physician oversight.
Why Transition Hours Matter for Your Career Timeline
If you plan to open your own practice or work in a setting where you would be the sole provider, transition-to-practice rules directly affect how quickly you can achieve that goal. A state requiring 2,000 supervised hours translates to roughly one year of full-time work under a collaborative agreement before you gain full independence. States with longer requirements can delay your autonomy by several years. If you are mapping out a multi-year strategy, resources like career planning for RNs who want to become NPs can help you factor these timelines in from the start.
Currently, 28 states and territories offer some form of full practice authority, but only 14 of those grant it immediately upon licensure with no transition period.1 The remaining states with full practice authority require you to log supervised hours first.
State-by-State Hour Thresholds
Transition requirements vary significantly across states. Here are concrete examples that illustrate the range:
- Virginia: 9,000 hours over 5 years, the longest transition period in the country
- Maryland: 3,000 hours of supervised practice
- Vermont: 2,400 hours or 24 months under a practice agreement
- Minnesota: 2,080 hours, equivalent to about one year of full-time work
- Connecticut: 2,000 hours or up to 3 years with a collaborating physician
- Delaware: 2,000 to 4,000 hours depending on specialty and circumstances
- Nebraska and Nevada: 2,000 hours each
- Maine: 24 months of supervised practice
- Colorado: 1,000 hours, one of the shorter requirements
- South Dakota: 1,040 hours, roughly six months of full-time practice
These numbers represent the key differentiator when comparing states for career planning purposes.
Waivers and Exceptions
Some states waive or reduce transition requirements for NPs who bring prior experience or hold national certification for a specified number of years. If you have been practicing under a collaborative agreement in another state, your accumulated hours may count toward the new state's requirement. Checking with your state board of nursing about credit for prior experience can save you months or years of additional supervised practice.
Recent Legislative Changes
Utah eliminated its transition-to-practice requirement entirely, allowing NPs to practice independently from the moment of licensure.4 Several other states have introduced bills between 2024 and 2026 aimed at shortening or removing transition periods, though the legislative landscape continues to evolve. Staying current with your state nursing board and professional organizations like the American Association of Nurse Practitioners (AANP) helps you track changes that could accelerate your path to full independence.
NP Salaries: Full Practice Authority States Vs. Supervised States
