Most important takeaways…
- PMHNPs diagnose, prescribe, and deliver psychotherapy across the lifespan, distinguishing them from general NPs and psychiatrists.
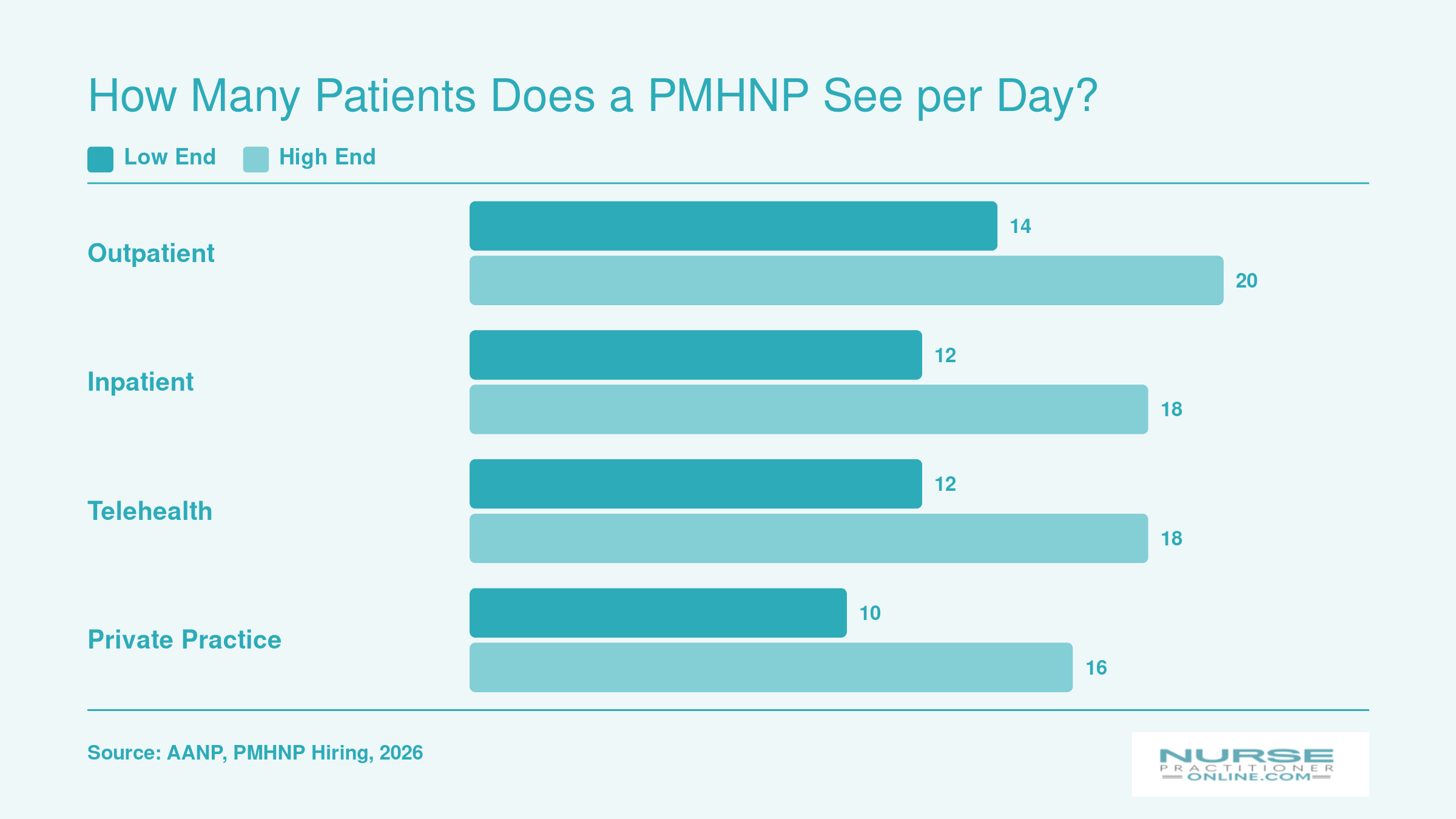
- Daily patient volumes typically range from 8 to 20 depending on appointment type and practice setting.
