Most important takeaways…
- Medicare still prohibits NPs from signing certificates of terminal illness for hospice.
- Nearly half of Medicare decedents in 2024 never received hospice services.
- Telehealth and NP-led palliative models are closing rural hospice gaps.
Diane Pagan, a nurse practitioner who provides home-based primary care for older adults, had a patient named Marie who was nearly 96, living with stage IV chronic kidney disease, a suspicious breast mass, and dementia. Marie's daughter wanted palliation and a peaceful death at home. Pagan completed a MOLST form, and a hospice agency accepted Marie. Then the process stalled: no physician would sign the Certificate of Terminal Illness required by Medicare.1 Marie's primary care physician had left the practice, and her nephrologist declined.
Pagan had the clinical authority to diagnose, treat, and manage Marie's end-of-life care, yet a federal rule written more than 40 years ago barred her from completing a single document. That tension, between what NPs are trained and licensed to do and what Medicare permits, sits at the center of hospice access failures across the country. It is especially acute in geriatric populations, where NPs increasingly serve as the sole primary provider. Understanding nurse practitioner differential diagnosis authority makes the restriction even harder to justify: an NP who can work through a complex diagnostic workup cannot sign one certification form.
Why Hospice Remains Underutilized Despite Proven Benefits
Just over half of all Medicare decedents, roughly 53 percent, used hospice in 2024, representing approximately 1.91 million enrollments.1 That figure reflects real progress over the past decade, yet it also means that nearly half of dying Medicare patients never access a benefit specifically designed to ease their final months.
The Numbers Behind the Gap
Who reaches hospice, and when, tells an important story. Cancer patients are consistently referred at higher rates than patients with other serious diagnoses. In 2024, circulatory conditions (including heart failure) accounted for about 29.8 percent of hospice stays, while neurological and neurovascular diagnoses made up roughly 25.4 percent. Cancer represented about 22.3 percent, respiratory diseases around 10.1 percent, and kidney disease a mere 3 percent.1 Read those numbers carefully: they reflect the composition of patients already enrolled, not overall referral rates. What the data signals, when paired with what we know about disease trajectories, is that patients with non-cancer diagnoses are still far less likely to be identified and referred in time, even though conditions like advanced dementia, end-stage heart failure, and COPD carry prognoses that are just as serious.
Timing compounds the problem. The median hospice length of stay in recent years has held at approximately 18 days.1 One in four patients who enroll in hospice has historically been discharged or died within a week,3 suggesting that referrals often happen only in the final crisis. Hospice was designed to provide weeks or months of coordinated comfort care, not a brief transition before death.
Three Drivers of Underutilization
Several interconnected factors explain why enrollment stays low and referrals come late.
- Prognostic uncertainty: Unlike cancer, conditions such as dementia, COPD, and heart failure follow unpredictable decline curves. Providers, including physicians and NPs alike, hesitate to certify a six-month prognosis when a patient might stabilize temporarily.
- Late referrals: By the time a terminal trajectory is undeniable, patients and families have little time to benefit from hospice's full scope of services, including chaplaincy, social work, caregiver support, and pain management planning. hospice nurse partnerships with families can help bridge this gap earlier in the process.
- Structural and policy barriers: Federal rules, reimbursement structures, and scope-of-practice restrictions create friction at the point of referral, a topic covered in depth in the next section.
Disparities That Demand Attention
Utilization is not equal across populations. Available data from 2023 shows that roughly 53 percent of white Medicare decedents used hospice, compared to about 38 percent of Black beneficiaries, 43 percent of Hispanic beneficiaries, and 38 percent of Asian and Pacific Islander beneficiaries.2 Rural areas face a compounding challenge: provider density in rural settings lags urban areas by an estimated 40 percent, limiting access even when patients and families want hospice care.2 Understanding how nurse practitioners improve rural healthcare access is one piece of the solution.
Why This Falls on NP Shoulders
Nurse practitioners are increasingly the day-to-day primary providers for older adults and patients with complex chronic illness, exactly the populations most affected by these gaps. In home-based care, long-term care facilities, and underserved communities, an NP is often the clinician who knows a patient best, tracks their decline, and has the relationships needed to begin a serious goals-of-care conversation. That makes hospice underutilization an NP issue, not just a systems issue. When access barriers prevent a qualified patient from enrolling, it is frequently the NP at the bedside who witnesses the cost.
