Most important takeaways…
- Acute care NPs manage high-acuity patients in hospitals, while primary care NPs build long-term relationships in outpatient settings.
- Certification defines your legal scope: you cannot practice outside your certified population focus under the AACN Consensus Model.
- The national median NP salary was $129,210 as of the latest BLS data, though pay varies widely by state and setting.
- BLS projects 40% NP job growth through 2033, creating strong demand across both acute and primary care tracks.
The NP track you select during graduate school locks in your certification, your legal scope of practice, and the patient populations you can treat for the rest of your career. That single admissions decision separates two fundamentally different clinical worlds: acute care NPs manage episodic, complex, and critical illness in hospital and specialty settings, while primary care NPs (most commonly FNPs) build longitudinal relationships around wellness, prevention, and chronic disease management across the lifespan.
With state licensing boards increasingly enforcing the AACN Consensus Model, crossing from one track to the other after graduation typically means earning a second master's degree or post-graduate certificate. The stakes of choosing correctly have never been higher.
What Is an Acute Care NP Vs. A Primary Care NP?
The distinction between acute care and primary care nurse practitioners is not about where you work. It is about the population focus and clinical competencies you gain during graduate education, and the scope of practice you are authorized to carry afterward.
Acute Care NP: Managing Complex, Acute, and Critical Illness
An acute care nurse practitioner is educated and certified to manage patients experiencing complex acute illness, critical injury, or exacerbations of chronic disease. The American Association of Colleges of Nursing (AACN) and the National Organization of Nurse Practitioner Faculties (NONPF) define acute care NP preparation as focused on physiologic instability, advanced diagnostic reasoning, and interventions for patients across the lifespan or within the adult-gerontology population. Acute care NPs work in settings where patients require continuous monitoring, rapid intervention, and multidisciplinary coordination, including intensive care units, surgical services, emergency departments, specialty inpatient units, and hospitalist teams. Many of these roles overlap with the critical care nurse practitioner path. The acute care designation does not mean you only work in the ER; it means you are trained to manage unstable or rapidly changing conditions wherever they occur.
Primary Care NP: Health Promotion, Prevention, and Chronic Disease Management
Primary care nurse practitioners, by contrast, are prepared to provide comprehensive care across the wellness-to-illness continuum in outpatient or community-based settings. Family nurse practitioners (FNP) and adult-gerontology primary care NPs (AGPCNP) fall into this category. According to AACN and NONPF consensus standards, primary care NPs focus on health promotion, disease prevention, risk reduction, and management of stable chronic conditions. They conduct annual physicals, manage hypertension and diabetes, order screenings, provide counseling, and coordinate care for patients who are medically stable. Primary care does not mean you only work in family medicine clinics; primary care NPs also staff urgent care, occupational health, retail clinics, telehealth platforms, and community health centers.
The Population-Focus Model: Regulatory Backbone Since 2008
The 2008 AACN Consensus Model for APRN Regulation established the population-focus framework that now governs NP education and licensure across the United States. Under this model, your graduate program and certification exam must align with one of six population foci: family/individual across the lifespan, adult-gerontology acute care, adult-gerontology primary care, pediatric acute care, pediatric primary care, or neonatal. To understand one of these tracks in depth, explore the adult-gerontology nurse practitioner role and scope of practice. This framework ensures that your clinical training, scope of practice, and legal authority to diagnose and prescribe are tied to the patient populations and acuity levels you are competent to manage. Regulatory boards, certification bodies, and employers all use this population-focus language to determine where and how you can practice.
Scope of Practice: How Certifications Define Where You Can Work
Choosing ANCC certification versus AACN certification shapes not just your exam experience but your entire career trajectory. Both pathways lead to acute care credentials, yet the certifying body you select influences your eligibility requirements, renewal process, and how employers perceive your qualifications. Understanding the full nurse practitioner licensing landscape is essential before committing to either route.
