Most important takeaways…
- NP employment is projected to grow 40% between 2024 and 2034, making policy engagement more urgent than ever.
- A structured seven step toolkit moves you from passive awareness to drafting testimony and meeting legislators.
- Between 2022 and 2026, NP coalitions secured multiple state victories expanding full practice authority and reimbursement parity.
- States with full practice authority, such as Oregon, tend to show stronger NP salary and employment figures.
Nurse practitioners write more than one billion prescriptions annually and serve as the primary care provider for roughly a quarter of rural Americans, yet fewer than 10 of the 535 members of Congress hold a nursing credential of any kind. The people closest to patient care are largely absent from the rooms where Medicaid reimbursement, scope of practice, and prescriptive authority get decided.
That gap is not an accident. Clinical schedules, the cost of advocacy time, and a training culture that treats policy as someone else's job all push NPs toward the exam room and away from the statehouse. The practical question is not whether nurses belong in politics. It is how a working clinician finds 30 useful minutes a month to move the needle. This seven-step toolkit gives you a structured plan to do exactly that, from mapping your policy landscape to contacting legislators, testifying at hearings, and building a sustainable advocacy habit you can maintain alongside your clinical career.
Why Nurse Practitioners Must Have a Seat at the Policy Table
The Bureau of Labor Statistics projects 40% job growth for nurse practitioners between 2024 and 2034, a rate that dwarfs nearly every other occupation in the country.1 At the same time, the Association of American Medical Colleges estimates the United States will face a shortage of up to 86,000 physicians by 2036, with primary care alone accounting for a gap of 20,200 to 40,400 providers.2 NPs are already stepping in to fill that void, yet the policy framework governing their practice has not kept pace with the reality on the ground.
The Direct Line Between Policy and Patient Access
Scope-of-practice laws, prescriptive authority rules, and Medicaid reimbursement rates are not abstract bureaucratic details. They determine, in concrete terms, who receives care and who does not. In full practice authority states, NPs can evaluate patients, diagnose conditions, and prescribe medications without physician oversight. In restricted-practice states, collaborative agreements or supervisory requirements create bottlenecks that limit the number of NPs who can practice independently, particularly in underserved areas.
Consider rural communities, where roughly 75 million Americans already lack adequate access to primary care.2 In full practice authority states, NPs can open clinics, accept patients, and deliver the same evidence-based care a physician would. In restricted states, an NP who wants to serve a remote community may be unable to find a collaborating physician within a reasonable distance, leaving patients without a provider at all. The policy difference is not theoretical; it translates directly into appointment wait times, emergency room overcrowding, and preventable hospitalizations. This is precisely why so many communities now rely on a nurse practitioner as a primary care provider.
If You Don't Shape the Rules, Someone Less Informed Will
Why should nurses be involved in politics? Because every legislative session, people who have never administered a medication, triaged a patient, or managed a panel of chronically ill adults make decisions that dictate how you practice. Lobbyists, insurers, and competing professional organizations all have seats at the table. When NPs are absent from that conversation, the resulting policies reflect someone else's priorities, not the clinical reality you navigate every shift.