- Gonzaga graduate Shahrum Ali estimates his PMHNP degree delivered roughly 30 percent higher return on investment.
- Sustainable careers require employer-level supports like manageable caseloads, protected charting time, and clinical supervision.
The psychiatric workforce shortage has moved from a slow-building concern to an acute crisis, with more than 160 million Americans living in federally designated mental health professional shortage areas as of 2025. Psychiatric-mental health nurse practitioners sit at the center of the response: they are the fastest-growing segment of psychiatric prescribers in the country, trained to bridge holistic nursing assessment with psychiatric diagnosis, medication management, and psychotherapy.
What does a typical day actually look like for these providers? The answer shifts depending on setting, patient volume, and career stage. Insights from Shahrum Ali, a recent PMHNP graduate who completed his degree online while working full time, help ground the picture in lived experience rather than theory. The practical tension for most nurses weighing this path is straightforward: demand is high and compensation is strong, but caseload pressures and emotional toll are real variables that differ sharply from one employer to the next.
What Does a PMHNP Do? Role, Scope, and How It Differs From a Psychiatrist
Psychiatric-mental health nurse practitioners function as full-scope psychiatric providers who diagnose mental health conditions, prescribe medications, deliver psychotherapy, and coordinate care across the lifespan. Unlike family nurse practitioners who consult on behavioral health as needed, PMHNPs specialize exclusively in psychiatric assessment and treatment, managing everything from first-line antidepressants to complex polypharmacy for treatment-resistant psychosis.
Education Path and Practice Authority
The path to PMHNP practice begins with a BSN, followed by a two- to three-year MSN-PMHNP program that blends advanced pharmacology, psychopathology, and evidence-based psychotherapy modalities with 500 to 750 supervised clinical hours. Graduates sit for the national certification exam administered by the American Nurses Credentialing Center (ANCC), earning the credential Psychiatric-Mental Health Nurse Practitioner, Board Certified (PMHNP-BC). This differs sharply from the psychiatrist route: four years of medical school, four years of psychiatric residency, and optional fellowship training, resulting in an MD or DO degree rather than a nursing credential.
Prescriptive authority varies by state. In 26 states and the District of Columbia as of 2026, PMHNPs practice independently without physician collaboration or supervision, writing prescriptions for controlled substances and managing their own patient panels. In the remaining states, collaborative agreements with physicians are required, though the day-to-day clinical work often looks identical. This independence makes PMHNPs particularly valuable in rural and underserved communities where psychiatrist shortages leave patients waiting months for care, a dynamic explored in depth in discussions about the NP role in modern healthcare.
Patient Populations and Clinical Breadth
PMHNPs treat the full spectrum of psychiatric conditions. Typical patient presentations include:
- Mood and anxiety disorders: Major depression, generalized anxiety disorder, panic disorder, and treatment-resistant variants
- Trauma and stress-related disorders: PTSD, acute stress disorder, and complex trauma presentations
- Attention and impulse-control disorders: ADHD across the lifespan, including initial diagnosis in adults
- Substance use disorders: Medication-assisted treatment for opioid, alcohol, and stimulant use, often integrated with behavioral counseling
- Severe mental illness: Bipolar disorder, schizophrenia, schizoaffective disorder, requiring close monitoring and antipsychotic management
This breadth positions PMHNPs as first-line providers for the majority of mental health presentations, reserving psychiatrist referrals for cases requiring electroconvulsive therapy, transcranial magnetic stimulation, or forensic expertise.
Hour-By-Hour: Sample PMHNP Schedules by Setting
Outpatient clinic days begin with a structured eight-hour shift and scheduled intakes, while inpatient psychiatric units require earlier starts, bedside rounding, and interdisciplinary team meetings that reshape the entire day.1 The setting determines not just where you work but how you allocate every hour of clinical time, charting, and collaborative care planning.