The Two Main Certifying Bodies
The American Nurses Credentialing Center (ANCC) offers certifications spanning acute and primary care populations. For acute care, the Adult-Gerontology Acute Care Nurse Practitioner Board Certified (AGACNP-BC) credential requires graduation from an accredited graduate program with at least 500 supervised clinical hours.1 The exam consists of 175 questions over 3.5 hours, with a passing score of 350.2 Recent data shows approximately 80 percent of candidates pass on their first attempt.1 Certification remains valid for five years, requiring 75 continuing education hours (including 25 in pharmacology) for renewal. The exam fee runs $395.2
For primary care tracks, ANCC offers the Family Nurse Practitioner Board Certified (FNP-BC) and Adult-Gerontology Primary Care Nurse Practitioner Board Certified (AGPCNP-BC) credentials, following similar eligibility and renewal structures.
The American Association of Critical-Care Nurses (AACN) offers the Acute Care Nurse Practitioner Certified in Adult-Gerontology (ACNPC-AG) credential. This exam also includes 175 questions over 3.5 hours and requires 500 clinical hours.4 The AACN pathway reports a higher pass rate of approximately 91 percent based on 2023 data.3 Exam fees range from $270 for members to $375 for non-members, with candidates limited to four attempts.3
Legal Consequences of Practicing Outside Your Scope
This is the critical issue many prospective NPs overlook: your certification legally defines where and how you can practice. An acute care NP who routinely manages stable primary care patients operates outside their certified scope. The consequences are serious.
State boards of nursing can impose discipline ranging from mandatory remediation to license suspension. Malpractice insurers may deny coverage for claims arising from out-of-scope practice, leaving you personally liable. Employers face their own exposure when they assign NPs to patient populations mismatched with their certification. Hospital credentialing committees scrutinize this alignment carefully, and violations can jeopardize an entire facility's accreditation.
State Scope of Practice Landscape in 2025-2026
As of 2026, roughly half of U.S. states grant full practice authority to nurse practitioners, allowing independent practice without physician oversight. The remaining states maintain reduced or restricted practice environments requiring varying degrees of collaborative agreements or supervision.
Here is where it gets nuanced for acute versus primary care NPs: full practice authority primarily affects outpatient and community settings. Hospital-based acute care NPs typically work under institutional bylaws and credentialing requirements regardless of state law. A primary care nurse practitioner in a full-practice state might open an independent clinic, while an acute care NP in that same state still operates within hospital protocols and collaborative frameworks.
Certification Determines Reimbursement Eligibility
Even in states with the most permissive scope-of-practice laws, certification dictates reimbursement. The Centers for Medicare and Medicaid Services (CMS) and private insurers require NPs to bill only for services aligned with their certified population focus. An FNP cannot bill Medicare for acute care services rendered in an ICU setting, regardless of clinical competence or state authorization.
This reimbursement reality constrains employers. A rural hospital might prefer hiring one NP to cover both the emergency department and outpatient clinic, but payer rules make this impractical. Understanding this dynamic helps you recognize why job postings specify certification types so precisely.
