Most important takeaways…
- The U.S. faces a projected shortage of up to 86,000 physicians by 2036, accelerating NP demand nationwide.
- NPs in 27 states plus D.C. hold full practice authority, while others still require physician oversight agreements.
- Bureau of Labor Statistics data puts the median NP salary at $129,210, with 40 percent job growth projected through 2032.
- Telehealth now accounts for roughly 7 percent of primary care visits, and NPs lead a growing share of virtual encounters.
More than 355,000 nurse practitioners are currently practicing in the United States, and that number continues to climb as three powerful forces reshape the delivery of American healthcare: a rapidly aging population, a rising chronic disease burden, and persistent physician shortages concentrated in primary care and rural communities. The NP role is no longer supplementary. It is central to how patients access diagnosis, treatment, and ongoing management across hospitals, clinics, schools, and telehealth platforms.
The expansion is not uniform. State-level scope-of-practice laws, interdisciplinary team structures, and reimbursement models vary widely, creating a complex landscape for nurses considering advanced education. The evolving role of nurse practitioners reflects broader structural changes in how care is delivered. At the same time, evidence on patient outcomes, cost effectiveness, and job satisfaction continues to accumulate, offering a clearer picture of where the profession stands in 2026 and where it is headed.
Why the NP Role Is Expanding Across U.S. Healthcare
The Association of American Medical Colleges (AAMC) projects the United States could face a shortage of up to 86,000 physicians by 2036, with primary care gaps hitting rural and medically underserved communities hardest. Nurse practitioners are stepping directly into that void, and a convergence of demographic, legislative, and public health forces is accelerating the trend.
Aging Populations and Chronic Disease Are Driving Demand
As the Baby Boomer generation ages, the need for sustained, relationship-based primary care is climbing fast. More than 10,000 Americans turn 65 every day, and many of them are managing multiple chronic conditions: diabetes, heart disease, hypertension, COPD. According to a National University overview of advanced nursing trends, these aging population dynamics and the growing burden of chronic disease are core drivers behind the expanding NP role.1 Adult-gerontology nurse practitioners, in particular, are positioned to meet this surge because their training focuses on exactly these patient populations and the complex care coordination they require.
Legislative Momentum Toward Full Practice Authority
State legislatures have been steadily removing barriers that once limited what NPs could do independently. As of 2026, more than half of U.S. states and territories grant full practice authority for nurse practitioners, allowing them to evaluate patients, diagnose conditions, order tests, and prescribe medications without physician oversight. Several additional states have introduced or advanced legislation to follow suit. This legislative momentum does more than expand individual scope; it unlocks workforce capacity in regions where recruiting physicians has proven nearly impossible. For nurses weighing an NP career, the state-by-state trajectory points clearly toward broader autonomy and greater professional independence.
The Mental Health Crisis as a Growth Catalyst
Rising mental health needs represent another powerful expansion driver. Psychiatric mental health nurse practitioners (PMHNPs) are among the fastest-growing NP specialties nationwide, fueled by a behavioral health provider shortage that predates but was sharpened by the pandemic era. Many counties, particularly in rural areas, have no practicing psychiatrist at all. PMHNPs are filling those gaps across outpatient clinics, integrated care teams, telehealth platforms, and community health centers. Data on which states need nurse practitioners the most confirms that the psychiatric NP shortage remains especially acute in underserved regions.
What This Means for Your Career Path
These converging forces (physician shortages, demographic shifts, policy changes, and unmet mental health demand) are not temporary. They represent structural changes in how healthcare is delivered. For working nurses considering the next step, the expansion of the NP role is less a trend and more a long-term realignment of the healthcare workforce. Choosing the right NP specialty and the right program to prepare for it has never carried more weight.
What Nurse Practitioners Actually Do: Day-To-Day Across Settings
One of the most common misconceptions about nurse practitioners is that they function as physician assistants or play a supporting role in patient care. In reality, NPs diagnose conditions, order and interpret tests, prescribe medications, and manage treatment plans independently in a growing number of states. Understanding what that looks like across different clinical settings can help you figure out which specialty aligns with your strengths, your lifestyle, and the kind of impact you want to make.