Outpatient Clinic: A Blend of Intakes and Follow-Ups
Most outpatient PMHNPs arrive between 8:00 and 8:30 a.m., review the day's schedule, and prepare for two to four new intakes interspersed with 14 to 20 total patient appointments. A typical morning block runs from 8:30 to 11:30, mixing 45- to 60-minute intakes with 15- to 30-minute medication management follow-ups. From 11:30 to 12:00, many clinicians catch up on charting before a working lunch at 12:00 to 12:30.
Afternoons shift to follow-up appointments and complex cases from 12:30 to 3:30, followed by a dedicated charting window from 4:15 to 5:00. Some practices hold weekly or monthly team meetings midday or early morning, each lasting about an hour. The nine-hour shift balances direct patient care with administrative tasks, and clinicians who protect their charting blocks report lower end-of-day documentation stress.
Inpatient Psychiatric Unit: Early Starts and Daily Team Rounds
Inpatient PMHNPs typically begin between 6:45 and 7:00 a.m., spending the first hour reviewing overnight notes and safety flags. Bedside rounds start at 8:00 and run until 10:30, covering 12 to 18 patients with short 5- to 15-minute follow-ups and one or two 45- to 60-minute intakes for new admissions.
From 10:30 to 11:30, the interdisciplinary team meets to discuss treatment plans, discharge readiness, and social work coordination. After an abbreviated lunch from 12:30 to 1:00, afternoons are reserved for family meetings, emergency department consults, and re-evaluations until 2:30. A 60- to 90-minute charting block from 2:30 to 3:30 closes out the eight- to ten-hour shift, which often ends by 3:30 to 4:00 p.m.
Telehealth: Virtual Huddles and Appointment Stacking
Telehealth PMHNPs log in at 8:30, join a brief virtual huddle from 8:45 to 9:00, then begin patient blocks at 9:00. Morning intakes run 30 to 60 minutes each, with three scheduled before lunch at 12:00 to 12:30. Afternoon follow-ups from 12:30 to 4:30 are often stacked in 15- to 20-minute increments, allowing 12 to 18 total visits per day.
Charting breaks fall between 2:30 and 3:00, then again from 4:30 to 5:00 or 5:30. Monthly quality assurance and training calls replace the daily in-person team meeting. The flexibility of telehealth attracts PMHNPs who value remote work, though the risk of back-to-back video fatigue requires intentional boundary setting around screen time and break discipline. If you are preparing to interview for a telehealth role, reviewing virtual nurse practitioner interview tips can help you communicate that discipline to prospective employers. For a comparison of how other NP specialties structure their clinical days, our day in the life of a pediatric nurse practitioner profile offers a useful contrast.
Questions to Ask Yourself
How Many Patients Does a PMHNP See per Day?
Patient volume is one of the biggest factors shaping a PMHNP's daily rhythm. New patient intakes typically run 45 to 60 minutes, while follow-ups average 15 to 30 minutes, so the mix of appointment types directly determines how many people you see. Documentation also claims a significant chunk of your day: roughly 25% to 35% of total work hours, depending on setting. Keep in mind that productivity-based compensation models can push these numbers higher, which may boost earnings but can also cut into the time available for thorough, patient-centered care.
Inpatient Vs. Outpatient Vs. Telehealth: How the Day Differs
Does the setting where a PMHNP works actually change what a typical day looks like? The short answer is yes, significantly. The pace, patient acuity, team structure, documentation demands, and degree of autonomy can shift dramatically depending on whether you are working in a hospital unit, a community clinic, or a virtual practice.
Inpatient Psychiatric Settings
In an inpatient environment, the rhythm tends to be fast and highly collaborative. You are likely working alongside attending psychiatrists, social workers, case managers, and nursing staff. Patient acuity is higher, crises are more frequent, and your documentation burden reflects that intensity. On-call responsibilities are more common here than in other settings, and the expectation to respond quickly to acute changes is woven into the workday.