Nurse practitioner salaries vary considerably from state to state, but the relationship between practice authority and pay is more nuanced than you might expect. Several full practice authority (FPA) states, such as California, Oregon, and Alaska, rank among the highest-paying states for NPs. However, restricted and reduced practice states like New Jersey, New York, and Texas also offer competitive wages. The reality is that cost of living, local demand, practice setting (rural vs. urban), and specialty all drive salary at least as much as whether a state grants full, reduced, or restricted practice authority. Use the table below to compare median annual wages, but keep these factors in mind before making a move based on pay alone.
| State | Practice Authority Level | Total NPs Employed | Median Annual Salary | 25th Percentile | 75th Percentile |
|---|---|---|---|---|---|
| California | Full | 20,980 | $166,610 | $140,260 | $205,400 |
| New Jersey | Reduced | 9,590 | $149,620 | $126,030 | $162,250 |
| Alaska | Full | 570 | $145,450 | $104,000 | $165,510 |
| New York | Reduced | 20,430 | $145,390 | $128,190 | $164,670 |
| Oregon | Full | 2,430 | $144,600 | $129,840 | $163,240 |
| Washington | Full | 4,790 | $140,220 | $125,890 | $161,730 |
| Connecticut | Full | 3,680 | $138,960 | $125,910 | $159,680 |
| Massachusetts | Full | 8,920 | $138,890 | $125,590 | $160,310 |
| New Mexico | Full | 1,870 | $138,440 | $113,240 | $156,000 |
| Arizona | Full | 7,540 | $133,790 | $115,290 | $151,650 |
| Montana | Full | 1,050 | $133,640 | $112,180 | $141,050 |
| New Hampshire | Full | 1,790 | $132,440 | $120,270 | $143,010 |
| District of Columbia | Full | 790 | $131,380 | $119,240 | $143,960 |
| Hawaii | Full | 470 | $130,940 | $121,410 | $158,100 |
| Rhode Island | Full | 1,200 | $130,710 | $126,200 | $160,030 |
| Texas | Restricted | 21,690 | $129,880 | $110,570 | $143,860 |
| Colorado | Full | 4,130 | $129,750 | $110,300 | $139,440 |
| Vermont | Full | 680 | $129,740 | $115,650 | $139,930 |
| Iowa | Full | 2,810 | $129,420 | $115,950 | $137,900 |
| Florida | Restricted | 24,690 | $129,010 | $109,670 | $143,670 |
| Idaho | Full | 1,570 | $128,940 | $119,290 | $140,920 |
| Illinois | Reduced | 9,560 | $128,620 | $111,450 | $138,420 |
| Wisconsin | Reduced | 4,950 | $128,580 | $117,630 | $137,150 |
| Minnesota | Full | 8,690 | $128,570 | $103,250 | $139,590 |
| Indiana | Full | 7,470 | $128,280 | $111,210 | $134,840 |
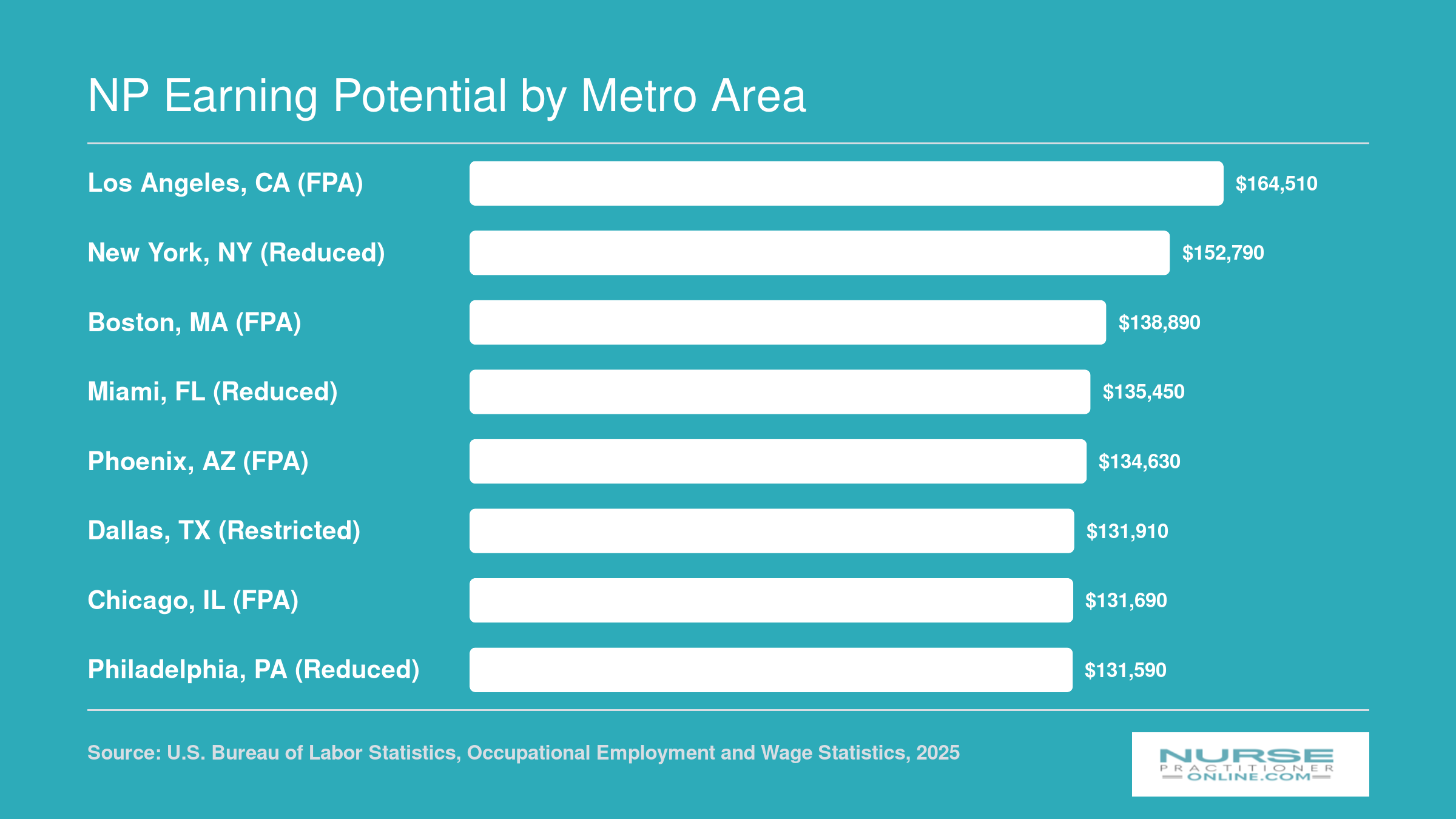
NP Earning Potential by Metro Area
Where you practice can significantly affect your earning potential as a nurse practitioner. The chart below highlights median NP salaries across ten of the highest-employing metro areas, based on the latest BLS data. Notably, top-paying metros span both full practice authority (FPA) states and reduced or restricted practice states, so practice authority level is just one of many factors that shape compensation.
How NPs With Full Practice Authority Compare to PAs and MDs
Nurse practitioners in full practice authority states and physician assistants both receive Medicare reimbursement at 85% of the physician rate in 2026, but the similarities end there.1 Understanding how NPs with FPA compare to PAs and physicians across scope, autonomy, billing, and training can help you set realistic expectations for your career trajectory and earning potential.