Political engagement is not optional for a profession growing this fast. With NP ranks expanding at such a dramatic pace, the gap between workforce capacity and legal authority will only widen unless practitioners themselves push for change. Advocacy is a professional responsibility on par with staying current on clinical guidelines. The toolkit in this article is designed to make that work manageable, even if you have never contacted a legislator before.
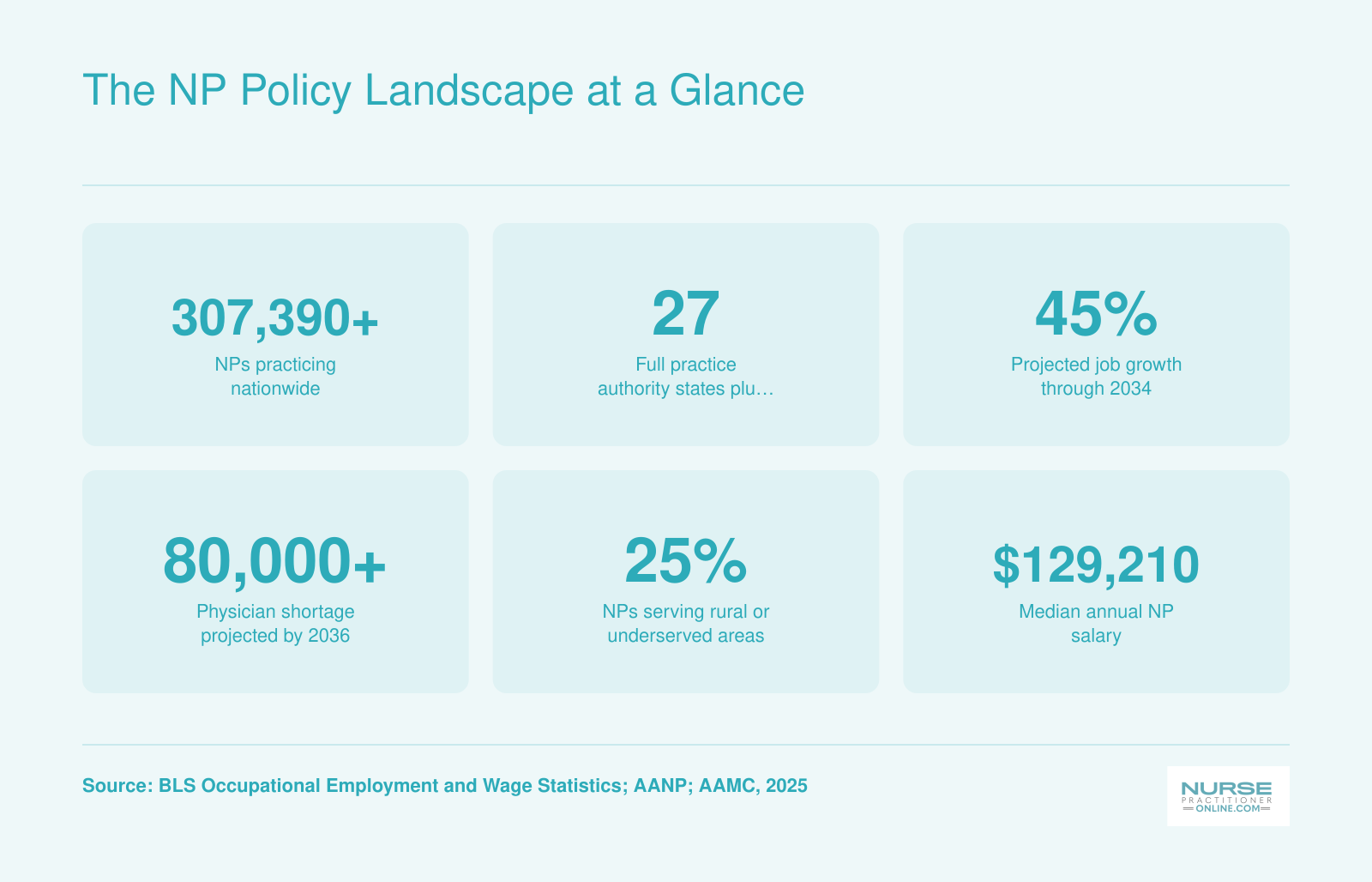
The NP Policy Landscape at a Glance
These numbers tell a clear story: nurse practitioners are a fast-growing workforce stepping into critical gaps in American healthcare, yet policy barriers still limit their impact in many states. Understanding the landscape is the first step toward changing it.
Barriers That Keep NPs Out of Politics, and How to Overcome Them
What actually stops nurse practitioners from engaging in health policy, and how can you push past those obstacles without sacrificing your clinical career or personal life?
The barriers are real, but none of them are insurmountable. Understanding exactly what holds NPs back from political engagement is the first step toward dismantling those obstacles one by one.
Time Constraints and Shift Work
Working 12-hour shifts, rotating schedules, and managing patient loads leaves little energy for anything beyond recovery. The solution is not to carve out hours you do not have. Instead, embrace micro-advocacy. A 10-minute phone call to a legislative aide during your lunch break counts. Sending a pre-written email template to your state representative before bed counts. Signing onto a coalition letter drafted by your professional organization counts. Advocacy does not require attending every town hall or testifying at the statehouse. Small, consistent actions accumulate into meaningful influence.
Knowledge Gaps About the Legislative Process
Many NPs feel unprepared because nursing education rarely covers how bills become laws or how to navigate committee structures. This gap closes quickly with targeted resources. Your state nurses association likely offers policy primers and advocacy training. Organizations like the American Association of Nurse Practitioners provide webinars explaining legislative processes in plain language. You do not need a political science degree. You need a basic understanding of who makes decisions, when they make them, and how to reach them at the right moment.
Fear of Overstepping Professional Boundaries
Some NPs worry that political involvement crosses into territory that nurses should avoid. This concern deserves a direct response: advocacy is explicitly within your ethical scope. The American Nurses Association Code of Ethics, Provision 9, establishes that nurses must work to shape social policy and address social determinants of health. Speaking up for patients, communities, and the profession is not overstepping. It is fulfilling your professional obligation.
Employer Restrictions and Workplace Culture
Certain healthcare systems discourage or prohibit staff from lobbying on the clock or using institutional affiliation in political communications. The workaround is straightforward: separate your personal advocacy from your employer. Contact legislators as a constituent and licensed NP, not as a representative of your workplace. Join professional associations that lobby on your behalf without requiring you to take public stances that might conflict with employment policies.