If you want a detailed picture of clinical rotation structures in inpatient psychiatry, PMHNP program directors at accredited schools are a useful first call. Many publish curriculum overviews that break down what students actually encounter across rotation sites, and those descriptions often reflect real-world workflows closely. For a broader look at how NP clinical rotations are structured, those resources can provide helpful context before you begin.
Outpatient and Community Clinics
Outpatient practice generally offers more predictability. Scheduled appointments, longer therapeutic relationships with patients, and more autonomous decision-making are common features. Documentation is still significant, but the pace allows for more deliberate charting. Team structures vary: some clinics integrate behavioral health fully, while others are primarily solo or small-group NP practices.
For firsthand accounts of what outpatient days actually look like, peer forums such as the AANP Community or PMHNP-focused groups on social platforms are worth exploring. Practicing PMHNPs there often discuss the practical differences in team dynamics, caseload management, and documentation tools across settings.
Telehealth and Virtual Psychiatry
Telehealth has become a meaningful practice option for psychiatric NPs, and the technology landscape continues to evolve. Platforms designed for healthcare video visits are commonly referenced in state telehealth guides, and the Center for Connected Health Policy (CCHP.org) maintains state-by-state information worth bookmarking. For a deeper look at platform comparisons and adoption trends, searching PubMed using terms like "telepsychiatry platform" surfaces peer-reviewed literature that goes beyond marketing materials.
For employment data across all three settings, the Bureau of Labor Statistics (BLS.gov) remains the most reliable starting point. The American Association of Nurse Practitioners (AANP) publishes practice surveys that capture telehealth adoption trends among NPs, and ANCC sets the certification standards that govern scope regardless of setting. If you are still weighing which clinical path best fits your skills and interests, securing the right clinical preceptor early can shape your experience in any of these environments. Using these sources together gives you a grounded picture before you commit to a path.
Related Articles
A PMHNP's Journey: From Online Program to Clinical Confidence
Reading a program brochure versus hearing from someone who actually finished one are two very different ways to evaluate a PMHNP path. Brochures sell the curriculum. Graduates tell you what the program asked of them and what it gave back. Shahrum Ali, who completed Gonzaga University's online MSN-PMHNP program, sat down for a Q&A published in June 2026 that offers a candid look at both sides of that equation.
Confidence as the Real Deliverable
Asked what skill grew most during the program, Ali didn't point to a clinical technique or a diagnostic framework. He pointed to confidence. He described a steady progression from tentative first-quarter clinicals to a final quarter where faculty no longer felt like supervisors evaluating him, but like peers consulting with him. That shift, from student to colleague, is the quiet outcome a lot of graduate programs promise and fewer actually deliver. For working nurses considering any advanced practice track, including adult-gerontology, it's worth asking current students whether they feel that arc happening in their own program.
The ROI Conversation, in Plain Numbers
Ali estimates his earning potential is roughly 30% higher with the PMHNP credential than it would be without an advanced degree.1 That figure is his personal estimate, not a national benchmark, but it's a useful anchor when you're weighing tuition, lost overtime, and three or more years of part-time study against long-term compensation. If you're exploring the differences between degree levels, our comparison of MSN vs DNP vs PhD in nursing can help you map out long-term value. If you're already a working RN, run the math on your own setting and region before committing.
Clinicals, Placements, and Working Full Time
The honest part of Ali's story: securing nurse practitioner clinical rotations on schedule was hard. He credits proactive communication with program facilitators, his own due diligence, and trading strategies with classmates who had already landed sites. He also worked full time throughout the program, leaning on the online coursework's flexibility and the extended clinical timeline to make it sustainable.
For adult-gerontology NP candidates reading this, the takeaways translate directly: budget time for placement hunting early, build a peer network you can text when a preceptor falls through, and choose a program structure that bends around your shift schedule rather than fighting it.
The biggest skill I developed was confidence, from first quarter clinicals to last quarter. By the end, faculty felt like peers.
