Most important takeaways…
- Medicare reimburses NPs at 85% of the physician rate, but incident-to billing can capture the full 100% when strict supervision rules are met.
- E/M code selection for 2025 and 2026 outpatient visits (99202 through 99215) hinges on medical decision making complexity, not time alone.
- Credentialing errors, not clinical mistakes, are the leading cause of Medicare Part B claim denials for nurse practitioners.
- NPs who master billing and coding can earn well above the national median salary of $129,210 reported by the Bureau of Labor Statistics.
Most nurse practitioner programs dedicate zero hours to billing and coding, yet reimbursement errors cost the average primary care practice between $5,000 and $15,000 per provider annually in denied claims, clawbacks, and missed revenue. You graduate ready to diagnose and prescribe, but rarely equipped to submit a clean claim or defend an audit.
Mastering primary care billing is not optional if you want autonomy, fair pay, or the ability to negotiate your own contracts. Medicare rules differ from commercial payers. Telehealth codes carry unique documentation requirements. Incident-to billing can boost practice revenue or trigger federal audits, depending on how you execute it. For NPs weighing which clinical path best aligns with billing independence, understanding the differences between acute care vs. primary care NP roles adds useful context.
The sections ahead walk through seven resource areas: Medicare reimbursement mechanics, E/M coding for office visits, incident-to and split/shared arrangements, private payer credentialing, telehealth claim requirements, common denial patterns, and how billing fluency translates to higher salary benchmarks. Practices increasingly expect new hires to bill correctly from day one, and NPs who can do so command stronger offers.
NP Billing Basics: How Nurse Practitioner Reimbursement Works
Medicare's long-standing policy of reimbursing nurse practitioners directly at 85% of the physician rate has shifted from a simple payment formula to a career-defining competency, as state laws evolve and telehealth regulations expand. Understanding this reimbursement backbone starts with federal rules, enrollment steps, and your local scope of practice.
How Medicare Sets the Baseline: The 85% Rule
At the federal level, nurse practitioners are recognized as billing providers under Medicare Part B. The key number to remember is 85%: CMS reimburses NPs at 85% of the Medicare Physician Fee Schedule amount for covered services. This applies whether you bill under your own National Provider Identifier (NPI) or through a group practice. The latest fee schedule and policy updates are always posted on CMS.gov; a quick search for "Medicare NP billing" will pull up the current year's conversion factor and relative value units. Bookmark the page and review it when annual updates drop each January.
Step 1: Enroll in PECOS to Bill Directly
Before you can submit a single claim, you must be enrolled in Medicare. The Provider Enrollment, Chain, and Ownership System (PECOS) is the online portal for NP registration. Head over to the Medicare Learning Network (MLN) for free, step-by-step enrollment guides that walk you through the required documents, NPI linkage, and attestation statements. Keep in mind that your application must reflect your state's practice authority: if your state requires a collaborative agreement, you'll need to submit that documentation as part of the enrollment package. Once approved, you'll receive a Medicare enrollment record that allows you to bill directly or reassign benefits to an employer.
Know Your State Scope of Practice
Federal reimbursement rules are one piece; state law is the other. Nurse practitioner billing authority is ultimately tied to scope-of-practice regulations. For a comprehensive breakdown, our guide to nurse practitioner practice authority by state details each jurisdiction's current status. The American Association of Nurse Practitioners (AANP) also maintains an up-to-date interactive map showing which states have full practice authority, reduced practice, or restricted practice. As of June 2026, 27 states and the District of Columbia have enacted full practice authority, meaning NPs in those states can evaluate, diagnose, and prescribe without a mandated collaborative agreement and can bill directly under their own NPI without needing a physician's co-signature. In other states, incident-to billing or split/shared services may be required to secure higher reimbursement. Always cross-check AANP's map with your state board of nursing's latest practice updates, because legislation can change quickly.
Staying Informed: Policy Changes and Employment Context
CMS occasionally releases transmittals that affect NP billing, from expanded telehealth codes to new chronic care management reimbursements. Set aside time each quarter to review AANP's advocacy alerts and CMS's MLN Connects newsletters. For a broader perspective on the profession's trajectory, the Bureau of Labor Statistics (BLS) projects nurse practitioner roles to grow 46% from 2023 to 2033, far outpacing other occupations. That growth amplifies the importance of mastering billing. The NPs who can navigate reimbursement efficiently will be better positioned for nurse practitioner advancement opportunities and independent practice.
E/M Coding for Primary Care Office Visits
E/M codes (Evaluation and Management) capture the clinical work of an office visit, from a straightforward single-problem check to a complex conversation about multiple new chronic conditions. For primary care nurse practitioners, fluency with the 2025-2026 outpatient code set (99202-99215) ensures accurate reimbursement and clear documentation.1
The 2025-2026 Outpatient E/M Code Set
The code range divides into new-patient and established-patient encounters. New-patient codes (99202-99205) apply when the NP (or another provider in the same group and specialty) has not rendered a professional service to the patient within the last three years. Established-patient codes (99211-99215) cover all other visits. Within each set, higher numbers indicate progressively greater clinical complexity and work. For example, 99204 and 99214 both reflect moderate-level decision making but differ by patient status.