Feeling Like One Voice Cannot Matter
Legislators receive thousands of communications, so why would yours make a difference? Here is the reality: most constituents never contact their representatives at all. A thoughtful, personal message from a healthcare professional who treats patients in that district carries significant weight. Legislative staffers track constituent feedback, and elected officials notice when multiple nurses from the same area raise the same concern. Your single voice, combined with others, becomes impossible to ignore. This collective power is exactly how NPs have successfully advocated for issues like DNP entry-to-practice requirements and expanded scope of practice.
The Real Risk Is Inaction
Every barrier listed above has a practical solution, but none of those solutions matter if NPs stay on the sidelines. The greatest risk is not overreach or embarrassment or wasted effort. The greatest risk is allowing people who do not understand frontline care to make decisions that affect your patients, your practice, and your profession. The seat at the policy table exists. The only question is whether you choose to fill it.
Step-By-Step: The 7-Part NP Health Policy Toolkit
Passive awareness versus active engagement: most nurse practitioners recognize that policy shapes their daily practice, but far fewer have a structured plan to influence those decisions. This seven-step toolkit transforms you from a spectator into an informed advocate, building from foundational knowledge to concrete action. Each step equips you with the tools, language, and confidence to shape the health policy conversations that determine how you serve your patients.
Step 1: Know Your Policy Landscape
Start by understanding the three tiers of nurse practitioner practice authority by state. Full practice authority (FPA) states allow NPs to evaluate, diagnose, order tests, and prescribe medications without physician oversight or collaboration agreements. Reduced practice authority states require some level of collaboration, supervision, or team agreement with a physician. Restricted practice states mandate physician supervision for diagnosis and prescriptive authority.
As of May 2026, thirty states and territories grant full practice authority, fifteen operate under reduced practice, and eleven maintain restricted practice environments.1 These categories directly affect where you can work, how quickly you can open a practice after graduation, and whether you need to pay for ongoing collaborative agreements.
Check your state's current status using the American Association of Nurse Practitioners (AANP) practice environment map, which updates as legislation passes. If you practice in New York, you enjoy full practice authority. Illinois colleagues work under reduced practice rules. California and South Carolina maintain restricted environments, though South Carolina has introduced S.3580 during the 2025-2026 legislative session to expand FPA.2 Knowing your baseline helps you spot opportunities for change.
Step 2: Identify Your Priority Issues
Policy covers dozens of issues beyond practice authority. Focus your initial advocacy energy on one or two topics where your clinical expertise and patient population intersect. Family NPs in rural areas might prioritize telehealth reimbursement parity and broadband access. Psychiatric-mental health NPs often advocate for mental health parity laws and funding for community behavioral health centers. If you serve Medicaid-heavy populations, payment reform and eligibility rules directly affect your practice viability. Exploring different nurse practitioner specialties can help you pinpoint where your clinical focus and policy priorities overlap.
Choose issues where your voice carries authentic weight. Legislators value testimony rooted in real patient stories, not abstract policy theory. When you can explain how a specific regulation delays care for your diabetic patients or forces families to drive two hours for mental health visits, you become a credible, persuasive witness.
Step 3: Find Your Legislators and Their Positions
Identify your state senator, state representative, U.S. senator, and U.S. representative by entering your home address into your state legislature's website and Congress.gov. Write down their names, district office phone numbers, and email addresses.
Next, determine which legislators sit on health committees. State health and human services committees hear scope-of-practice bills. Appropriations committees control Medicaid funding. At the federal level, the Senate Health, Education, Labor, and Pensions (HELP) Committee and the House Energy and Commerce Committee oversee most health legislation.
Review recent voting records on bills affecting NPs. Most state legislatures publish bill histories showing who voted yes, no, or abstained. If your representative voted against an FPA expansion bill two years ago, you need a different approach than if they sponsored it. Understanding their track record prevents wasted effort and helps you tailor your message.
Step 4: Join Professional Advocacy Organizations
Individual voices matter, but organized advocacy moves legislation. The American Association of Nurse Practitioners provides federal lobby days, tracks every state bill affecting NP practice, and sends legislative alerts when critical votes approach. Membership unlocks access to the AANP political action committee (PAC), sample testimony, and talking points drafted by policy staff who monitor Capitol Hill daily.
Join your state nurse practitioner association as well. State groups often have stronger relationships with local legislators and can arrange in-district meetings faster than national organizations. Specialty organizations like the National Association of Pediatric Nurse Practitioners or the American Association of Critical-Care Nurses offer policy resources tailored to your practice area.
Membership fees range from fifty to three hundred dollars annually, but most organizations offer reduced rates for new graduates. The return on investment appears quickly when you receive a bill alert about legislation that would have blindsided you otherwise, or when you attend a lobby day and secure a fifteen-minute meeting with your state senator.
State-By-State NP Practice Authority Status
NP practice authority simply means what a nurse practitioner is legally allowed to do without a supervising physician. States fall into three categories: full practice (NPs can evaluate, diagnose, treat, and prescribe independently), reduced practice (NPs need a collaborative agreement for at least one element of practice), and restricted practice (NPs must have physician supervision or delegation for most patient care). Knowing your state's status is the starting point for any advocacy effort. For a detailed breakdown, see our guide to nurse practitioner practice authority by state.