PMHNP Salary and Compensation Structures
The table below draws on 2024 Bureau of Labor Statistics wage data for Nurse Practitioners broadly (BLS does not break out PMHNP-specific figures). Because psychiatric specialty NPs often command a premium over general NP roles, these numbers serve as a useful floor rather than a ceiling. Surrounding factors like your compensation model, productivity expectations, and practice setting can shift your actual take-home pay significantly in either direction.
| Wage Measure | Annual Salary |
|---|---|
| National Median (All NPs) | $129,210 |
| 25th Percentile | $109,940 |
| 75th Percentile | $149,570 |
| National Mean | $132,000 |
Burnout, Emotional Toll, and Self-Care Strategies for PMHNPs
Working in psychiatric care versus working in general nursing presents a stark difference in emotional demands. While all nurses face occupational stress, psychiatric mental health nurse practitioners navigate a unique landscape of secondary trauma, complex patient presentations, and systemic barriers that can accelerate burnout without proper safeguards in place.
The Scope of Burnout in Psychiatric Nursing
Burnout among psychiatric nurses has reached concerning levels. According to a DNP project from the University of Texas at Arlington, the burnout rate among psychiatric nurses stands at 91.1 percent1, dramatically higher than the 53 percent rate reported across the broader nursing workforce in 2026 data from the JAMA Network.2 Behavioral health providers overall show an 83 percent burnout rate per Trilliant Health's examination of America's behavioral health crisis.3
These numbers reflect the cumulative weight of caring for patients in crisis, managing complex medication regimens, and witnessing trauma on a daily basis. The demand-to-supply ratio for psychiatric nurse practitioners currently sits at 4:1 according to a 2026 workforce analysis4, meaning those in practice carry heavier caseloads than the field can sustainably support. For a broader look at where the shortages are most acute, see our breakdown of the psychiatric nurse practitioner shortage by state.
What Drives PMHNP Burnout
Several factors converge to create the conditions for burnout in psychiatric practice:
- Emotional labor and trauma exposure: Daily encounters with patients experiencing suicidal ideation, psychosis, or severe depression require sustained emotional regulation that depletes internal resources over time. The 2026 Nurse Salary and Work-Life Report found that 46 percent of nurses experience compassion fatigue.2
- Documentation burden: Forty-three percent of nurses cite documentation demands as a primary contributor to burnout.2 For PMHNPs, thorough psychiatric evaluations, treatment plans, and coordination notes compound this pressure.
- Workload and patient ratios: Nearly half of nurses (48 percent) identify staffing ratios as a burnout driver.2 In psychiatric settings with provider shortages, PMHNPs often see more patients than recommended.
- Moral distress: The 2026 report reveals that 51 percent of nurses experience moral injury, often from watching patients struggle to access care due to insurance barriers, bed shortages, or long wait times.2
Is Being a PMHNP Stressful?
Yes, this career carries significant stress, but that stress is manageable with intentional strategies. Sixty-two percent of nurses report feeling overwhelmed, and 53 percent experience prolonged stress.2 However, PMHNPs who build robust self-care practices and select settings aligned with their capacity report greater career satisfaction and longevity.
Burnout risk also varies considerably by practice environment. Inpatient psychiatric units and crisis stabilization roles expose providers to acute, high-intensity situations daily. Outpatient clinics and telehealth positions typically offer more predictable schedules and greater control over patient volume, reducing some stress triggers. You can explore the differences across settings in our guide to PMHNP subspecialty comparison.
Evidence-Based Strategies for Self-Care
Research supports several approaches for managing the emotional demands of psychiatric practice:
- Clinical supervision: Regular sessions with an experienced mentor provide space to process difficult cases and receive guidance on complex presentations.
- Peer consultation groups: Connecting with fellow PMHNPs, whether in person or virtually, reduces the isolation that 25 percent of nurses report feeling.2 Sharing experiences normalizes challenges and generates practical solutions.
- Mindfulness-based stress reduction: Structured mindfulness practices have demonstrated effectiveness in reducing provider burnout across mental health disciplines.
- Boundary-setting on caseload: Negotiating sustainable patient volumes during hiring discussions or advocating for limits within current positions protects against chronic overextension.