Since 2021, history and physical exam no longer dictate the code level.2 Providers still record them as medically appropriate, but the final level hinges on medical decision making (MDM) or total time spent on the date of the encounter.3
Medical Decision Making Drives Code Selection
MDM is the primary driver because it reflects the clinical thought required. It breaks into three elements: - Number and complexity of problems addressed: This considers whether the issue is acute, chronic, stable, or unstable. - Data reviewed and analyzed: This includes ordering or reviewing labs, imaging, tests, outside records, or requiring independent interpretation. - Risk of complications, morbidity, or mortality: This factor weighs treatment risks, diagnostic procedure risks, and social determinants that affect health.
To reach a given MDM level, you need at least two of the three elements to meet or exceed that level's threshold.2 For instance, moderate MDM (99204/99214) requires two conditions like stable chronic illnesses plus prescription drug management. High MDM (99205/99215) demands two conditions such as a chronic illness with a severe exacerbation that poses a threat to bodily function or life.
A Primary Care Example: 99214 vs 99215
Consider a 45-year-old patient presenting for a first visit after a screening revealed elevated blood pressure and glucose. The NP reviews recent lab results from an outside facility showing an A1c of 7.8 and persistent hypertension. After a history and focused exam, the NP diagnoses type 2 diabetes and stage 1 hypertension. The plan: start metformin and lisinopril, order repeat labs in three months, and provide lifestyle counseling. Here the problems are two stable chronic illnesses (moderate); the NP reviewed external labs (moderate data); and prescribing two new maintenance medications constitutes moderate risk. Two of three moderate elements land the visit at a 99214.
What would push the service to 99215? Suppose the same patient arrives with a blood pressure of 200/120, blurred vision, and an A1c of 11. The NP recognizes impending hypertensive emergency and poorly controlled diabetes with a high risk of acute complications. The NP urgently coordinates with a cardiologist, orders immediate labs and imaging, and decides to administer antihypertensives on site. The problems are now high (acute exacerbation and threat of severe morbidity), and the risk is high due to the potential for rapid decompensation. Even if the data review remains moderate, meeting two high-level factors justifies 99215. Having reliable nurse practitioner tools at your fingertips can help you quickly cross-reference MDM criteria during documentation.
When Time-Based Coding Makes Sense
Total time on the date of the encounter offers an alternative selection method.3 Each code has a typical time threshold: for example, 99214 requires at least 25 minutes of total time, and 99215 requires at least 40 minutes.1 If counseling or care coordination dominates the visit, time-based coding often yields a higher, more accurate level than MDM alone. A medication review with extensive education on insulin self-management, diet, and activity might push a follow-up visit past 30 minutes, allowing the NP to bill 99214 even when the MDM level might otherwise be lower. Whichever method is used, documentation must explicitly support the chosen code, including a clear description of the clinical thinking or a time log when time drives the level.
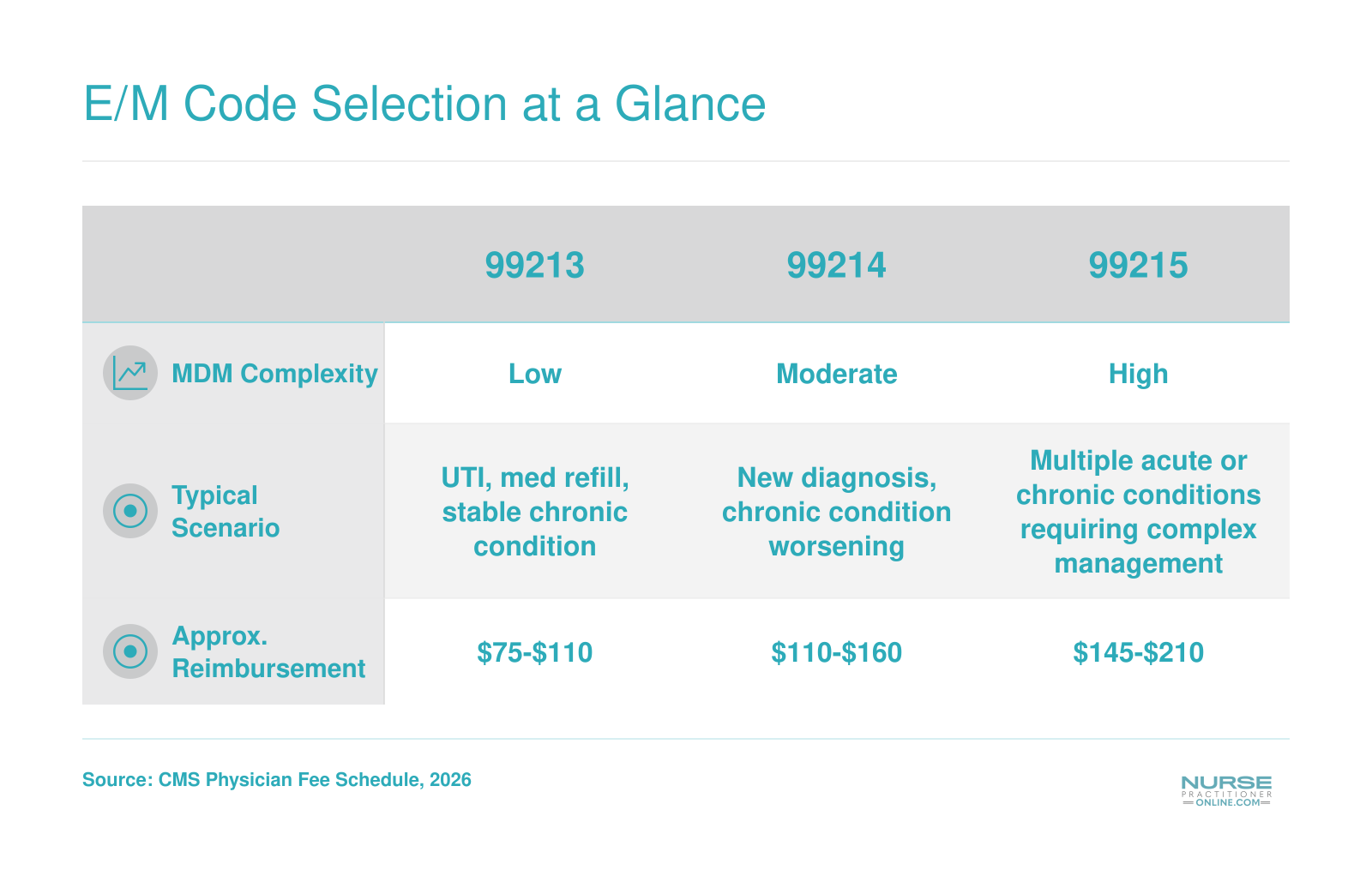
E/M Code Selection at a Glance