Primary Care: Panels, Chronic Disease, and Continuity
A typical day for a primary care NP revolves around a patient panel of 15 to 25 visits. You might start the morning managing diabetes follow-ups, adjusting insulin regimens, and reviewing lab trends. By midday, you could be conducting a well-child exam, then counseling a patient on hypertension management. Afternoons often bring walk-in concerns, prescription refills, and referral coordination with specialists. The pace is steady rather than frantic, and the reward is longitudinal: you watch patients improve over months and years. Chronic disease management, including conditions like heart failure, COPD, and depression, is the backbone of this work. If you're weighing whether to pursue a generalist or specialist track, understanding the differences between acute care NP vs primary care NP roles is a useful starting point.
Acute and Emergency Care: Speed and Procedural Decision-Making
Contrast that with an acute care or emergency NP role, where the tempo is markedly different. You might intubate a patient, suture a laceration, and interpret a CT scan all before lunch. Triage decision-making is constant: determining which patients need immediate intervention, which can safely wait, and which require transfer to a higher level of care. Procedural skills matter here, and the clinical reasoning is compressed into minutes rather than scheduled appointments.
Telehealth: Virtual Visits and Remote Monitoring
Telehealth NPs have reshaped how care reaches patients, especially in rural and underserved communities. A virtual visit workflow typically involves a video consultation, chart review, e-prescribing, and follow-up messaging, all completed without a physical exam room. Remote patient monitoring adds another layer: reviewing blood pressure trends, glucose readings, or weight fluctuations transmitted from a patient's home device. The clinical thinking is the same as in-person care, but the communication skills shift. You rely more heavily on patient-reported symptoms, visual cues on camera, and precise documentation to guide treatment without hands-on assessment. For a deeper look at regulations and reimbursement, see our guide on telehealth for nurse practitioners.
Home Health and Long-Term Care: Geriatric Focus
NPs working in home health and long-term care settings often serve older adults with complex, overlapping conditions. A day might include conducting geriatric assessments in assisted living facilities, adjusting palliative care plans for patients with advanced illness, and coordinating with social workers, pharmacists, and family members. Care coordination is central to this role. You are frequently the clinician who synthesizes input from multiple providers and translates it into a plan the patient and family can actually follow. For adult-gerontology nurse practitioner professionals in particular, this setting offers some of the most meaningful, relationship-driven work in advanced practice nursing.
The Common Thread
Across every setting, the defining feature of the NP role is clinical autonomy. Whether you are managing a panel of diabetic patients in a community clinic, stabilizing a trauma patient in the emergency department, or conducting a telehealth visit from your home office, you are making diagnostic and prescribing decisions. In the majority of U.S. states that grant full practice authority, no supervising physician is required. This is not an assisting role. It is independent clinical practice built on advanced education and nursing expertise.
Questions to Ask Yourself
NP Scope of Practice: How It Varies by State
A nurse practitioner in Oregon can diagnose, treat, and prescribe independently from day one, while an NP with identical credentials in Texas must secure a physician's signature before writing certain prescriptions. That contrast shapes where you can practice, how you run your patient panel, and whether you can open your own clinic.
The Three Practice Authority Tiers
The American Association of Nurse Practitioners recognizes three classifications that describe how much autonomy state law grants NPs:1
- Full practice authority: NPs evaluate patients, diagnose conditions, order tests, and prescribe medications, including controlled substances, without a required collaborative agreement or physician oversight.
- Reduced practice: NPs can provide most clinical services but must enter a formal collaborative agreement with a physician or meet supervision requirements for at least one element of practice, often prescribing.
- Restricted practice: State law requires physician supervision, delegation, or team management for NPs to deliver care, limiting independent decision-making across the board.
As of 2026, 28 states plus the District of Columbia grant full practice authority.1 That number has grown steadily: six states moved into the full practice column between 2023 and 2026, including New York, Massachusetts, and Kansas. A decade ago, only 22 states offered this level of autonomy. For a complete breakdown, see our guide to nurse practitioner practice authority by state.