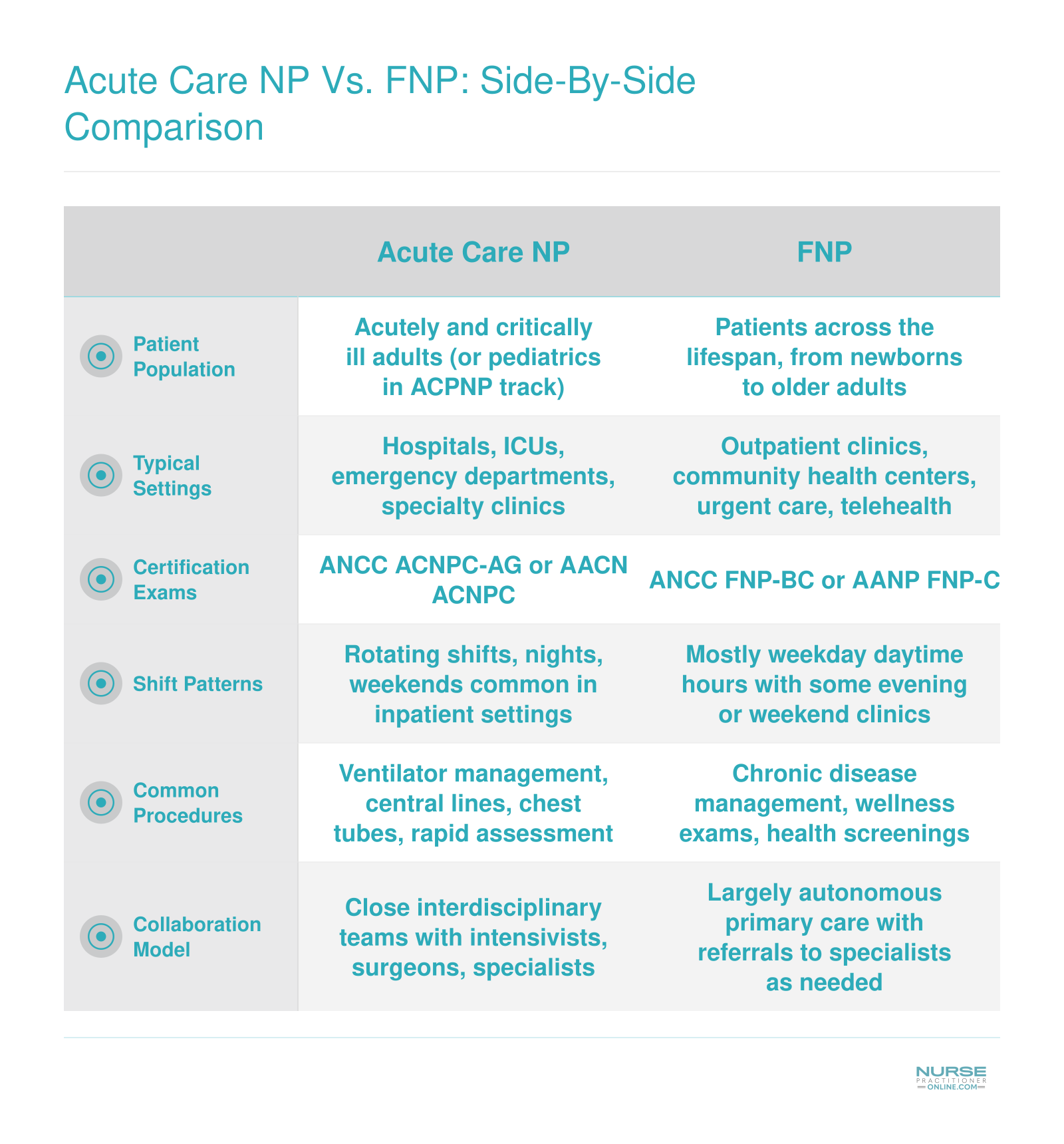
Acute Care NP Vs. FNP: Side-By-Side Comparison
This quick-reference table highlights the core differences between acute care nurse practitioners and family nurse practitioners. Bookmark it for easy comparison as you weigh your options.
Day-To-Day: What Each Role Really Looks Like
The central tension here is intensity versus continuity. Acute care NPs work at a higher pitch, managing fewer patients with far greater acuity, while primary care NPs sustain longer-term relationships across a much larger patient panel. Both are demanding, just in different ways.
The Acute Care NP Workday
Expect 12-hour shifts, and plan for some of those to stretch to 13 or 15 hours when a critical patient is mid-workup at shift change.1 Most acute care nurse practitioner roles involve three shifts per week, which sounds manageable until you account for weekends and holidays, both of which come with the territory.2 Some hospitalist and nocturnist programs run a 7-on/7-off pattern that clusters your work and your time off in full-week blocks.