The AANP Interactive State Map
- Live data: The American Association of Nurse Practitioners (AANP) hosts an interactive map on their website that color-codes each state as full, reduced, or restricted practice. It is updated regularly and reflects the most recent legislative changes.
- Quick reference: Hover over any state to see a summary of its practice environment, including whether NPs need a collaborative agreement, the level of prescriptive authority, and any recent milestones.
- Advocacy fuel: Use this map to compare your state to neighbors or to illustrate the nationwide patchwork when talking to lawmakers.
Barton Associates' State-by-State Breakdown
- Legislative tracking: Barton Associates maintains a page that not only lists each state's current status but also tracks pending bills from the 2025-2026 legislative sessions. This is especially valuable at the start of a new year when multiple states are considering practice authority changes.
- Concise summaries: Each state entry includes a short narrative of what the law allows and highlights upcoming hearings or floor votes. If a state is on the cusp of moving from reduced to full practice, you will find the bill number and status here.
- Practical use: Bookmark this resource and check it before any meeting with a legislator so you can reference the most recent developments.
Your State Board of Nursing and Legislature Websites
- Official source: For the most authoritative information, go directly to your state board of nursing. They publish the statutes and administrative rules that define NP scope of practice. Look for a "Practice Act" or "Scope of Practice" section.
- Real-time bills: Pair that with your state legislature's bill search tool. Enter keywords like "nurse practitioner," "full practice authority," or "collaborative agreement" to see introduced legislation, committee assignments, and voting records.
- Why it matters: Cross-referencing these sources ensures you are not relying on outdated third-party summaries when a bill has already been signed into law.
Employment Data as a Policy Mirror
- BLS.gov insights: The Bureau of Labor Statistics (BLS) provides state-level employment numbers and wages for nurse practitioners. While it does not directly label practice authority, patterns often emerge: states with longer-standing full practice authority tend to show higher NP employment per capita in primary care and rural areas.
- Making the case: When advocating for change, pairing employment data with the AANP practice status can help you argue that full practice authority expands access to care without sacrificing safety. Understanding nurse practitioner licensing requirements in your state adds another layer of credibility to your argument.
Remember, no single source gives you the complete picture. Triangulate between the AANP map, Barton Associates' legislative tracker, official state sites, and BLS employment data to stay reliably informed about where your state stands and where it is headed.
Your Toolkit Continued: Steps 5–7
How do I actually reach a legislator in a way they'll remember, and what do I say in under a minute? That's the nuts-and-bolts question most nurse practitioners ask when they move from policy interest to action. The final three steps of this toolkit turn intent into impact, starting with direct contact, moving to public testimony, and ending with a sustainable advocacy rhythm.
Step 5: Contact Your Legislators
Not all outreach carries equal weight. The hierarchy of impact is clear: an in-person meeting at the district office or state capitol lands hardest, followed by a phone call, then a personalized email, and finally a form letter or petition signature. A five-minute face-to-face chat, especially if you bring a local perspective, can shift a lawmaker's stance more than a hundred generic emails. When scheduling, target the weeks just before key committee votes, during the legislative session, or use district office hours when lawmakers are home and less rushed.
- Before you call: identify one specific bill by number and know whether you support or oppose it.
- During the call: share your name, town, and role as a nurse practitioner, then state your position and one sentence about real-world impact.
- End with: a polite ask for the legislator's support, and offer to provide more information if needed.
The templates section coming up gives you exact scripts, so you never have to guess what to say.
The 30-Second Rule: Make the Call Count
Most legislative staffers answer the phone, log your name, position, and bill number in under 30 seconds. You don't need to be a policy expert or a polished debater. You simply need to call and clearly register your stance. Staff tally constituent contacts daily, and a surge of calls on a specific bill can stop a hearing or flip a vote. Your voice matters more than your talking points.
Step 6: Testify and Show Up
Public comment at state hearings gives nurse practitioners a powerful, real-time platform. Start by checking your state legislature's website for upcoming committee hearings on health policy bills. Look for a "public testimony" or "register to speak" link. A two-minute testimony should follow a simple structure: introduce yourself by name and credentials, state your position, share one data point or personal story, and end with a clear ask. Practice it out loud with a timer.
Leave behind a one-page fact sheet. Keep it to bullet points: who you are, the bill number, three key facts with sources, and your contact information. Hand it to the committee clerk before you speak. Even if you never get called on, your physical presence and that sheet signal that NPs are paying attention.
Step 7: Build a Long-Term Advocacy Habit
View advocacy as an ongoing professional practice, not a one-time reaction to a crisis. Design a quarterly rhythm that you can maintain alongside clinical work. Here is a realistic starting calendar:
- Quarter 1: attend one legislative hearing or public meeting in your state.