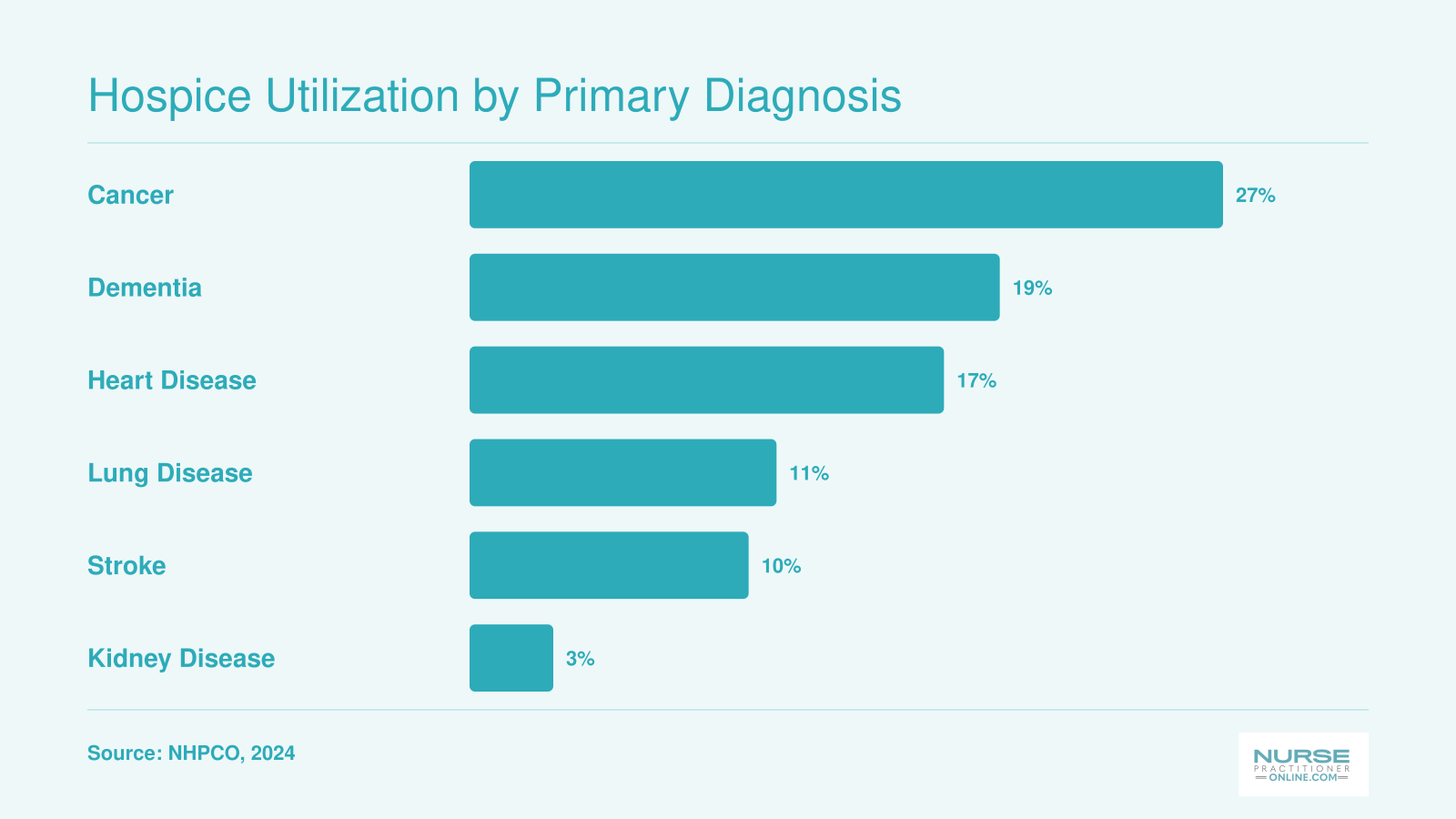
Hospice Utilization by Primary Diagnosis
Cancer patients have historically dominated hospice enrollment, but the majority of Americans who could benefit from end-of-life comfort care live with non-cancer conditions. For NPs managing multi-morbid geriatric panels, the gap between cancer and non-cancer referral rates reveals how much work remains in expanding timely hospice access.
The CTI Problem: How Medicare Law Blocks NP-Led Hospice Referrals
Can nurse practitioners legally certify a patient for hospice under Medicare?
No. Despite full authority to diagnose terminal illness, manage end-of-life care, and write orders for palliative interventions, nurse practitioners cannot sign the Certificate of Terminal Illness (CTI) required for Medicare hospice eligibility. That regulatory restriction, written into federal law more than four decades ago, names only physicians as eligible certifiers. The gap creates real, sometimes devastating delays for patients who need comfort care most.