What Reduced Practice Looks Like Day to Day
In reduced or restricted states, collaborative agreements typically require an NP to identify a supervising or collaborating physician, submit documentation of the arrangement to the state board, and sometimes pay the physician a fee. Oversight can mean chart reviews, co-signatures on prescriptions for controlled substances, or periodic in-person meetings.
These requirements add administrative overhead and can limit where NPs work. Rural clinics without a nearby collaborating physician may struggle to hire NPs even when demand for care is high. Some NPs report that collaborative fees range from a few hundred to several thousand dollars per year, an expense that cuts into earnings or clinic budgets.
Why It Matters for Patients
Research consistently links full practice authority to improved healthcare access, particularly in underserved and rural areas. States that allow NPs to practice to the full extent of their training tend to have more primary care providers per capita in rural counties. Patients in those regions often face shorter wait times and travel fewer miles for routine and preventive care. Restricting NP autonomy does not improve safety metrics; it simply creates bottlenecks. These trends are closely tied to the evolving role of nurse practitioners across the broader healthcare system.
Check Your Target State Before You Enroll
If you plan to relocate after graduation or want the flexibility to open your own practice, research the practice environment in every state you are considering. Our ranking of the best states for nurse practitioners can help you compare pay, demand, and regulatory climate side by side. Scope of practice laws determine whether you can work independently, accept certain insurance panels without physician co-sign, or prescribe the full range of medications your patients need. Choosing a program is only half the equation. Understanding where you can actually use that credential shapes your long-term career options.
NP Vs. PA: How These Roles Compare in Modern Care Teams
Nurse practitioners and physician assistants both diagnose illness, order tests, prescribe medications, and manage patient care, yet they arrive at those responsibilities through fundamentally different training philosophies and practice frameworks. If you are weighing the two paths, or simply trying to understand where each fits on a modern care team, the distinctions matter more than their surface similarities suggest.
Training Model and Education
NPs are educated within a nursing model.1 The typical route runs from RN licensure through a Master of Science in Nursing or DNP, building on a foundation that emphasizes holistic, patient-centered care. Clinical training during graduate school generally ranges from 500 to 1,000 hours, layered on top of the hands-on nursing experience most students bring to the program.
PAs follow a medical model.1 Candidates usually enter a Master of Physician Assistant Studies program after completing a bachelor's degree, often with prerequisite healthcare experience. PA programs front-load clinical rotations more heavily, requiring roughly 2,000 supervised clinical hours before graduation.
Both pathways produce competent clinicians, but the educational lens shapes how each provider approaches a patient encounter. NPs tend to frame care around wellness, prevention, and the social determinants that influence a specific population. PAs are trained as generalists who can pivot across specialties under the medical model's diagnostic framework.
Certification and Recertification
NPs earn board certification through the American Academy of Nurse Practitioners Certification Board or the American Nurses Credentialing Center, depending on their specialty. Recertification is maintained through continuing education hours.1
PAs certify through the National Commission on Certification of Physician Assistants. Maintaining that credential requires both continuing medical education hours and a periodic recertification exam.1
Scope of Practice and Team Role
This is where the day-to-day experience diverges most. NPs practice under a population-focused philosophy, meaning their scope is tied to the patient population they were educated and certified to serve, such as family, adult-gerontology NP vs. acute care NP, or psychiatric mental health. In a growing number of states, NPs hold independent prescriptive authority and function as primary care providers without physician oversight.
PAs operate under a delegated authority model, meaning their prescriptive and practice privileges are extended by a supervising or collaborating physician. Within that arrangement, PAs serve as team-based clinicians who often rotate across specialties throughout their careers. Understanding how to build an NP-led care team can clarify the practical differences these models create in daily workflows.
Which Path Fits You?
Neither role is universally "better." Consider these key differences when deciding:
- Practice independence: NPs can practice autonomously in full-practice-authority states; PAs generally require a collaborative agreement with a physician.