- Quarter 2: make one direct contact (call, meeting, or personalized email) with your legislator or their staff.
- Quarter 3: post one social media message tagging your legislator about an NP priority, with a professional, respectful tone.
- Quarter 4: co-sign a sign-on letter led by your state NP association, amplifying your voice without reinventing the wheel.
This cadence makes advocacy manageable. Over time, you'll feel less like an outsider and more like a trusted resource lawmakers recognize. And when a bill critical to your practice comes up, you'll already have the relationships and habits in place to mobilize quickly.
Templates and Scripts for Contacting Legislators
The biggest mistake NPs make when reaching out to legislators is defaulting to the easiest path: copying and pasting a generic form letter. Personalized communication takes more time, but it's the only kind that genuinely shifts votes. When you connect a real patient story to a specific policy ask, you turn an abstract bill into a human imperative. Below are ready-to-adapt tools that make personalizing quick and repeatable.
Email Template for Legislators
Subject: Please support [bill number] to improve patient access in [your city/county]
Dear [Representative / Senator] [Last name],
I am a nurse practitioner in [city or district], and I am writing to ask you to vote yes on [bill number], which [briefly state what the bill would do, e.g. removes outdated physician supervision requirements].
Last month, I cared for a patient [insert brief, de-identified story, e.g. who drove over 100 miles to see me because no NP in his rural town could prescribe his maintenance medications independently]. Current law means [explain the concrete barrier your patient faced]. Passing [bill number] would directly allow NPs like me to [state the improved outcome, e.g. manage that condition locally, saving travel and cost].
I urge you to support [bill number] and strengthen our healthcare workforce. Thank you for your time, and I am happy to provide more clinical context.
Sincerely, [Your name], APRN [Your practice city, state]
Phone Call Script (30 Seconds)
When you call, you will likely speak to a staffer. Be polite and concise.
Introduction: "Hello, my name is [name], and I'm a nurse practitioner in [city/town]. May I leave a brief message for [Representative / Senator] [Last name]?"
Issue: "I'm calling about [bill number], which addresses [briefly, e.g. outdated barriers that limit patient access to NP care]. Right now, [one-sentence problem, e.g. many patients in our area must wait weeks for primary care appointments because state law limits what NPs can do without a physician contract]."
Ask: "Please ask [Representative / Senator] to vote yes on [bill number]. This would [direct patient benefit, e.g. let me order home health services for my bedbound patients without a duplicative physician sign-off, getting them care faster]."
Thank you: "Thank you for your time and for all your office does."
Testimony Outline for a 2-Minute Hearing Statement
Hearings often limit public testimony to two minutes. Hit these beats:
- Hook (15 seconds): "Chair [Name] and members of the committee, my name is [name], and I've been a family nurse practitioner for [X] years. I treat patients in [community type, rural, urban, underserved] every day, and I'm here to tell you how [bill number] directly affects their lives."
- Credentials (15 seconds): One sentence on your training and experience: "I hold national board certification and a graduate degree from [university]; I've managed [X number] patient visits per year."
- Patient impact story (45 seconds): Describe one de-identified patient case illustrating the barrier: "Take my patient 'Maria,' a 67-year-old with diabetes and heart failure. Because current law requires a collaborative practice agreement, I could adjust her insulin and diuretics, but when her physician partner retired, I had to stop, and Maria ended up in the ER with fluid overload."
- Specific policy ask (30 seconds): "I urge you to pass [bill number]. This legislation allows NPs to practice to the full scope of our education and national certification, eliminating delays and keeping patients like Maria safe and stable at home."
- Closing (15 seconds): "Thank you for your consideration. I'm happy to answer any questions."
One-Page Leave-Behind Fact Sheet Outline
Design this for a single printed page you can hand to a staffer or legislator.
- Headline stat: A compelling, state-specific figure: "In [state], 28% of counties are primary care health professional shortage areas. NPs could fill the gap if allowed to practice to their full scope."
- 3 bullet points:
- Access: "Full practice authority is associated with a 16% increase in primary care utilization in underserved communities (Health Affairs)."
- Safety: "NPs have provided safe, high-quality care for over 50 years, and no state has reversed full practice authority due to safety concerns."
- Cost: "Eliminating duplicative oversight saves the state an estimated [local figure] annually in administrative costs."
- Call to action: "Please vote YES on [bill number] to remove outdated barriers and let nurse practitioners close the access gap."
- Your contact info: Name, credentials, clinic name, city, phone, email.
Although templates save time, their power multiplies when you anchor them in a real, de-identified patient encounter. If you are still exploring how to become a nurse practitioner, these advocacy skills will serve you well from day one. One vivid two-sentence story will outweigh a stack of generic postcards. Always ask: would this anecdote help a neighbor understand what's at stake? If yes, it's ready to use.