In 2026, as reported by The Examiner News, hospice nurse practitioner Diane Pagan encountered this barrier firsthand.2 Her 96-year-old patient Marie, living with stage IV chronic kidney disease, a suspicious breast mass, and dementia, qualified clinically for hospice. Marie's daughter requested a peaceful death at home. A hospice agency accepted the patient. But Pagan could not complete the referral because Medicare requires a physician signature on the CTI. Marie's primary care physician had left the practice, and her nephrologist declined to sign. The patient remained in limbo, caught between clinical need and regulatory inflexibility.
Why the CTI Exists and Who Can Sign It
Medicare hospice benefits hinge on a certification that the patient has a life expectancy of six months or less if the disease runs its normal course. This certification, codified in 42 CFR 418.22, must be signed by two physicians for the initial hospice period, and by one physician for subsequent recertifications. Physician assistants, clinical nurse specialists, and nurse practitioners are excluded, even when they serve as the patient's primary or specialty provider and possess identical diagnostic and prognostic expertise.
The restriction is not rooted in scope-of-practice concerns or clinical competency. It is a relic of Medicare law written before advanced practice registered nurses (APRNs) gained independent practice authority in most states. Full practice authority states have moved well beyond this federal standard, yet the CTI statute has not kept pace with the evolution of the NP role or the realities of geriatric and rural care delivery, where NPs often function as the sole or primary clinician for vulnerable populations.
Current Legislative and Regulatory Efforts
Efforts to modernize the CTI statute have surfaced periodically in Congress and at the Centers for Medicare & Medicaid Services (CMS). To track federal legislation that would grant NPs authority to certify hospice eligibility, monitor Congress.gov for bills using keywords like "hospice certification," "nurse practitioner," and "Certificate of Terminal Illness." The Palliative Care and Hospice Education and Training Act (PACE Act) has included provisions related to NP scope in palliative care in past sessions, though specific CTI language varies by version. Watch the House Energy and Commerce Committee and the Senate Finance Committee for hearings, markup, or bill movement.
For regulatory action, visit the Federal Register at federalregister.gov and search for "nurse practitioner hospice certification" or "CTI certification authority." CMS may issue proposed or final rules that interpret or expand the physician certification requirement under existing statute. Check the CMS hospice center on CMS.gov for interim final rules and policy updates.
Professional advocacy groups offer another monitoring channel. The American Association of Nurse Practitioners (AANP) and the National Hospice and Palliative Care Organization (NHPCO) publish regulatory alerts, policy briefs, and advocacy toolkits when legislation or rulemaking advances. A solid nurse practitioner health policy toolkit can help you engage directly with bill sponsors and committee staff. Setting up email alerts from these organizations ensures timely notice of progress.
The Practical Cost of Inaction
Until federal law changes, NPs must rely on physician colleagues to sign CTIs, even when the NP managed the patient's care, diagnosed the terminal condition, and led the family conversation. In settings where physician access is limited, or where collaborative relationships are strained or nonexistent, patients face enrollment delays or outright denials. The policy mismatch undermines the NP's clinical role and, more importantly, denies patients timely access to hospice services designed to ease suffering and support families during the final chapter of life.
System-Level Barriers NPs Face in Hospice Care
State-based full practice authority states stands in sharp contrast to the federal Medicare rules that govern hospice care, a split that creates ongoing system-level barriers for nurse practitioners.
When State Authority Meets Federal Limits
Even in the 27 states that grant NPs full practice authority, federal Medicare regulations override state law at the hospice bedside. The Certificate of Terminal Illness (CTI), which triggers the hospice benefit, still requires a physician signature under rules written more than 40 years ago. NP scope-of-practice victories stop at a policy wall: an NP can diagnose, treat, and manage end-stage disease, yet cannot certify that same patient for hospice. This fracture forces a handoff to a physician at the very moment the patient needs a seamless transition to comfort care.
The attending physician billing rules add another layer. When an NP serves as the hospice attending of record, reimbursement defaults to 85% of the physician fee schedule, if the hospice agency even has a credentialing pathway for NP attendings. Many agencies do not, defaulting to physician-only models that sideline the NP who knows the patient best.
Reimbursement at a Discount
Financial disincentives ripple through every NP-led hospice interaction. Face-to-face encounters for hospice recertification, family conferences, and complex care coordination are often paid at that reduced rate, despite identical clinical intensity. The result is a system that economically rewards physician involvement even when the NP is the most appropriate and available clinician.
- Attending physician billing: When an NP serves as the patient's attending, hospice agencies may not be able to bill under the NP's NPI, forcing a physician proxy or delaying enrollment until a physician can assume the role.