Evaluation and Management (E/M) codes are the backbone of primary care billing for nurse practitioners. Selecting the right code depends on the complexity of your medical decision making (MDM). Here is a quick comparison of the three most common office visit codes you will use in primary care.
Incident-To and Split/shared Billing Rules for NPs
When can an NP's visit be billed under the supervising physician's name and reimbursed at the full physician rate?
That is one of the most practical billing questions in primary care, and the answer turns on two distinct billing arrangements: incident-to billing and split/shared visits. Getting either one wrong is a fast track to a denied claim or an audit.
How Incident-To Billing Works
Incident-to billing allows a claim to go out under the supervising physician's National Provider Identifier, triggering reimbursement at 100% of the Medicare Physician Fee Schedule rather than the 85% rate an NP would receive under their own NPI.1 To qualify, every one of the following conditions must be met:
- Initial visit requirement: A physician must have performed and documented the initiating visit that established the diagnosis and plan of care. An NP cannot create that foundation.
- Same plan of care: The NP's subsequent visit must follow that established plan. If the patient presents with a new problem, the claim cannot go incident-to, period.
- Direct supervision: A physician must be physically present in the office suite and immediately available, though not necessarily in the same room. As of January 1, 2026, CMS allows virtual direct supervision through real-time audio and video technology, but audio-only connections do not satisfy the requirement.2
- Employment or expense relationship: The NP must be an employee or contractor whose costs are borne by the billing practice, not an independent contractor billing separately.
- Office or clinic setting only: Incident-to is not available in facility settings such as hospital outpatient departments.
Note that care management services like transitional care management and chronic care management follow a general supervision standard rather than direct supervision, which gives practices a bit more flexibility for those specific codes.1
Split/Shared Visit Rules Through 2026
Split/shared billing applies in facility settings, such as hospital outpatient clinics, where both a physician and an NP contribute to the same patient encounter on the same date. Under rules finalized through 2026, the determining factor is the substantive portion of the visit: whichever provider performs more than half of the total time documented for the encounter is considered the billing provider.3 If the NP performs the substantive portion, the claim goes out under the NP's NPI at 85%. If the physician does, it bills at 100%.
Documentation of time is now the critical variable. Practices that relied on other definitions of substantive portion in prior years need to confirm their workflows reflect the time-based standard now in effect. For NPs working as primary care nurse practitioners, understanding these billing mechanics directly affects both practice revenue and professional credibility.
A Real-World Workflow Example
Consider this scenario: a patient with Type 2 diabetes established care with the supervising physician two months ago. Today the NP is seeing the patient for a scheduled follow-up to review blood glucose logs and adjust medication. The physician is in the office suite, reachable immediately, and the visit addresses the existing diabetes plan with no new problems.
This qualifies for incident-to billing. The claim goes out under the physician's NPI at 100%.