Key NP Policy Issues Beyond Full Practice Authority
Full practice authority gets most of the headlines, but the policy landscape affecting nurse practitioners is far broader. The real tradeoff every NP advocate faces is this: do you spread your energy across every issue, or do you go deep on one and actually move the needle? The answer is almost always the latter. Pick the issue that intersects your specialty, your patient population, and your state's current legislative calendar, then become the person lawmakers call when they have questions.
Here are five policy areas that deserve your attention in 2026, and that many advocacy guides overlook entirely.
Telehealth Prescribing and Reimbursement Parity
Telehealth expanded access to NP-delivered care dramatically, but the payment structure has not kept pace with the practice reality. As of late 2025, only 23 states had full telehealth payment parity, while 36 states plus Washington, D.C. had private payer parity laws in place.12 The gaps matter because reimbursement shortfalls mean NPs eat the cost or patients lose access. A federal Medicare telehealth waiver currently runs through December 31, 2027, and what happens after that is the biggest policy cliff facing telehealth NPs right now.34 New Jersey's parity law has a sunset date of July 1, 2026, making it a live legislative fight this year. New Mexico, by contrast, expanded its Telehealth Act in 2025, a model worth studying.5
Medicare and Medicaid Payment Equity
Medicare currently reimburses NPs at 85 percent of the physician fee schedule for identical services. That gap does not reflect a difference in quality. It reflects a policy choice, and it is one that organized NP advocacy has targeted as a federal priority going into 2026.6 Closing this gap would directly increase NP revenue, expand rural and underserved access, and align payment with scope of practice reality.
Mental Health Workforce Funding
The behavioral health workforce shortage creates a direct opening for psychiatric-mental health NPs. Two federal programs, the Behavioral Health Workforce Education and Training program and the National Health Service Corps, are active funding vehicles for 2025 to 2026.7 Advocacy that protects and expands these programs keeps pipeline funding flowing into NP training slots. If you work in behavioral health or plan to, this is your issue.
Maternal Health and Health Equity Legislation
NPs are explicitly recognized as maternal health providers in current federal funding frameworks.6 Bills targeting maternal mortality, especially among Black and Indigenous women, consistently include NP-delivered care as part of the solution. If maternal health aligns with your practice, exploring the path to becoming a women's health nurse practitioner can position you to lead in this space. Staying engaged with maternal health legislation keeps NPs in the room where funding and scope decisions get made.
Controlled Substance Prescribing Authority
In states where NPs still face restrictions on prescribing controlled substances, including Schedule II medications, the practical impact falls hardest on pain management and addiction medicine patients. State-level DEA registration requirements and prescriptive authority limits vary widely. AANP tracks active legislation on NP signature recognition and direct credentialing in multiple states, both of which affect how smoothly NPs can prescribe and bill without physician co-signature requirements.6
You do not need to champion all five of these areas. Choose the one that fits your practice setting, get credible on the facts, and show up consistently. That focused approach is what turns an interested NP into an effective advocate.
Case Studies: NP-Led Policy Wins That Changed the Rules
What specific policy victories have nurse practitioners actually won in state legislatures over the past four years, and how did they do it?
Between 2022 and 2026, nurse practitioners secured a string of legislative wins that expanded practice authority, improved reimbursement, and widened telehealth access across the United States. These victories were not accidents. They followed deliberate campaigns led by NP coalitions, state nursing associations, and individual advocates who testified, lobbied, and organized their colleagues. Studying these case studies reveals the strategies that work and the timelines you can expect when you flex your own political muscle.
Nevada: Full Practice Authority After a Decade of Advocacy
In January 2023, Nevada Governor Joe Lombardo signed SB 438, granting full practice authority to advanced practice registered nurses, including nurse practitioners. The Nevada Nurses Association and the Nevada State Board of Nursing led a 10-year campaign that included hundreds of hours of legislative testimony, coalition-building with rural health clinics, and data demonstrating that Nevada ranked 47th in primary care access. The bill passed both chambers with bipartisan support. By 2025, BLS data showed Nevada's NP workforce grew 18 percent year-over-year, one of the fastest rates in the nation, as newly autonomous NPs opened practices in underserved areas.
North Carolina: Telehealth Parity and Medicaid Reimbursement
In June 2024, North Carolina passed HB 149, which made pandemic-era telehealth flexibilities permanent and required Medicaid to reimburse NPs at the same rate as physicians for equivalent services. The North Carolina Nurses Association partnered with Duke University School of Nursing alumni and the state chapter of AANP to flood legislative inboxes with constituent letters and organize a virtual lobby day that drew over 500 participants. The bill's fiscal note projected $12 million in annual savings by shifting care from emergency departments to NP-led telehealth visits. State health department reports published in early 2025 confirmed a 22 percent increase in rural Medicaid beneficiaries receiving primary care within 30 days of enrollment.