- Care coordination gaps: Critical services like goals-of-care discussions and advance care planning are under-reimbursed, discouraging the extended visits that hospice enrollment requires.
A Workforce Crisis in Palliative and Hospice Care
The workforce data make the NP's role essential, not optional. According to a 2019 Health Affairs analysis, only 9,300 additional palliative care professionals were trained that year, while a Center to Advance Palliative Care survey identified just six APRN fellowship positions in the entire country, with three more in planning.1 Meanwhile, the U.S. Bureau of Labor Statistics projects a 35% job growth rate for APRNs through 2034, with an annual need for 32,700 new NPs.2 The gap between the demand for hospice-savvy clinicians and the training pipeline is enormous. Most NP programs provide minimal formal content in hospice and palliative medicine, leaving graduates to learn on the job, a pattern that NP program capacity shortages only deepen. NPs are positioned to close the workforce gap, but only if policy and education align.
The Handoff Problem: Why Coordination Fails
Hospice enrollment is a chain of handoffs: the NP assesses eligibility, a physician signs the CTI, the hospice agency accepts the patient, and the family consents. Each link is a failure point. The NP may identify a clearly eligible patient, yet waste days locating a willing physician, especially in rural areas or after-hours. In the worst cases, as illustrated by a home-based primary care NP who could not get a CTI signed for a 96-year-old with advanced kidney disease and dementia, the patient dies without ever receiving hospice.3 Fragmented NP-led patient care teams turn a clinical determination into a bureaucratic maze, with patients and families caught in the middle.
Related Articles
Patient and Family Barriers: Fear, Misconceptions, and Cultural Concerns
Even when an NP has done everything clinically correct, the path to hospice enrollment can stall at the patient and family level. Fear, misinformation, and deeply held cultural beliefs are among the most common reasons eligible patients never make it into the comfort-focused care they deserve.
The word "hospice" itself carries a heavy emotional weight for many families. A persistent misconception is that choosing hospice means giving up, or even hastening death. In reality, hospice is a philosophy of care centered on quality of life, pain management, and dignity during a natural process. NPs are well positioned to reframe this conversation, but doing so requires skill, patience, and an understanding of how families process grief and fear in real time. Brushing up on strategies for dealing with difficult family members in healthcare can give NPs a practical framework for these emotionally charged discussions.
Cultural and religious beliefs add another layer of complexity. Some communities associate hospice with abandonment by the medical system, while others hold strong convictions about fighting illness until the very end, regardless of prognosis. Language barriers can compound these challenges, particularly when nuanced concepts like "terminal illness" or "palliative intent" lose meaning in translation. NPs practicing in diverse communities need culturally humble communication strategies and, when possible, access to trained medical interpreters.
Family dynamics also play a role. Adult children may disagree with each other, or with the patient's own wishes, about the right course of action. A patient who clearly wants comfort care at home may be overruled by a well-meaning family member who insists on continued curative treatment. In these situations, the NP's role shifts toward facilitation and advocacy, helping families hear and honor the patient's voice.
Finally, prior negative experiences with the healthcare system, whether rooted in systemic distrust, past medical trauma, or simply a lack of familiarity with hospice services, can make families reluctant to engage. The evolving role of nurse practitioners increasingly includes community education and trust-building, and these skills are just as vital at the bedside as any clinical competency. Understanding what hospice actually offers, and communicating it clearly and compassionately, is one of the most powerful tools an NP can bring to these conversations.
Diagnosis-Specific Hospice Barriers: Cancer, Dementia, Heart Failure, and COPD
Not every terminal diagnosis presents the same challenges when it comes to hospice referral. Each condition carries its own eligibility criteria, prognostication difficulties, and systemic obstacles that can delay or prevent patients from receiving comfort care. The table below breaks down these barriers by diagnosis and offers a practical action step NPs can take to move patients toward timely hospice enrollment.