Now change one detail: the patient mentions new knee pain and asks the NP to assess it. That new problem disqualifies the visit from incident-to status. The claim must revert to the NP's NPI at 85%, regardless of whether the physician is present.
The Compliance Risk You Cannot Afford to Ignore
Improper incident-to billing is a consistent focus of Office of Inspector General audits, and the most common finding is the absence of a qualifying initial service by the physician.4 Practices sometimes bill incident-to for visits where the NP saw the patient first, or where the physician's initiating note is missing from the record.
The financial exposure goes beyond repaying the 15% difference. Repeated improper billing can trigger False Claims Act liability. The safer habit is to verify incident-to eligibility at the scheduling or rooming stage, before the visit is ever documented, so the NP knows from the start which NPI the claim will use. Practices looking to tighten these pre-visit checks can draw ideas from nurse practitioner workflow improvement strategies.
Hospital and Facility Billing for Nurse Practitioners
Direct billing under your own NPI gives you the most autonomy in facility settings, but split/shared visits sometimes unlock higher reimbursement when a physician documents the substantive portion. Knowing when to use each path keeps your hospital practice both compliant and financially sound.
How NP Billing Works Across Hospital Settings
Hospital billing differs markedly from clinic-based reimbursement because Medicare pays a lower professional rate for services performed in facility locations.4 The facility itself bills separately for overhead, supplies, and nursing staff under a different component of the payment formula. As a nurse practitioner, you can bill directly under your own NPI at 85% of the Medicare physician fee schedule in all facility settings, including inpatient, outpatient, and the emergency department.1 Your choice of place-of-service code tells the payer where the encounter occurred:
- 21 (Inpatient Hospital): used for admitted patients receiving active care on a hospital unit.
- 22 (Outpatient Hospital): covers clinic visits, observation stays, and same-day procedures within the hospital campus.
- 23 (Emergency Room): applies to unscheduled visits in the emergency department, whether the patient is ultimately discharged or admitted.2
Split/Shared Billing in the Hospital Setting
For services furnished jointly by a physician and an NP in the same group practice on the same calendar day, Medicare permits split/shared billing. The entire service gets billed under the physician’s NPI at 100% of the fee schedule, but only if the physician documents the substantive portion. For 2024, the substantive portion is defined as more than half of the total time spent managing the patient encounter.2 This rule applies to evaluation and management visits in hospital inpatient, outpatient, and emergency department settings. It does not apply to critical care services or procedures. Both clinicians must document their portion of the visit, and the medical record must clearly indicate that the physician personally performed the substantive portion. Incident-to billing is never available in hospital settings,3 so split/shared is the only mechanism to capture full physician-level reimbursement for combined NP-physician work.
E/M Codes and Modifier Use
Common evaluation and management codes for hospital encounters include:
- Initial hospital care: 99221-99223
- Subsequent hospital care: 99231-99233
- Observation codes (e.g., 99218-99220 for initial observation, 99224-99226 for subsequent observation)
When billing directly under your NPI, append modifier -PN to the E/M code. This identifies the service as performed by a nurse practitioner and ensures correct reimbursement at the 85% rate. Skipping the modifier can trigger a denial or underpayment because the payer expects a physician-level modifier.
Compliance Tips for Hospital Audits
Facility billing is under intense scrutiny from Medicare and commercial payers. To pass an audit, your documentation must clearly support the level of service you billed, including the history, exam, and medical decision-making or total time spent. For split/shared visits, the record must explicitly show that the physician performed and documented more than half of the total time, with both clinicians’ notes present. Keep a log of split/shared encounters and flag any missing co-signatures promptly. Because facility rates are lower than non-facility rates,4 avoid inadvertently using office place-of-service codes (11) when the service was rendered in a hospital department. Even a small coding error can lead to recoupment down the road.
How to Bill Medicare as a Nurse Practitioner
Billing under a supervising physician versus billing under your own NPI as an independent provider: the difference shapes how much Medicare pays you, who gets the revenue, and how much professional autonomy you carry into every patient encounter. Getting this right starts before you ever submit a claim.
Enrolling Through PECOS
Medicare reimbursement for nurse practitioners runs through the Internet-based Provider Enrollment, Chain, and Ownership System, known as PECOS, accessed through the CMS Enterprise Portal.1 You will need an Identity and Access Management account before you can open an application. From there, select Individual Practitioner as your enrollment type and choose Nurse Practitioner as your provider type.3
The application walks through several sections: personal information, state licenses, practice locations, specialties, education, work history, malpractice coverage, billing and EFT details, and adverse legal actions.4 Your Medicare Administrative Contractor is assigned automatically based on your state and practice location, so you do not need to choose one.5 Once submitted, applications with an electronic signature typically process faster than paper alternatives, often within approximately two weeks.4
One point NPs frequently overlook: you need to enroll in two distinct capacities. Enrolling as a rendering provider lets you bill for services you personally perform. Enrolling as an ordering and referring provider lets you order labs, imaging, and referrals that Medicare will honor. Both enrollments are necessary for fully independent practice. You can track your application status using your Enrollment ID or Web Tracking ID.3
Annual Wellness Visits and Preventive Coding
Once enrolled, NPs functioning as primary care nurse practitioners can independently bill the Annual Wellness Visit codes that represent some of the highest-volume preventive services in primary care. G0438 covers the initial Annual Wellness Visit for a Medicare beneficiary who has been enrolled in Part B for more than twelve months. G0439 covers all subsequent Annual Wellness Visits. Neither code requires a physician to bill under their NPI, so NPs capture the full available reimbursement directly.