Patient loads vary by unit. In the ICU, you might be responsible for six to twelve patients, each with a complex, rapidly evolving picture. On a hospitalist or medical-surgical service, that number climbs to ten to eighteen. In the ED or an observation unit, you could move through fifteen to twenty-five patients in a single shift.1 The common thread is high acuity at every turn: rounding with intensivists or hospitalists, assisting with procedures like central line placements and chest tubes, interpreting labs and imaging in real time, and shouldering a significant documentation burden inside the EMR. Call expectations range from in-house overnight coverage to home call, depending on the facility and specialty.2
The Primary Care NP Workday
Primary care runs on a different rhythm entirely. Clinic hours are typically eight to ten hours, Monday through Friday, with no mandatory weekends or holidays.2 Your patient panel may range from 800 to 1,500 individuals, and on any given day you will see eighteen to twenty-four of them. Practices serving complex populations, such as geriatric or underserved panels, often cap that at twelve to eighteen to allow more time per visit.1
A typical morning might move from a well-child exam to a diabetes follow-up to a new hypertension diagnosis, then back to a Medicare Annual Wellness Visit. After-hours call is usually phone triage only. Some clinics rotate one evening session or a Saturday morning among providers, but that is the exception rather than the rule.
Where Work-Life Balance Really Differs
The tradeoff is structural. A three-shift acute care schedule can feel freeing on your four days off, but those shifts are physically and cognitively exhausting, and weekend or holiday rotation is non-negotiable. A Monday-through-Friday clinic schedule offers predictability and protected evenings, but the patient volume and documentation load that accumulates across a large panel adds up quickly. Neither path is easy. The question is which type of demand fits your life right now, and if you are leaning toward the acute side, exploring acute care np programs can help you compare curriculum options before you commit.
Comparing NP Specialties by Care Setting
Which NP specialty actually works in which care setting, and how do acute and primary care distinctions shape each certification?
The acute-versus-primary framework runs through nearly every nurse practitioner population focus, not just adult-gerontology. Each specialty certification determines where you can work and the patient acuity you manage. Understanding this structure helps you see how the track you choose during your NP program will map directly onto your day-to-day clinical environment.
Adult-Gerontology: Two Tracks, Two Worlds
Adult-Gerontology Primary Care NPs focus on preventive and chronic care for adults in outpatient settings such as primary care offices, community health centers, and long-term care facilities. Adult-Gerontology Acute Care NPs, by contrast, manage complex, unstable adult patients in hospitals, intensive care units, and emergency departments. The certifications are distinct and not interchangeable. According to the American Nurses Association, these two tracks require separate exams and clinical training because scope of practice differs significantly.1
Family NP: Always Primary Care
Family Nurse Practitioners hold a primary care certification spanning all ages. Typical settings include family practice clinics, community health centers, urgent care, schools, and rural or underserved areas. The University of Rochester notes that FNPs do not hold acute care credentials and therefore work outside hospital inpatient units unless hired into roles that fall within their outpatient scope.2
Pediatric and Neonatal: Acute and Primary Options
Pediatric Primary Care NPs provide well-child care, immunizations, and chronic disease management in outpatient pediatric practices. Pediatric Acute Care NPs (less common) work in pediatric hospitals and EDs managing critically ill children. If you are drawn to this path, exploring online PNP programs can help you compare your options. Neonatal NPs always work in acute settings, specifically neonatal intensive care units caring for critically ill newborns.3
Psychiatric-Mental Health: The Exception
Psychiatric-Mental Health NPs cross both acute and primary care boundaries. They work in outpatient clinics, private practice, telehealth, and inpatient psychiatric units. PMHNPs manage both stable ongoing mental health needs and acute psychiatric crises, making the population focus more flexible than most.4
Emergency and Women's Health
Emergency NPs specialize in acute unscheduled care in emergency departments and urgent care centers. Women's Health NPs focus on primary and preventive reproductive care in OB/GYN offices, addressing prenatal, postpartum, and gynecologic needs. These roles rarely overlap with other population foci due to highly specialized scopes of practice.5 Compensation also varies considerably across these specialties, so reviewing NP salaries by specialty can help you weigh financial factors alongside clinical interest.