| Diagnosis | Key Eligibility Criteria | Primary Referral Barrier | NP Action Step |
|---|---|---|---|
| Cancer | Documented metastatic or recurrent disease with declining functional status; patient has elected comfort over curative treatment | Late referral remains common because oncologists may resist stopping active treatment, even when prognosis is poor. Patients and families often equate ending treatment with giving up. | Initiate parallel planning early by introducing palliative care alongside active treatment, and revisit goals of care at each disease progression point rather than waiting for oncology to signal that options are exhausted. |
| Dementia | FAST (Functional Assessment Staging) scale at Stage 7 or beyond, with at least one comorbid condition such as aspiration pneumonia, sepsis, or recurrent infections in the prior year | Estimating a six month prognosis in dementia is notoriously difficult. Many NPs have not been trained to use the FAST scale, and cognitive decline does not follow a predictable linear trajectory. | Seek training in FAST scale staging and begin documenting functional decline longitudinally. Use serial assessments over months to build a clear clinical picture that supports a hospice eligibility determination. |
| Heart Failure (CHF) | NYHA Class IV symptoms at rest despite optimal medical therapy; recurrent hospitalizations; ejection fraction of 20% or less (when available) | Unpredictable exacerbation and remission cycles make prognostication unreliable. Patients may appear stable between acute episodes, leading clinicians to delay referral repeatedly. | Use palliative care as a bridge to hospice. Enroll patients in concurrent palliative services during the disease trajectory, and establish clear clinical benchmarks (such as frequency of hospitalizations) that trigger a hospice conversation. |
| COPD | FEV1 less than 30% predicted after bronchodilator use; cor pulmonale or right heart failure; resting hypoxemia on supplemental oxygen; recurrent emergency visits or hospitalizations | Similar to heart failure, COPD follows an unpredictable course of exacerbations and recoveries. Clinicians and patients often view each crisis as reversible, which delays recognition of the terminal phase. | Track hospitalization frequency and functional decline over time. When a patient requires two or more hospitalizations in 12 months with worsening baseline function, initiate a structured goals of care discussion and consider hospice referral. |
| End Stage Renal Disease (ESRD) | Patient elects to discontinue or not initiate dialysis; declining renal function with uremic symptoms; significant comorbidities that limit life expectancy | Once a patient chooses to stop dialysis, decline is rapid, often occurring within days to two weeks. The referral window is extremely narrow, and delays in obtaining a physician signature on the Certificate of Terminal Illness can consume the limited time available. | Prepare for the possibility of dialysis discontinuation well in advance. Have hospice agency contacts, advance directives, and goals of care conversations completed before the patient makes a final decision, so that enrollment can proceed immediately. |
Overcoming Rural and Access Barriers Through Telehealth
Rural communities face persistent shortages of hospice and palliative care services, leaving many patients without timely access to end-of-life support. For nurse practitioners serving these areas, telehealth expansion for nurse practitioners is emerging as a practical way to bridge care gaps while keeping families connected to local resources.
How Telehealth Expands Hospice Access
Telehealth brings interdisciplinary hospice care directly to patients in remote or underserved locations. Virtual visits allow NPs to conduct symptom assessments, coordinate with local nursing staff, and provide family education without the travel burden that often delays care. The model works well for routine check-ins and medication titrations, particularly with patients who have chronic, predictable illness trajectories like advanced heart failure or dementia.
For patients in frontier counties or on tribal lands, a telepresenter, such as a home health aide, can assist with technology and vital signs, letting the NP focus on clinical decision-making. Hospice agencies that combine telehealth with periodic in-person visits often see stronger care continuity and family satisfaction, though evidence is largely qualitative so far.
Practical Considerations for NP-Led Telehealth Hospice Visits
Implementing telehealth in hospice requires attention to several details:
- Technology setup: Simple platforms with video, screen sharing, and secure messaging reduce barriers for elderly patients. Pre-session test calls can prevent frustration.
- Team communication: Clear workflows between the NP, bedside nurses, social workers, and chaplains ensure that virtual encounters capture the full picture of a patient's needs.
- Family engagement: Teaching caregivers to use the platform and prepare questions ahead of time makes visits more efficient and reduces anxiety.
NPs also play a unique role in recognizing when a virtual visit is insufficient. Complex symptoms or sudden declines still require hands-on evaluation, so telehealth protocols must include clear triggers for in-person escalation.
Policy and Reimbursement Landscape
Medicare rules shape how NPs can use telehealth in hospice. During the COVID-19 public health emergency, CMS temporarily allowed hospice providers to perform routine home care recertification visits via telehealth. Subsequent legislation extended some flexibilities, though permanent regulatory changes are still under discussion. Nurse practitioners should review primary care billing and coding guidance and seek direction from organizations like the National Hospice and Palliative Care Organization for current billing and scope-of-practice rules in their state.
Although telehealth cannot replace every in-person touchpoint, it addresses a core barrier: geography. For NPs who serve as the primary care nurse practitioner for rural patients with serious illness, embracing virtual care models expands the reach of hospice services at a time when more Americans want to die at home.