- Specialty commitment: NP certification is population-specific from the start; PAs can shift specialties more fluidly.
- Prior nursing experience: If you are already a registered nurse, the NP pathway builds directly on the skills and clinical judgment you use every day.
- Team preference: PAs are trained for tightly integrated physician-led teams; NPs increasingly lead their own panels and clinics.
For working nurses considering advanced practice, the NP route offers a natural progression that leverages years of bedside experience while opening the door to autonomous, population-focused care. You can explore how these scope-of-practice nuances play out state by state later in this guide.
Related Articles
NP Impact on Patient Outcomes, Access, and Cost
The central question every health system and policy maker weighs is whether expanding the NP workforce improves patient outcomes and lowers costs without compromising quality. The evidence is nuanced, context-dependent, and sometimes contradictory. Recent studies show that NP-led care can match physician outcomes in many settings while improving access and lowering professional fees, but certain contexts reveal tradeoffs in utilization and downstream spending.
Are Nurse Practitioners as Effective as Doctors?
In outpatient primary care and chronic disease management, multiple studies from the past five years demonstrate that NP-led care produces comparable or superior outcomes on key clinical metrics. Patient satisfaction data from 2024 studies consistently place NP care at 89 to 96 percent satisfaction rates, reflecting strong communication, shared decision-making, and time spent with patients.3 For chronic conditions such as diabetes and hypertension, research shows NPs achieve equivalent glycemic control (measured by HbA1c) and blood pressure targets when managing patients within their scope.
Readmission rates for NP-managed patients in community health centers and rural clinics show no significant difference compared to physician-managed cohorts in published comparative analyses. In many underserved areas, the presence of a primary care nurse practitioner is the difference between timely care and no care at all, making direct comparisons less relevant than baseline access improvements.
A 2012 analysis of Medicare beneficiaries found that outpatient visits led by NPs cost 67.7 percent less in professional fees than physician-led visits, a figure that remains relevant as reimbursement models shift toward value and efficiency.2 This cost advantage is most pronounced in preventive care, routine follow-up, and stable chronic disease management.
Emergency and Complex Care: A More Complicated Picture
Not all settings yield the same outcomes. A three-year study published in 2022 examining Veterans Health Administration emergency departments found that when NPs were the sole provider for initial assessment, patients experienced an 11 percent increase in ED length of stay, a 20 percent rise in preventable hospitalizations, and 15 percent higher total health spending (an additional $238 per encounter on average).1 Per-visit costs rose by 7 percent, or roughly $66. These increases suggest that in high-acuity, time-sensitive environments without direct physician collaboration, NP autonomy may correlate with higher resource utilization and downstream costs.
This does not imply NPs are less capable, but rather that care complexity, team structure, and institutional support matter enormously. The same study did not find comparable increases in NP-physician team models, where collaborative protocols and real-time consultation were standard.
Wait Times and Access Gains
Clinics that add NPs to their provider roster see measurable reductions in appointment wait times. While specific figures vary by region and specialty, health systems report average wait-time drops of 15 to 30 percent when NP positions are filled in primary care or specialty clinics. In rural and underserved communities, the addition of a single NP can reduce wait times from weeks to days, improving continuity and preventive care adherence. Understanding the impact of nurse practitioners on health care helps put these access gains in a broader workforce context.
What the Evidence Means for You
NPs deliver high-quality, cost-effective care in the majority of outpatient and community-based settings. The value proposition is clearest in primary care, chronic disease management, and rural practice. In complex, high-acuity environments, collaborative models outperform independent practice on both outcomes and cost. As you consider your future NP role, understanding these context-specific findings will help you choose practice settings where your training, autonomy, and team structure align with the best patient outcomes.
NP-Led Care by the Numbers
Research consistently shows that nurse practitioners deliver high-quality, cost-effective care across settings. Here is a snapshot of the data shaping the NP landscape in 2026.