The 85% Payment Rule in Practice
When an NP bills under their own NPI, Medicare applies an 85% payment rate relative to the physician fee schedule. If Medicare allows $150 for a 99214 billed by a physician, the same service billed by an NP under their own number yields $127.50. That $22.50 gap per visit matters when you multiply it across a full panel. Understanding this arithmetic helps NPs negotiate compensation arrangements and evaluate whether incident-to billing, when permissible, changes the revenue picture for their practice.
Modifier -25 and Same-Day Visits
A common scenario in primary care: a patient comes in for their Annual Wellness Visit and also presents with a new or worsening problem that requires a separately documented evaluation. You can bill both the AWV and an E/M code on the same date, but Medicare requires modifier -25 appended to the E/M code to signal that the problem-oriented visit was significant and separately identifiable from the preventive service. The documentation must clearly support both services as distinct encounters within that visit. Bundling them into a single note without modifier -25, or using the modifier without the supporting documentation, are two of the more common triggers for claim denial and audit review.
Related Articles
Private Payer and Commercial Insurance Billing for NPs
The landscape of private payer reimbursement for nurse practitioners is shifting, but the pace of change varies dramatically depending on the insurer and the state where you practice. Understanding where each major commercial plan stands on NP credentialing and payment rates is essential for protecting your revenue and advocating effectively within your practice.
How Major Insurers Handle NP Reimbursement
Most large commercial insurers, including UnitedHealthcare, Aetna, Cigna, and Blue Cross Blue Shield plans, credential nurse practitioners as participating providers. However, reimbursement rates differ. Many private payers reimburse NPs at 85 percent of the physician fee schedule, mirroring the traditional Medicare rate, though some plans negotiate individually with practices and may offer different terms. Policies can also vary across regional BCBS affiliates, so a Blue Cross plan in one state may handle NP billing differently than one in another.
To find current reimbursement and credentialing details for a specific payer, check the commercial insurance section of each insurer's provider portal. If the information is not published there, call the payer's provider relations department directly. Keep a log of what you learn, because these policies change and written confirmation is always more reliable than a phone conversation alone.
State Payment Parity Laws
As of 2025 and into 2026, only a small number of states have enacted NP payment parity laws that require commercial insurers to reimburse nurse practitioners at the same rate as physicians for equivalent services. Oregon and Washington are among the most notable examples. In most other states, payers retain the discretion to set NP reimbursement below physician rates.
To check whether your state has a parity law in effect or pending legislation, review resources from the National Conference of State Legislatures or your state board of nursing. The American Association of Nurse Practitioners also maintains a regularly updated resource page that tracks payer reimbursement policies and state legislative developments. Bookmarking that page and checking it at least quarterly will keep you ahead of changes that directly affect your income.
Using Wage Benchmarks in Context
Bureau of Labor Statistics data on nurse practitioner wages can provide a useful baseline when evaluating whether your compensation reflects market norms. However, BLS figures aggregate earnings across all practice settings and specialties. They do not break down compensation by payer type or reflect whether a given state enforces payment parity for commercial plans. Use these numbers as a general reference point, not as evidence of what any single insurer should be paying.
Practical Steps for NPs in Private Payer Billing
- Verify your credentials annually: Confirm that each payer has your current NPI, specialty designation, and practice address on file. Credentialing lapses are a common cause of claim denials.
- Request fee schedules in writing: When joining a network, ask for the NP-specific fee schedule rather than assuming it matches physician rates.
- Track parity legislation: If your state is considering a parity bill, engagement through your professional association can make a real difference. For concrete strategies on shaping health policy, explore our nurse practitioner health policy toolkit.
- Document thoroughly: Private payers audit NP claims just as aggressively as Medicare. Ensure every visit note supports the code billed, regardless of the insurer.
Staying informed about each payer's policies takes effort, but it is one of the most direct ways to ensure you are compensated fairly for the care you provide. This is especially true for primary care nurse practitioners, who often carry the largest volume of billable visits in a practice.
Questions to Ask Yourself
Telehealth Billing for Nurse Practitioners in Primary Care
Telehealth is now a permanent part of primary care, but the billing rules sit on a shifting foundation of temporary congressional extensions and payer-specific quirks. As an NP, you are an authorized distant-site practitioner under Medicare, which means you can bill telehealth visits in your own name.1 The trick is matching the correct place-of-service (POS) code, modifier, and visit type to each encounter.