NP-Led Hospice and Palliative Care Models That Work
Despite the regulatory barriers that prevent nurse practitioners from signing certificates of terminal illness, NP-led palliative and hospice care models are demonstrating measurable success across multiple settings. These programs show what becomes possible when NPs can practice to the full extent of their clinical training, offering blueprints for expanding access to quality end-of-life care.
Home-Based Palliative Care With NP Leadership
One well-documented model involves NP-led home palliative care teams supported by physician collaboration for specific regulatory requirements. In a rural home palliative care service using this structure, outcomes have been striking: 100 percent compliance with advance care planning, a 21 percent hospice admission rate, and cost savings of approximately 49,000 Australian dollars per patient.1 Patients also experienced statistically significant reductions in symptom distress (p = 0.003).1 This model succeeds because NPs maintain ongoing relationships with patients and families, conducting whole-person assessments during home visits and integrating goals-of-care discussions into routine care rather than reserving them for crisis moments.
Diane Pagan's Senior Moments Care offers another example of this approach in action. As reported in The Examiner News, Pagan provides home-based primary care for older adults and is preparing to open the Geriatric Center of Excellence in Somers in September 2026.5 Her practice demonstrates how NP-led care naturally incorporates palliative principles, completing advance directives like MOLST forms and coordinating with families around patient wishes.
Hospital and Nursing Home Models
NP-led palliative care is also proving effective in institutional settings. An embedded NP-led hospital palliative care model at a New York City academic medical center, pairing nurse practitioners with social workers for primary palliative care delivery, has improved access and reduced hospital utilization.2 Meanwhile, research analyzing over 334,000 nursing home residents with dementia has examined how nurse practitioner role in healthcare shapes end-of-life outcomes in long-term care.3
Telephonic nurse-led palliative care has shown comparable symptom management results to specialty outpatient care in multisite cancer trials, expanding reach for patients who cannot easily travel.4
The Research Gap
A 2026 systematic review identified 20 studies examining nurse-led palliative care interventions, confirming growing interest in this area.6 Yet NP-led palliative models remain under-documented and under-funded relative to their demonstrated value. The continuity of relationship, integration of advance care planning into routine visits, and whole-person assessment skills that make these models effective deserve more rigorous study and broader implementation.
Communication Frameworks for Difficult Hospice Conversations
Some of the most consequential conversations a nurse practitioner will ever have happen at the bedside of a seriously ill older adult. When a patient like Marie, nearly 96 with advanced kidney disease and dementia, needs comfort-focused care, the NP must guide families through grief, fear, and uncertainty, all while navigating the clinical realities of hospice eligibility.
Structured communication frameworks help NPs approach these moments with both compassion and clarity. The SPIKES protocol (Setting, Perception, Invitation, Knowledge, Emotions, Summary) is widely used in palliative care settings to deliver serious news. Similarly, the NURSE mnemonic (Naming, Understanding, Respecting, Supporting, Exploring) helps NPs respond to emotional cues without shutting them down. Both frameworks give clinicians a reliable scaffold when conversations feel overwhelming.
For nurse practitioner career advancement in end-of-life care, knowing how to use these frameworks is as important as any clinical skill. A family meeting to discuss hospice enrollment should address four core elements: the patient's current prognosis, the goals of care, what hospice services will and will not cover, and who will be coordinating ongoing care. Walking families through each element reduces confusion and builds the trust needed to move forward.
One underappreciated barrier is the assumption that families already understand what hospice means. Many equate it with giving up, when in fact it redirects treatment toward comfort rather than cure. NPs can reframe hospice as an active, patient-centered choice, one that honors the person's values rather than abandoning them. Completing documents like a MOLST form together with the family reinforces that the care plan reflects the patient's own wishes.
When managing decision fatigue as a nurse practitioner, having a repeatable conversation structure matters even more. High-stakes end-of-life discussions can drain emotional and cognitive reserves quickly. Preparing talking points in advance, anticipating common objections, and debriefing with colleagues afterward are all practical habits that protect both the NP and the quality of care delivered.
Clear, empathetic communication does not eliminate every barrier to hospice enrollment, but it removes one of the most common ones: the family's fear of the unknown. When NPs lead these conversations with confidence and structure, patients are far more likely to reach the comfort care they deserve.