- Institutional supports: Employers offering schedule flexibility, employee assistance programs, and adequate administrative support create environments where PMHNPs can sustain their careers long-term.
The intensity of psychiatric practice does not have to lead to burnout. PMHNPs who proactively invest in their own wellbeing, and who choose employers that prioritize sustainable workloads, find that this deeply meaningful work remains fulfilling across decades of practice. Our full guide to preventing nurse practitioner burnout offers additional strategies you can put into action today.
Career Growth: From New Grad PMHNP to Leadership and Beyond
Your PMHNP career arc can stretch well beyond the exam room. After earning board certification and gaining a few years of clinical experience, many psychiatric NPs move into subspecialty niches such as addiction psychiatry, child and adolescent mental health, or forensic evaluation. Others pursue a DNP or post-master's certificate to qualify for leadership roles, faculty positions, or independent practice authority (available in a growing number of states). The entrepreneurship track is equally viable: opening a solo telehealth practice, building a group practice, or consulting for health systems on behavioral health integration. With the Bureau of Labor Statistics projecting roughly 135,000 new NP positions nationally through 2033, and persistent mental health workforce shortages across nearly two-thirds of rural Health Professional Shortage Areas, long-term demand for PMHNPs remains exceptionally strong.
Frequently Asked Questions About the PMHNP Career
These are some of the most common questions working nurses ask when considering a career as a psychiatric mental health nurse practitioner. Each answer draws on the real-world details explored throughout this guide.
- What does a psychiatric nurse practitioner do on a daily basis?
- A PMHNP conducts psychiatric evaluations, diagnoses mental health conditions, prescribes and manages medications, and provides therapy or brief interventions. A typical day includes reviewing patient histories, performing follow-up assessments, coordinating care with therapists and social workers, and documenting treatment plans. The exact mix of tasks shifts depending on whether the provider works in an outpatient clinic, inpatient unit, or telehealth setting.
- How many patients does a PMHNP see per day?
- Patient volume varies by practice setting and appointment type. In outpatient clinics, PMHNPs commonly see between 12 and 20 patients per day, with initial evaluations lasting 45 to 60 minutes and follow-ups running 15 to 30 minutes. Inpatient PMHNPs may round on a similar or larger panel, while telehealth providers can see slightly more patients because of reduced transition time between visits.
- Is being a PMHNP stressful?
- Psychiatric practice carries a real emotional toll. PMHNPs regularly work with patients in crisis, manage high acuity cases, and navigate complex medication regimens. Burnout prevention starts with employer-level supports like reasonable caseloads and clinical supervision, but individual strategies matter too. Regular peer consultation, clear boundaries between work and personal time, and dedicated self-care routines all help sustain a long, fulfilling career in psychiatric care.
- What is the difference between a PMHNP and a psychiatrist?
- Both diagnose and treat mental health disorders, but the training paths and practice models differ. A psychiatrist completes medical school and a four-year residency, while a PMHNP earns a master's or doctoral nursing degree with specialized psychiatric clinical hours. PMHNPs often spend more time per visit on holistic assessment and counseling. In many states, PMHNPs hold full practice authority and can prescribe independently.
- How long does it take to become a PMHNP?
- Starting from an active RN license, most nurses complete an MSN with a PMHNP specialization in two to three years. Programs designed for working nurses, like Gonzaga's online MSN-PMHNP track, offer flexibility through online coursework and extended clinical experiences. A BSN-to-DNP route typically takes three to four years. Adding time for certification exam preparation, most nurses can enter practice within roughly three years of starting their program.
- What is the work schedule of a psychiatric nurse practitioner?
- Schedules vary widely by setting. Outpatient PMHNPs often work standard weekday hours, typically 8 a.m. to 5 p.m., Monday through Friday. Telehealth roles may offer even more flexibility, with some providers setting their own hours. Inpatient and emergency psychiatric settings may involve 12-hour shifts, weekends, or on-call rotations. Many PMHNPs choose their setting specifically based on the schedule that best supports their work-life balance.