Scope of Practice and Autonomy
Nurse practitioners with full practice authority can evaluate, diagnose, order tests, and prescribe medications without physician oversight under state law.2 They can open their own clinics, hire staff, and serve as the sole provider in rural or underserved communities. Physician assistants, by contrast, still require a collaborative or practice agreement with a physician in every state, though the degree of day-to-day supervision varies.2 Physicians hold the broadest scope, with no statutory supervision requirements and full privileges based on specialty training and board certification.
Billing and Reimbursement
Both NPs with FPA and PAs can bill Medicare and Medicaid independently at 85% of the physician fee schedule.1 The key financial distinction for NPs in full practice authority states is that they do not need a physician's signature or collaborative agreement to submit claims. This allows NPs to capture the full 85% reimbursement for their own work, while PAs must structure their practice arrangements to account for physician oversight costs. Physicians bill at 100% of the Medicare rate, a 15-percentage-point premium that reflects their longer training and broader scope. For a deeper look at navigating claims and codes, see primary care billing and coding resources for nurse practitioners.
Training Length and Educational Pathways
Nurse practitioners complete a bachelor's degree in nursing, obtain RN licensure, and then pursue a master's or doctoral degree, typically totaling six to eight years of post-secondary education plus clinical experience. Physician assistants earn a master's degree after completing prerequisite coursework and direct patient care hours, usually totaling five to six years. Physicians complete four years of medical school followed by three to seven years of residency, totaling eleven to fifteen years of training after high school.
Can NPs Do 'Everything a Doctor Can'?
Even in full practice authority states, NPs face practical limitations that physician scope does not. Hospital credentialing policies often restrict NPs to associate or affiliate staff status, meaning they cannot serve as the admitting physician or attending of record in some facilities.3 Surgical privileges are another clear boundary: NPs generally cannot act as the primary surgeon and are limited to first-assist roles and minor procedures.3 Physician assistants face similar restrictions, requiring physician co-signature for certain privileges. Physicians hold full surgical and admitting privileges based on their specialty training and board certification, giving them access to roles and revenue streams that remain off-limits to advanced practice providers even in the most permissive regulatory environments.
The number of states granting nurse practitioners full practice authority has grown dramatically over the past decade. In 2018, only 23 jurisdictions offered full practice authority, according to research published in PubMed Central. By 2026, that number has expanded significantly as more states recognize the value of removing physician oversight requirements, nearly doubling the opportunities for NPs to practice independently.
Frequently Asked Questions About NP Practice Authority
Practice authority rules shape nearly every aspect of your NP career, from where you can work to how you run a clinic. Below are answers to the questions nurses ask most often when exploring independent practice options across the United States.
- What states allow nurse practitioners to practice independently without physician supervision?
- As of 2026, roughly half of U.S. states and territories grant nurse practitioners full practice authority, meaning NPs can evaluate patients, diagnose conditions, and prescribe medications without any physician oversight. States such as Arizona, Colorado, Montana, Oregon, and Washington have long permitted independent NP practice, and the list continues to grow as more legislatures pass supportive bills.
- How many states have full practice authority for nurse practitioners?
- The exact count shifts as new legislation takes effect, but approximately 27 states plus the District of Columbia and two territories currently grant NPs full practice authority. Several additional states allow full authority only after a supervised transition period. Because bills move through legislatures each session, it is worth checking your state board of nursing for the most current status.
- Can a nurse practitioner open their own practice?
- Yes, in full practice authority states an NP can legally open, own, and operate an independent clinical practice. This includes the ability to assess patients, order diagnostics, prescribe controlled substances, and bill insurers directly. In reduced or restricted practice states, opening a practice typically requires a formal collaborative agreement or physician supervision arrangement, which can add cost and complexity.
- What are the benefits of full practice authority for nurse practitioners?
- Full practice authority expands career options significantly. NPs gain the ability to establish independent clinics, especially in underserved rural and urban communities. It also removes the administrative burden and expense of maintaining physician collaboration agreements. Research consistently links full practice authority to improved primary care access, and many NPs report greater professional satisfaction and higher earning potential when practicing autonomously.
- Does the APRN Compact allow NPs to practice across state lines with full authority?
- Not exactly. The APRN Compact is designed to let NPs hold a single multistate license, but the practice authority level is governed by the destination state, not the state that issued the license. As of 2026, only four states (Delaware, North Dakota, South Dakota, and Utah) have enacted the compact, and it requires seven states to become operational. Several others, including Arizona, Idaho, Kansas, Kentucky, Montana, Nebraska, and New York, have pending legislation that could help the compact reach activation.
- Are there pending bills in 2026 that would grant new states full practice authority?
- Yes. Multiple state legislatures are considering bills that would either grant full practice authority outright or remove existing transition to practice requirements. On the compact front, at least seven states have pending APRN Compact legislation. Because legislative sessions vary by state and bills can stall or advance quickly, nurses should monitor their state nursing board and professional associations for real time updates on pending measures.