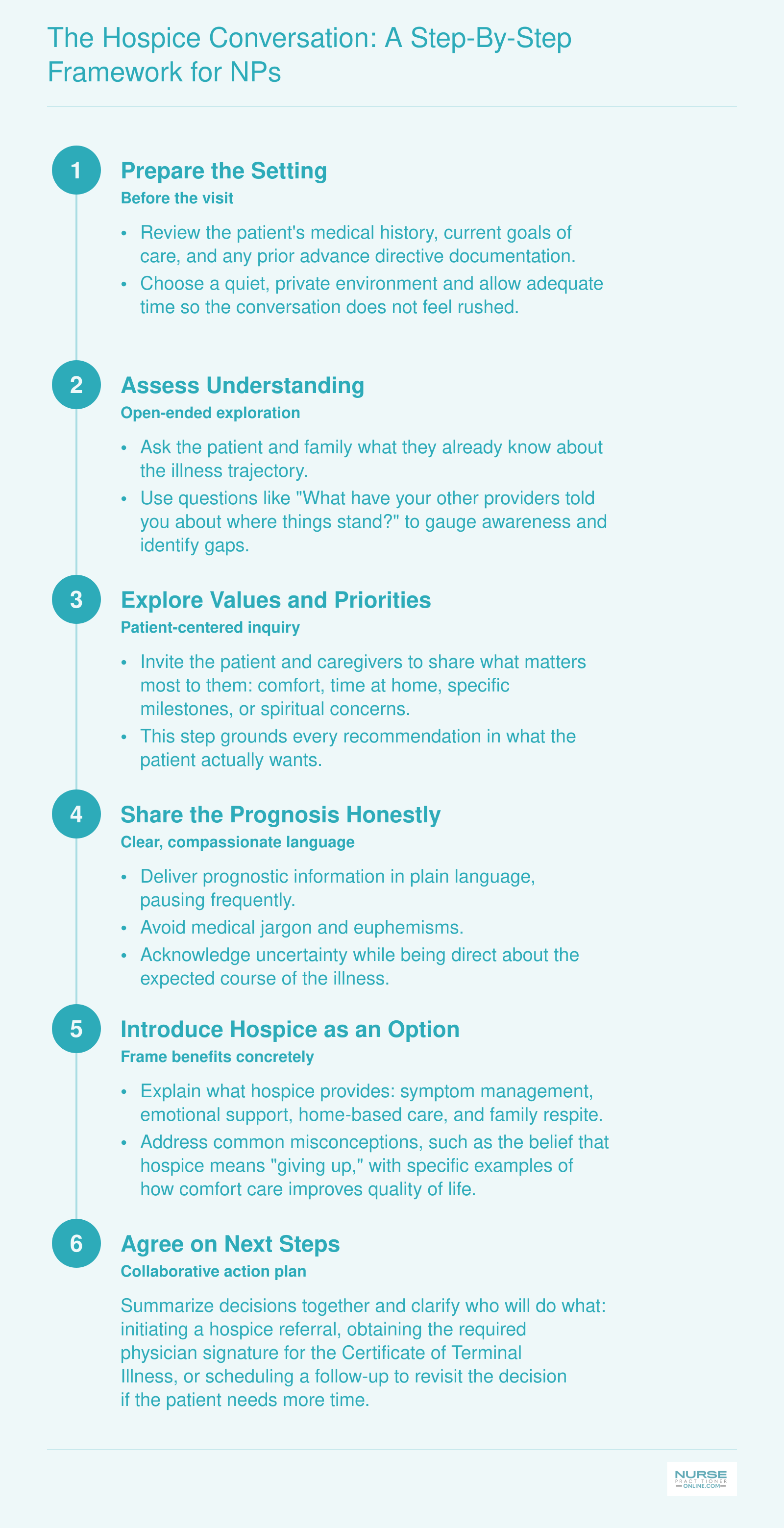
The Hospice Conversation: A Step-By-Step Framework for NPs
Effective hospice conversations follow a structured sequence that respects patient autonomy while ensuring clarity about prognosis and goals. This framework, synthesized from the SPIKES protocol and adapted for NP-led end-of-life discussions, offers a practical clinical guide. It is not a replacement for formal communication training but a starting point for building confidence in these critical conversations.
Advocacy and Policy Action: What NPs Can Do Now
Advocacy means taking concrete steps to change the policies and systems that limit NPs' ability to get patients into hospice care. For adult-gerontology nurse practitioners on the front lines, inaction is not an option when a simple signature can be the difference between comfort and crisis.
Push for Federal CTI Reform
The Certificate of Terminal Illness (CTI) barrier is rooted in Medicare law that hasn't seen a meaningful update in over four decades. NPs can drive change by contacting their representatives about legislation that would modernize this requirement. Even without a named bill in this article, your voice matters: ask your lawmakers to cosponsor measures that allow NPs to certify terminal illness for hospice eligibility. Engage with the American Association of Nurse Practitioners (AANP) and the Hospice and Palliative Nurses Association (HPNA) to amplify advocacy through organized letters, calls, and social media campaigns. When CMS opens public comment periods on hospice payment rules, file a statement detailing how the CTI restriction harms your patients.