Place-of-Service Codes: 10 vs 02
For most primary care telehealth visits, the patient is at home, which means POS 10 (Telehealth Provided in Patient's Home). This code triggers the non-facility payment rate, which is what you want, since the non-facility rate is generally higher and reflects the practice expense of running the visit from your office.1 POS 02 (Telehealth Provided Other than in Patient's Home) is used when the patient is at a clinic, facility, or other non-home location, and it pays at the facility rate.2 Choosing the wrong POS is one of the most common telehealth coding errors and a frequent target in payer audits.
Modifiers and Audio-Only Visits
For a standard video visit with Medicare, no modifier is required when you use the correct telehealth POS.1 Many commercial payers, however, still require modifier 95 (synchronous telemedicine via audiovisual system), and a few legacy contracts may ask for modifier GT. Verify each payer's policy before submitting.
For audio-only visits, append modifier 93 to your E/M code.3 CMS continues to allow audio-only E/M billing for medical (non-behavioral) primary care visits through December 31, 2027.4 After that date, current law restricts audio-only telehealth to behavioral health, unless Congress acts again. The older telephone E/M codes (99441 to 99443) were retired, so route audio-only encounters through the standard office or other outpatient E/M codes (99202 to 99215) with modifier 93.
Post-PHE Policy Status
Congress has extended, but not made permanent, most of the pandemic-era flexibilities for non-behavioral telehealth. Geographic and originating-site restrictions remain waived through December 31, 2027, so patients can still be seen at home anywhere in the country.1 Behavioral health is the exception: originating-site flexibility and the removal of frequency limits are permanent.2 If legislative advocacy interests you, learning how nurse practitioners get involved in politics can help you push for permanent telehealth reform.
State-level rules add another layer. Coverage parity (requiring commercial plans to cover telehealth) is now common, while payment parity (requiring equal reimbursement for telehealth and in-person care) exists in only about half of states.5 Always confirm both Medicare rules and your state's parity law before assuming a visit will be paid at the in-person rate.
Common NP Billing Denials, Audit Risks, and How to Avoid Them
The top cause of Medicare Part B claim rejections for nurse practitioners in 2025 is the NP not being internally associated with the billing provider in the payer's system, a credentialing issue that accounts for more denials than any clinical documentation problem.1 Understanding the landscape of denials, audit triggers, and self-monitoring strategies is essential for protecting your reimbursement and maintaining compliance.
Top Five Denial Reasons for NP Claims
Nurse practitioner claims face a handful of recurring denial scenarios, each tied to a specific error pattern:
- Credentialing gaps: Your NPI may be enrolled with Medicare but not linked to the billing Tax ID or group practice in the MAC's records, resulting in immediate rejection.1
- Incorrect rendering provider: Claims billed under a physician NPI when you delivered the service, or vice versa, trigger CO-4 modifier inconsistency denials.2
- Incident-to documentation shortfalls: Missing supervision logs or failure to document the physician's initial visit and ongoing direct supervision generate medical necessity denials (CO-97) during post-payment audits.2
- Modifier errors: Omitting modifier -25 when billing an E/M visit and a minor procedure on the same day, or using modifier -59 inappropriately, leads to bundling denials and potential audit flags.
- Medical necessity insufficiency: Vague or incomplete documentation that does not support the level of service billed results in CO-97 denials, particularly for high-level codes like 99215.2
Other frequent denial codes include CO-11 for diagnosis mismatches, CO-16 for incomplete claim information, CO-18 for duplicate services, and CO-252 when required documentation is missing from the claim or medical record.2 Medicare Advantage plans denied 18 percent of claims in 2023 that actually met Medicare coverage rules, underscoring the importance of thorough appeals.3
OIG Audit Red Flags
The Office of Inspector General monitors several patterns in NP billing:
- Upcoding patterns: A practice where the majority of E/M visits are coded as 99215 raises immediate scrutiny, since national benchmarks show most primary care encounters fall into mid-level codes.
- Same-day service stacking: Billing an E/M visit and a procedure without proper modifier -25 documentation to justify the separately identifiable evaluation triggers audits.
- Services outside scope of practice: Billing for procedures or specialty services not permitted under state law for NPs without physician collaboration creates fraud risk.
NPs who serve as primary care nurse practitioners should pay particular attention to E/M distribution benchmarks, because primary care practices tend to draw the most scrutiny for upcoding.
Quarterly Self-Audit Checklist
Review these items every three months to catch errors before payers do:
- Verify your NPI is active and correctly linked to every billing Tax ID and payer contract.
- Run a report of your E/M code distribution and compare it to national benchmarks (most primary care should cluster around 99213 and 99214).
- Confirm incident-to supervision logs are documented for every visit billed under that mechanism.
- Audit a random sample of claims for correct modifiers, especially -25 and -59.
- Check that diagnosis codes support the level of service and procedure billed.