NP Salary and Job Growth: What the Data Shows
Nurse practitioners are among the fastest-growing occupations in the United States, and the compensation data reflects that demand. According to the Bureau of Labor Statistics, the median annual wage for NPs reached $129,210 as of 2024, with top earners surpassing $149,570. Meanwhile, BLS projections estimate roughly 32,700 annual openings for nurse practitioners, nurse anesthetists, and nurse midwives through 2034, driven by retiring clinicians, expanding scope of practice laws, and surging patient demand in primary care, behavioral health, and geriatrics.
| Metric | Value |
|---|---|
| Total NP Employment (2024 BLS) | 307,390 |
| Median Annual Wage | $129,210 |
| Mean Annual Wage | $132,000 |
| 25th Percentile Wage | $109,940 |
| 75th Percentile Wage | $149,570 |
| Projected Job Growth Rate (2022 to 2032) | 45% |
| Projected New NP Jobs (2022 to 2032) | 118,600 |
| Projected Job Growth Rate, NPs/CRNAs/CNMs (2024 to 2034) | 35% |
| Projected Annual Openings, NPs/CRNAs/CNMs (2024 to 2034) | 32,700 |
| NPs Prepared in Primary Care | 90% |
| Growth Ranking Among All Occupations (2024 to 2034) | 3rd |
Highest-Paying States for Nurse Practitioners
Where you practice can significantly affect your earning potential as a nurse practitioner. The table below shows the top 15 states (and the District of Columbia) ranked by median annual salary, based on the most recent Occupational Employment and Wage Statistics from the U.S. Bureau of Labor Statistics (2024 data). California leads by a wide margin, with a median salary more than $30,000 above the next highest state.
| State | Total NPs Employed | Median Annual Salary | 25th Percentile | 75th Percentile | Mean Annual Salary |
|---|---|---|---|---|---|
| California | 20,980 | $166,610 | $140,260 | $205,400 | $173,190 |
| New Jersey | 9,590 | $149,620 | $126,030 | $162,250 | $140,470 |
| Alaska | 570 | $145,450 | $104,000 | $165,510 | $142,340 |
| New York | 20,430 | $145,390 | $128,190 | $164,670 | $148,410 |
| Oregon | 2,430 | $144,600 | $129,840 | $163,240 | $148,030 |
| Washington | 4,790 | $140,220 | $125,890 | $161,730 | $143,620 |
| Connecticut | 3,680 | $138,960 | $125,910 | $159,680 | $141,140 |
| Massachusetts | 8,920 | $138,890 | $125,590 | $160,310 | $145,140 |
| New Mexico | 1,870 | $138,440 | $113,240 | $156,000 | $136,620 |
| Arizona | 7,540 | $133,790 | $115,290 | $151,650 | $132,920 |
| Montana | 1,050 | $133,640 | $112,180 | $141,050 | $131,560 |
| New Hampshire | 1,790 | $132,440 | $120,270 | $143,010 | $133,660 |
| District of Columbia | 790 | $131,380 | $119,240 | $143,960 | $137,600 |
| Hawaii | 470 | $130,940 | $121,410 | $158,100 | $135,020 |
| Rhode Island | 1,200 | $130,710 | $126,200 | $160,030 | $139,600 |
Telehealth, AI, and Interdisciplinary Care: Where the NP Role Is Heading
As of April 2026, telehealth encounters account for 6.9 percent of primary care visits nationally, a figure that has held steady in the 6-7 percent range since mid-2023.1 While the pandemic spike has normalized, telehealth remains a durable channel for care delivery, and nurse practitioners are uniquely positioned to lead in this space.
Telehealth Use Across Specialties
Physician telehealth adoption data from 2024 shows 71.4 percent of physicians used telehealth at least once per week, with 15.7 percent reporting high-volume usage.2 NPs, particularly those in primary care, psychiatry, and chronic disease management, report similar or higher utilization rates. The American Medical Association has backed the CONNECT for Health Act of 2025, federal legislation that would expand telehealth access and maintain reimbursement parity for remote services, including those delivered by nurse practitioners.3
For real-time policy updates, start with the American Association of Nurse Practitioners (AANP) research page, which publishes annual telehealth utilization surveys and tracks state and federal rule changes. The AANP also maintains policy alerts that flag scope-of-practice and reimbursement shifts as they happen.