Salary and Job Outlook: Acute Care NP Vs. Primary Care NP
The Bureau of Labor Statistics groups all nurse practitioners under a single occupational code, so it does not break out pay by acute care versus primary care specialty. The national median annual wage for nurse practitioners was $129,210 as of May 2024, with total employment of roughly 307,390. The BLS projects 40 percent job growth for NPs from 2024 to 2034, making this one of the fastest growing occupations in healthcare. Specialty-specific compensation surveys, such as those published by AANP and Medscape, generally show that acute care NPs earn modestly higher median pay than family or primary care NPs, largely reflecting the acuity and hospital-based settings in which they practice. However, program-level specialty salary breakdowns are not yet available in the current public data, so the table below focuses on verified national figures.
| Metric | Nurse Practitioners (National, May 2024) |
|---|---|
| BLS Occupational Code | 29-1171 |
| Total Employment | 307,390 |
| Median Annual Wage | $129,210 |
| 25th Percentile Wage | $109,940 |
| 75th Percentile Wage | $149,570 |
| Mean Annual Wage | $132,000 |
| Projected Job Growth (2024 to 2034) | 40% |
NP Salary by State
Nurse practitioner salaries vary significantly depending on where you practice. The table below shows median annual wages for NPs across 25 states, drawn from the latest Bureau of Labor Statistics data. Keep in mind that these figures reflect all nurse practitioners in each state, not just acute care or primary care tracks. Much of the variation comes down to local cost of living and scope of practice regulations. States that grant NPs full practice authority, for example, sometimes see higher compensation because NPs can operate more independently and bill directly.
| State | Total NPs Employed | Median Annual Salary | 25th Percentile | 75th Percentile |
|---|---|---|---|---|
| California | 20,980 | $166,610 | $140,260 | $205,400 |
| New Jersey | 9,590 | $149,620 | $126,030 | $162,250 |
| Alaska | 570 | $145,450 | $104,000 | $165,510 |
| New York | 20,430 | $145,390 | $128,190 | $164,670 |
| Oregon | 2,430 | $144,600 | $129,840 | $163,240 |
| Washington | 4,790 | $140,220 | $125,890 | $161,730 |
| Connecticut | 3,680 | $138,960 | $125,910 | $159,680 |
| Massachusetts | 8,920 | $138,890 | $125,590 | $160,310 |
| New Mexico | 1,870 | $138,440 | $113,240 | $156,000 |
| Arizona | 7,540 | $133,790 | $115,290 | $151,650 |
| Montana | 1,050 | $133,640 | $112,180 | $141,050 |
| New Hampshire | 1,790 | $132,440 | $120,270 | $143,010 |
| District of Columbia | 790 | $131,380 | $119,240 | $143,960 |
| Hawaii | 470 | $130,940 | $121,410 | $158,100 |
| Rhode Island | 1,200 | $130,710 | $126,200 | $160,030 |
| Texas | 21,690 | $129,880 | $110,570 | $143,860 |
| Colorado | 4,130 | $129,750 | $110,300 | $139,440 |
| Vermont | 680 | $129,740 | $115,650 | $139,930 |
| Iowa | 2,810 | $129,420 | $115,950 | $137,900 |
| Florida | 24,690 | $129,010 | $109,670 | $143,670 |
| Idaho | 1,570 | $128,940 | $119,290 | $140,920 |
| Illinois | 9,560 | $128,620 | $111,450 | $138,420 |
| Wisconsin | 4,950 | $128,580 | $117,630 | $137,150 |
| Minnesota | 8,690 | $128,570 | $103,250 | $139,590 |
| Indiana | 7,470 | $128,280 | $111,210 | $134,840 |
Education Pathways: Curriculum, Clinical Hours, and Prerequisites
Your choice of NP track dictates which classrooms, simulation labs, and clinical sites you will spend the next two to four years inside. Acute care and primary care programs share a common graduate nursing foundation, but they diverge sharply once you enter specialty coursework, and the gap widens further at the clinical placement stage.
Shared Core, Divergent Specialty Courses
Both MSN tracks build on the same graduate-level foundation: advanced pathophysiology, advanced pharmacology, advanced health assessment (often called "the three Ps"), plus research methods, healthcare policy, and population health. After that core, the curricula split.