Maryland: Prescriptive Authority Expansion
Maryland's HB 1214, signed in May 2022, removed the physician collaboration requirement for NPs with at least two years of clinical experience. The Maryland Nurses Association worked closely with the Johns Hopkins School of Nursing to provide economic impact data and testimony from practicing NPs. The campaign emphasized workforce shortages exacerbated by the COVID-19 pandemic. Legislative analysis published on the Maryland General Assembly website documented that the change would add an estimated 800 full-time-equivalent primary care nurse practitioner providers statewide by 2024.
How to Find and Verify These Wins Yourself
Start with AANP's State Policy Tracker, which posts real-time updates on pending and passed legislation in all 50 states. Cross-reference bill numbers and sponsors on your state legislature's website (search terms like "nurse practitioner full practice authority [state]" work well). For workforce impact, check BLS.gov's Occupational Employment and Wage Statistics database, filtering by state and year. University school of nursing news pages often profile alumni who led advocacy efforts. Finally, state health department annual reports and Medicaid program evaluations provide outcome data on access, cost, and quality after policy changes take effect.
How NP Salaries and Employment Vary by State, and Why Policy Matters
The table below highlights nurse practitioner salary and employment figures across 25 states and the District of Columbia, drawn from approximate 2024 Bureau of Labor Statistics data. Notice how many of the states with full practice authority (such as Oregon, Montana, New Mexico, Arizona, Colorado, and Minnesota) maintain competitive salaries while also employing significant numbers of NPs per capita. While salary is only one factor in career decisions, these numbers make the policy conversation personal: where NPs can practice independently, the workforce tends to grow, competition for talent increases, and compensation reflects that demand. Keep in mind that cost of living, population density, and local healthcare needs also shape these figures.
| State | Total NPs Employed | Median Annual Salary | 25th Percentile Salary | 75th Percentile Salary | Mean Annual Salary |
|---|---|---|---|---|---|
| California | 20,980 | $166,610 | $140,260 | $205,400 | $173,190 |
| New Jersey | 9,590 | $149,620 | $126,030 | $162,250 | $140,470 |
| Alaska | 570 | $145,450 | $104,000 | $165,510 | $142,340 |
| New York | 20,430 | $145,390 | $128,190 | $164,670 | $148,410 |
| Oregon | 2,430 | $144,600 | $129,840 | $163,240 | $148,030 |
| Washington | 4,790 | $140,220 | $125,890 | $161,730 | $143,620 |
| Connecticut | 3,680 | $138,960 | $125,910 | $159,680 | $141,140 |
| Massachusetts | 8,920 | $138,890 | $125,590 | $160,310 | $145,140 |
| New Mexico | 1,870 | $138,440 | $113,240 | $156,000 | $136,620 |
| Arizona | 7,540 | $133,790 | $115,290 | $151,650 | $132,920 |
| Montana | 1,050 | $133,640 | $112,180 | $141,050 | $131,560 |
| New Hampshire | 1,790 | $132,440 | $120,270 | $143,010 | $133,660 |
| District of Columbia | 790 | $131,380 | $119,240 | $143,960 | $137,600 |
| Hawaii | 470 | $130,940 | $121,410 | $158,100 | $135,020 |
| Rhode Island | 1,200 | $130,710 | $126,200 | $160,030 | $139,600 |
| Texas | 21,690 | $129,880 | $110,570 | $143,860 | $130,930 |
| Colorado | 4,130 | $129,750 | $110,300 | $139,440 | $127,610 |
| Vermont | 680 | $129,740 | $115,650 | $139,930 | $130,580 |
| Iowa | 2,810 | $129,420 | $115,950 | $137,900 | $133,020 |
| Florida | 24,690 | $129,010 | $109,670 | $143,670 | $128,340 |
| Idaho | 1,570 | $128,940 | $119,290 | $140,920 | $131,380 |
| Illinois | 9,560 | $128,620 | $111,450 | $138,420 | $128,880 |
| Wisconsin | 4,950 | $128,580 | $117,630 | $137,150 | $130,490 |
| Minnesota | 8,690 | $128,570 | $103,250 | $139,590 | $128,120 |
| Indiana | 7,470 | $128,280 | $111,210 | $134,840 | $126,520 |
From Advocate to Elected Official: Policy Career Pathways for NPs
Moving from writing letters and attending hearings to actually shaping policy from inside the system is the natural extension of everything in this toolkit. Think of it as the long game: Step 7 taken further for NPs who want to make advocacy their primary career, not just a professional obligation. Several concrete pathways can get you there, and each one builds on the advocacy skills you have already started developing.
Health Policy Fellowships
Fellowships immerse you in the mechanics of policymaking, from drafting legislation to analyzing regulatory impact, while connecting you with a network of like-minded health professionals. Here are programs that accept or specifically target nurse practitioners.