- Review all denied claims from the previous quarter and identify patterns.
- Ensure place-of-service codes match where care was actually delivered (incorrect POS is a top rejection reason for CPT 99309 claims).1
Appealing Denied Claims: One Actionable Tip
When filing a redetermination (you have 120 days from the denial notice), always reference the specific payer policy number or CMS manual section that supports your claim, not just clinical justification.4 For example, cite the CMS Internet-Only Manual section 240.2 when appealing an incident-to denial, or reference the Medicare Claims Processing Manual Chapter 12 for E/M modifier rules. Payers are more likely to overturn denials when you demonstrate policy compliance, not simply clinical rationale.
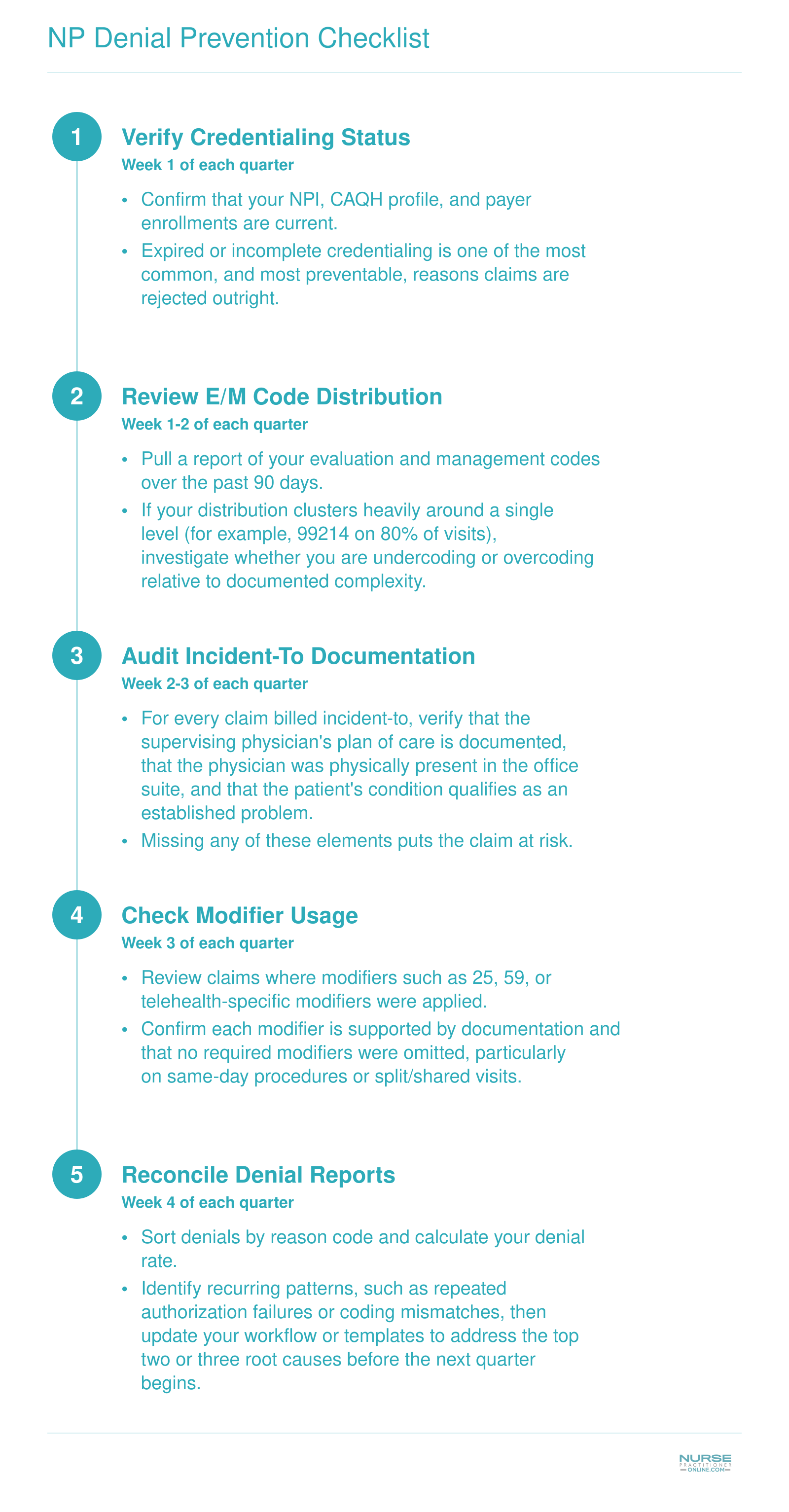
NP Denial Prevention Checklist
Running a quarterly self-audit helps you catch billing errors before they become costly denials or audit flags. This five-step workflow is designed so you can implement it immediately and repeat it every quarter to keep your claims clean.