Reimbursement and Prescribing Rules
CMS updates its telehealth policies annually in the Physician Fee Schedule final rule. For a closer look at how reimbursement works in practice, our primary care billing and coding guide breaks down NP-specific scenarios. The 2025 proposed repeal of the in-person requirement for Medicare telemental health visits, if finalized, would further expand the NP role in psychiatric care.3
State-level telehealth prescribing policies vary widely, especially for controlled substances. The DEA enforces the Ryan Haight Act, which restricts online prescribing of controlled medications. Exemptions introduced during the public health emergency remain subject to review. For the latest state rules, use the Telehealth Resource Centers and the National Conference of State Legislatures (NCSL) telehealth policy tracker. DEA.gov provides updates on controlled substance prescribing via telehealth. NPs who want to advocate for better prescribing rules can also explore our nurse practitioner health policy toolkit for practical steps.
AI and Interdisciplinary Integration
Artificial intelligence tools are beginning to support NP workflows, from ambient documentation that auto-generates visit notes to predictive algorithms that flag patients at risk for chronic disease exacerbation. NPs working in team-based care models, particularly those embedded in federally qualified health centers and hospital systems, are integrating AI-driven decision support into their daily practice.
Interdisciplinary care is no longer optional. NPs increasingly co-manage patients with physicians, pharmacists, social workers, and care coordinators, using shared electronic health records and population health dashboards. This team-based model, supported by value-based payment contracts, allows NPs to practice at the top of their license while improving outcomes and reducing redundant visits. Understanding full practice authority states can help you identify where these collaborative models offer the greatest autonomy.
To stay current, subscribe to AANP policy alerts, follow CMS Telehealth Updates newsletters, and set up alerts for NP telehealth state policy. The landscape shifts quickly, and NPs who monitor these channels can adapt their practice before regulatory changes take effect.
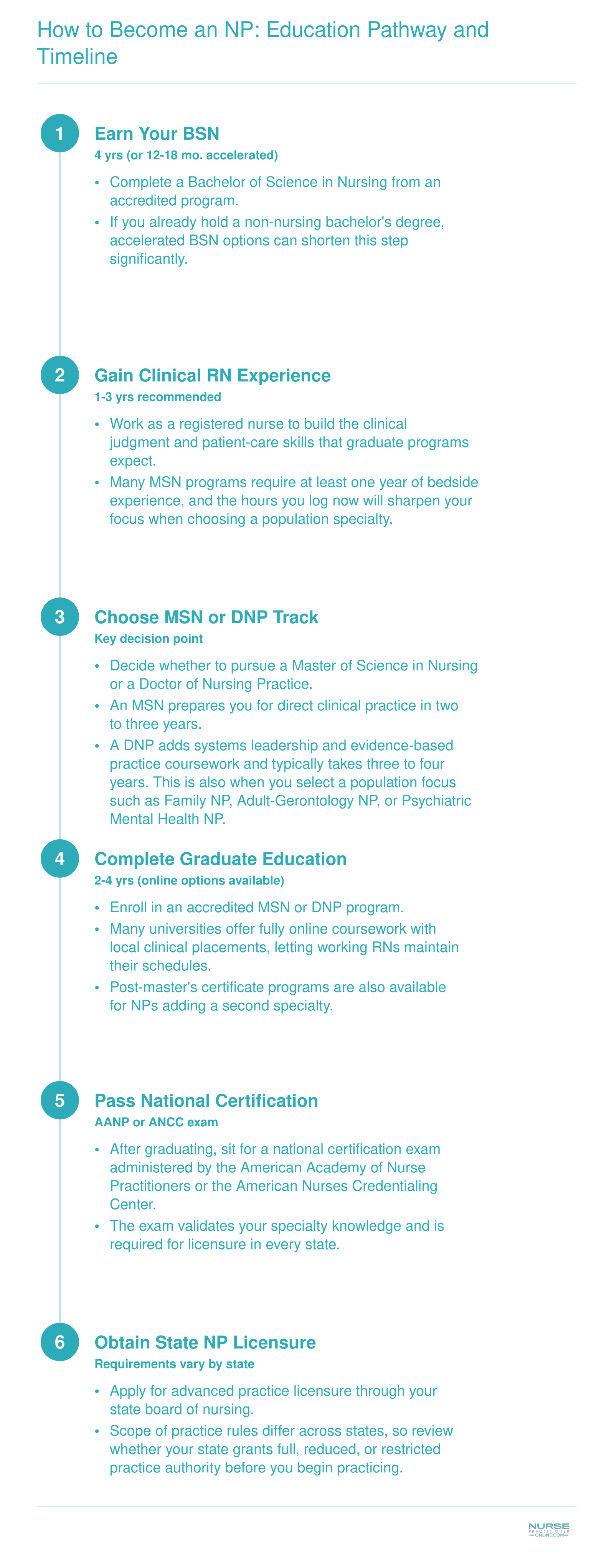
How to Become an NP: Education Pathway and Timeline
The journey from registered nurse to nurse practitioner follows a clear, step-by-step progression. While the exact timeline depends on your starting point and whether you choose full-time or part-time study, most working RNs can expect to spend roughly six to ten years moving from a BSN through certification and licensure. Online MSN and post-master's certificate programs make it possible to keep working while you advance.
Common Questions About the NP Role in Healthcare
Whether you are just beginning to explore advanced practice nursing or actively weighing program options, these frequently asked questions cover the essentials. Each answer draws on the data and analysis discussed throughout this guide.