- AANP Health Policy Fellowship: Open to AANP members who hold an active NP license and national certification. You need demonstrated involvement in policy or advocacy. The program is part-time, making it feasible for working clinicians. Applications typically open in the fall.1
- National Academy of Medicine State Health Policy Fellowship: A full-time, residential program for mid-career health professionals with significant state-level leadership experience. NPs who have served in state leadership roles are eligible. Fellows work directly on state health policy priorities.2
- Health and Aging Policy Fellows Program: This 12-month program offers both residential and non-residential tracks and selects roughly 14 fellows per year. It is designed for clinicians, researchers, and leaders in health and aging. NPs who work with older adults are well-positioned applicants. Applications generally open in late winter or early spring.3
- GWU Fellowship in Health Policy and Media: A 12-month, non-residential, part-time fellowship open to healthcare professionals, policy analysts, and researchers. Its spring application deadline (March 14 for the 2025-2026 cohort) makes it easy to plan ahead.4
Fellows in these programs spend their time analyzing legislation, advising policymakers, publishing policy briefs, and building relationships on Capitol Hill or in state capitols. The experience translates directly into credibility when you pursue appointed or elected roles later.
Appointed Advisory Roles
You do not have to run a campaign to hold a policy position. State boards of nursing, Medicaid advisory committees, and federal panels such as those convened by CMS regularly seek clinician input. Governors appoint healthcare professionals to these bodies, and NPs who have been active in their state nursing associations or who have fellowship experience are strong candidates. These roles let you influence scope-of-practice regulations, reimbursement rules, and quality standards from inside the regulatory process. If you are still building your credentials, reviewing licensing and certification requirements can help you confirm that your qualifications are current before you apply.
Running for Office
NPs have won seats at the local and state level. Former Oregon state senator Laurie Monnes Anderson, a nurse practitioner, served in the state legislature for over a decade and championed healthcare access bills throughout her tenure. Former U.S. Representative Eddie Bernice Johnson of Texas, a registered nurse who advanced healthcare policy at the federal level for nearly 30 years, demonstrated how clinical expertise translates into legislative effectiveness. Their examples show that clinical credibility resonates with voters, especially in districts where healthcare access is a defining concern.
If elected office interests you, start local. School boards, city councils, and county health commissions are accessible entry points that let you build a campaign track record without leaving clinical practice entirely.
Putting It All Together
These pathways are not mutually exclusive. Many NPs complete a fellowship, serve on an advisory board, and then decide whether to pursue elected office. The sequence builds skills incrementally: policy analysis first, then governance experience, then public leadership. Whatever depth of involvement suits your career and life, the key takeaway is that the system has room for you, and it works better when nurse practitioners are inside it.
Frequently Asked Questions About NPs in Politics
Getting involved in health policy can feel unfamiliar, especially if your training focused squarely on clinical care. These answers address the most common questions nurse practitioners ask when they start flexing their political muscle.
- What is full practice authority for nurse practitioners?
- Full practice authority (FPA) allows nurse practitioners to evaluate patients, diagnose conditions, order tests, and prescribe medications, including controlled substances, without a collaborative or supervisory agreement with a physician. As of 2026, roughly half of U.S. states plus the District of Columbia grant FPA. The remaining states impose varying levels of oversight that can limit where and how NPs deliver care.
- How can nurse practitioners influence health policy at the state level?
- Start by identifying your state legislators who sit on health committees and schedule brief meetings or phone calls. Share concise, evidence-based talking points tied to patient outcomes. Testify at committee hearings, submit written comments on proposed rules, and join your state NP association's advocacy day. Consistent, relationship-driven outreach is far more effective than one-time contact.
- Is it appropriate for NPs to contact legislators while employed at a hospital or health system?
- Yes, but use personal time, personal email, and personal devices. Identify yourself as a constituent and a nurse practitioner rather than a representative of your employer. Most hospitals have policies separating institutional lobbying from individual advocacy. As long as you speak on your own behalf and on your own time, contacting legislators is both legal and encouraged.
- What are the most important NP policy issues in 2026?
- Key issues include expanding full practice authority in restricted and reduced-practice states, securing equitable reimbursement under Medicare and private payers, removing barriers to NP-led prescribing of controlled substances, addressing telehealth regulation consistency across state lines, and strengthening NP roles in behavioral health and primary care shortage areas. Workforce funding and loan-repayment programs also remain high priorities.
- How do I find out which legislators sit on health committees in my state?
- Visit your state legislature's official website and look for committee rosters under headings such as Health, Health and Human Services, or Public Health. You can also search your address on your legislature's "find my legislator" tool, then check each representative's committee assignments. Your state NP association often publishes updated lists of health committee members as well.
- Can NPs lobby or donate to political campaigns?
- Absolutely. As private citizens, nurse practitioners may donate to candidates, volunteer for campaigns, and lobby legislators on policy issues. Many NP professional organizations also operate political action committees (PACs) you can contribute to. If you lobby on behalf of an organization and exceed certain spending thresholds, federal or state registration requirements may apply, so check your state's lobbying disclosure rules.