NP Salary and Career Impact of Billing Proficiency
Nurse practitioners earn a strong national median salary, but those who master billing and coding position themselves to push well beyond the midpoint. According to the Bureau of Labor Statistics, the national median salary for NPs is $129,210, while NPs at the 75th percentile earn $149,570 or more. Billing fluency is one of the key differentiators that can help you reach that upper tier. NPs who understand primary care billing and coding generate more revenue for their practices by reducing claim denials, coding visits accurately, and maximizing appropriate reimbursement. That measurable contribution to the bottom line strengthens your negotiating position when it comes to salary reviews, performance bonuses, and leadership roles. In states with full practice authority, NPs often enjoy both higher reimbursement rates and greater compensation, because they can bill independently without physician oversight. If you are exploring ways to advance your earning potential, investing in billing expertise is one of the most practical steps you can take.
| Salary Benchmark | Annual Earnings |
|---|---|
| 25th Percentile | $109,940 |
| National Median (50th Percentile) | $129,210 |
| 75th Percentile | $149,570 |
| National Mean | $132,000 |
Highest-Paying States for Nurse Practitioners
The table below ranks the top 10 states by median annual salary for nurse practitioners, based on the most recent Bureau of Labor Statistics data. Notice that several of the highest-paying states, including California, Oregon, Washington, New Mexico, Connecticut, and Alaska, are full-practice-authority states where NPs can evaluate, diagnose, and treat patients without physician oversight. That overlap is no coincidence: when NPs bill independently under their own NPI, they capture the full reimbursement for their services, reinforcing the direct link between billing autonomy and higher earnings.
| Rank | State | Median Annual Salary | Total Employment |
|---|---|---|---|
| 1 | California | $166,610 | 20,980 |
| 2 | New Jersey | $149,620 | 9,590 |
| 3 | Alaska | $145,450 | 570 |
| 4 | New York | $145,390 | 20,430 |
| 5 | Oregon | $144,600 | 2,430 |
| 6 | Washington | $140,220 | 4,790 |
| 7 | Connecticut | $138,960 | 3,680 |
| 8 | Massachusetts | $138,890 | 8,920 |
| 9 | New Mexico | $138,440 | 1,870 |
| 10 | Arizona | $133,790 | 7,540 |
Frequently Asked Questions About NP Billing and Coding
Billing and coding questions come up constantly for nurse practitioners working in primary care. Below are straightforward answers to the questions NPs ask most often, with specific codes and rules referenced where applicable.
- Can nurse practitioners bill Medicare independently?
- Yes. Nurse practitioners who hold a National Provider Identifier (NPI) and are enrolled in the Medicare program can bill Medicare directly under their own NPI. When billing independently, NPs are reimbursed at 85% of the Medicare Physician Fee Schedule rate. Independent billing does not require physician oversight, though your state's scope of practice laws must still permit the services you provide.
- What is the difference between incident-to billing and direct billing for NPs?
- With direct billing, the NP bills under their own NPI and receives 85% of the physician rate. With incident-to billing, the NP's services are billed under a supervising physician's NPI at 100% of the physician rate. Incident-to billing requires that the physician initiated the plan of care, remains on site during the visit, and that the patient is established. It does not apply in hospital or facility settings.
- How much less do nurse practitioners get reimbursed compared to physicians?
- Under Medicare, NPs who bill independently receive 85% of the Medicare Physician Fee Schedule amount, which translates to a 15% reduction compared to physician reimbursement. Private payers set their own rates and policies. Some commercial insurers reimburse NPs at the same rate as physicians, while others apply varying discounts. Always verify each payer's reimbursement schedule in your contract.
- What E/M codes do nurse practitioners use for office visits?
- NPs use the same Evaluation and Management (E/M) codes as physicians. For established patient office visits, the most common codes are 99211 through 99215. For new patient visits, the range is 99202 through 99205. Code selection is based on the level of medical decision making or total time spent on the encounter, following the current AMA CPT guidelines updated in 2023.
- Can nurse practitioners bill for telehealth visits?
- Yes. NPs can bill for telehealth visits using the same E/M codes they would use for in-person encounters, along with the appropriate place of service code and modifier 95 (or the modifier required by the specific payer). Medicare covers a range of NP telehealth services, though eligible originating sites and geographic restrictions can change. Always check the latest CMS telehealth services list for current coverage rules.
- Do NP billing rules differ between Medicare and private insurance?
- They do. Medicare has standardized rules, including the 85% reimbursement rate for NPs and specific incident-to requirements. Private insurers establish their own credentialing processes, fee schedules, and billing guidelines. Some commercial plans credential NPs the same as physicians, while others restrict certain billing privileges. Review each payer contract carefully and contact the payer's provider relations team with questions.
- Does my state's scope-of-practice law affect how I can bill?
- Absolutely. States fall into three categories: full practice authority, reduced practice, and restricted practice. In full practice authority states, NPs can bill for a broader range of services without a collaborative agreement. In states requiring physician supervision or collaboration, your billing options may be limited, particularly for incident-to billing arrangements. Always confirm that your clinical services align with your state's nurse practice act before submitting claims.