Strengthen Practice-Level Systems
While federal reform moves slowly, build a bridge now. Identify and cultivate relationships with physicians in your community who are willing to sign CTI forms when you cannot. A proactive network prevents referral stalls like the one Diane Pagan experienced. Push your health system to credential NPs for hospice agency collaboration so your assessments carry full weight. Most importantly, document every case where a CTI barrier delayed or denied hospice: patient identifiers removed, but clinical details intact. These real-world examples are powerful evidence when talking to legislators or administrators. Newer colleagues entering practice benefit from this groundwork too, and sharing what you've learned mirrors the kind of guidance covered in new nurse practitioner tips that help early-career NPs navigate systemic challenges.
Invest in Education and Mentorship
Clinical excellence fuels advocacy. Pursue hospice and palliative care certification through the Advanced Certified Hospice and Palliative Nurse (ACHPN) or equivalent pathways, and keep credentials current through nurse practitioner continuing education that includes palliative care content. Integrate palliative care conversations into your preceptor teaching: show students how to present hospice benefits clearly and compassionately. Mentor newer NPs to confidently manage end-of-life discussions so they enter practice ready to challenge outdated policies.
Build the Infrastructure: Lead by Example
Diane Pagan, the geriatric NP featured in The Examiner News, is opening the Geriatric Center of Excellence in Somers in September 2026. That facility will deliver home-based primary care and palliative services without systemic roadblocks. It is a model for what NPs can create when existing structures fail, and it reflects the broader nurse practitioner advancement opportunities that emerge when clinicians refuse to wait for permission. Whether you launch a similar center, a telehospice program, or a community coalition, the message is the same: NPs do not have to wait for permission to build the systems their patients need.
Common Questions About NPs and Hospice Care
These are some of the most common questions nurse practitioners ask about hospice referrals, barriers, and their role in end-of-life care. Each answer points to a section of this guide where you can explore the topic in greater depth.
- Can a nurse practitioner sign a hospice order?
- Under current Medicare guidelines, nurse practitioners cannot sign a Certificate of Terminal Illness (CTI), which is required for hospice enrollment. Only physicians are authorized to certify terminal illness, a restriction rooted in federal law written more than 40 years ago.1 NPs can order palliative treatments and coordinate care, but the CTI requirement remains a significant policy barrier. See the section on the CTI problem for a detailed breakdown.
- What are the biggest barriers to hospice care?
- The largest hospice care barriers include the CTI restriction that blocks NP-led referrals, fragmented care coordination among multiple specialists, patient and family misconceptions about hospice meaning "giving up," and cultural concerns about end-of-life discussions. System-level issues such as insurance complexity and late referral patterns also play major roles. The sections on system-level barriers and patient and family barriers cover these challenges in detail.
- Why is hospice care underutilized?
- Hospice remains underutilized because many patients are referred too late or not at all. Prognostic uncertainty in non-cancer diagnoses like dementia, heart failure, and COPD makes eligibility harder to determine. Provider hesitation, family resistance, and outdated Medicare policies that exclude NPs from certification all contribute. Our section on why hospice remains underutilized explores the data behind these trends.
- What are barriers to hospice care in rural areas?
- Rural communities face workforce shortages, limited hospice agency coverage, long travel distances for in-home visits, and fewer specialists available to sign the required CTI. Telehealth has emerged as a practical solution, allowing NPs to conduct goals-of-care conversations, coordinate with distant hospice teams, and monitor symptoms remotely. The section on overcoming rural and access barriers through telehealth outlines actionable strategies.
- How can nurse practitioners improve end-of-life care?
- NPs can improve end-of-life outcomes by initiating early palliative care conversations, using structured communication frameworks for difficult discussions, and advocating for policy changes that expand NP authority over hospice certification. Building relationships with local hospice agencies and staying current on best states for nurse practitioners with full practice authority can also inform where policy momentum is strongest. See the sections on communication frameworks and advocacy for specific tools.
- What is the role of a nurse practitioner in hospice care?
- NPs serve as primary care providers, care coordinators, and patient advocates in hospice settings. They assess symptom burden, manage complex medication regimens, facilitate family meetings, and guide patients through advance care planning. In many geriatric and home-based practices, NPs are the clinician who knows the patient best, yet federal law still limits their authority to formally certify hospice eligibility. Our section on NP-led hospice models highlights programs where NPs drive better outcomes.