- What is the role of a nurse practitioner in modern healthcare?
- Nurse practitioners diagnose and treat acute and chronic conditions, order and interpret diagnostic tests, prescribe medications, and coordinate patient care across settings. In 2026, NPs serve as primary care providers in clinics, hospitals, specialty practices, and telehealth platforms. Their training blends clinical expertise with a patient-centered, preventive focus that positions them as key contributors to closing provider gaps nationwide.
- Are nurse practitioners as effective as doctors?
- Multiple peer-reviewed studies show that NP-led primary care produces patient outcomes, including satisfaction scores and chronic disease management results, comparable to those of physician-led care. As discussed earlier in this article, research consistently finds no significant difference in quality metrics when NPs practice to the full extent of their education. NPs also tend to spend more time on patient education and preventive counseling.
- How long does it take to go from RN to nurse practitioner?
- Most registered nurses complete a Master of Science in Nursing (MSN) in two to three years of full-time study, or three to four years part-time. A Doctor of Nursing Practice (DNP) typically adds one to two years beyond the MSN. Online and hybrid programs, like those highlighted on nursepractitioneronline.com, offer flexible scheduling so working nurses can advance without leaving the bedside.
- How does NP scope of practice vary by state?
- NP authority ranges widely across the United States. Full practice authority states allow NPs to evaluate, diagnose, and prescribe independently. Reduced practice states require a collaborative agreement with a physician, and restricted practice states mandate direct physician oversight. As of 2026, the trend continues toward expanding full practice authority, with more states removing supervisory requirements each legislative session.
- What is the difference between a nurse practitioner and a physician assistant?
- NPs are educated in a nursing model that emphasizes holistic, patient-centered care, while PAs train under a medical model with a broader, generalist foundation. NPs choose a population focus (such as adult-gerontology or family) during their graduate program, whereas PAs typically specialize after graduation. Licensing, prescriptive authority, and supervision requirements also differ by state, as outlined earlier in this guide.
- What impact do NPs have on healthcare costs and patient access?
- NPs improve access by practicing in underserved and rural communities where physician shortages are most acute. Studies show NP-delivered primary care can reduce per-visit costs and lower emergency department utilization. As aging populations and rising chronic disease rates drive demand, NPs help health systems stretch limited resources while maintaining quality, making them a cost-effective solution to growing provider shortages.