Acute care NP programs layer in critical care pharmacology, hemodynamic monitoring, ventilator and airway management, invasive procedures (central lines, chest tubes, arterial lines), and management of complex multi-system disease. Family and primary care NP programs emphasize well-child and well-woman care, preventive screening, chronic disease management across the lifespan, behavioral health integration, and patient education for long-term self-management.
Clinical Hour Requirements
Accredited NP programs require a minimum of 500 to 750 direct patient care hours at the MSN level, with most programs landing between 600 and 750. DNP programs typically require 1,000+ hours total. The setting is what matters:
- Acute care placements: ICU, ED, step-down, rapid response, and inpatient specialty services such as cardiology or trauma.
- Primary care placements: family medicine clinics, pediatric offices, community health centers, women's health, and student health.
Programs generally will not let you swap settings to fit your schedule. An acute care student cannot log primary care hours toward certification eligibility, and vice versa.
MSN vs. DNP
The DNP adds roughly 12 to 24 months and a scholarly project or residency focused on systems leadership, quality improvement, or evidence translation. It does not expand your legal scope of practice: an acute care DNP and an acute care MSN sit for the same certification exam. If you are considering a DNP AGNP pathway, choose it when you want leadership, faculty, or policy roles, or if you are entering the field now and want to match the AACN's long-stated push toward DNP as the entry credential.
Ideal RN Background
Admissions committees and clinical preceptors look for relevant bedside experience. ICU, ED, PACU, or step-down nurses are well-positioned for acute care tracks. Med-surg, ambulatory, school health, public health, and home health nurses bring the assessment and counseling skills primary care programs reward. Nurses interested in younger populations may also explore pediatric nurse practitioner roles, which span both acute and primary care tracks.
Can an Acute Care NP Work in Primary Care (And Vice Versa)?
With the AACN Consensus Model now fully integrated into state licensing laws, the line between acute care and primary care NP practice is clearer, and less flexible, than ever before. The straightforward answer is no: you cannot legally work outside your certified population focus. Even if your clinical skills overlap, practicing in a setting that doesn't match your certification violates both national board standards and most state nursing board regulations.
The Consensus Model and State Board Enforcement
The Consensus Model explicitly ties NP certification to a specific patient population and care setting. An acute care NP is educated and certified to manage patients with unstable, complex, or critical conditions, typically in hospitals or ICUs. A primary care NP, like an FNP, is prepared for continuous, comprehensive care across the lifespan in outpatient settings. Crossing that line, no matter how experienced you are, puts your license at risk. State boards have issued advisories and, in documented cases, disciplined NPs who practiced outside scope. During credentialing, employers verify your certification matches the role, and insurers may deny claims if the provider isn't deemed qualified.
The Legitimate Crossover: Post-Master's Certificate Pathway
If you want to switch tracks, the only recognized route is a post-master's certificate. These programs build on your existing graduate degree and add the necessary didactic and clinical hours for the new population focus.1 Expect 20 to 30 additional credit hours and 360 to 750 clinical hours, depending on the program. For example, East Carolina University's AGACNP certificate requires 20 credits2, while the University of New Hampshire's version demands 30 credits and 750 clinical hours.3 George Washington University's program falls in the middle at 20 credits and 600 clinical hours.4 Most working nurses complete these part-time in 3 to 6 semesters, roughly 1 to 2 years. You'll need an MSN, DNP, or PhD in nursing as a prerequisite, and programs are available fully online with local clinical placements. You can compare options across schools in our roundup of online post-master's ACNP certificate programs, or explore post master's certificate FNP programs if you're heading in the primary care direction.
PMHNP Exception and Dual Certification
One notable exception is the Psychiatric-Mental Health NP (PMHNP). Because the PMHNP population focus is not defined by acute or primary care labels, these NPs can typically practice across outpatient, inpatient, and telehealth settings without a separate certification. For NPs who want the broadest scope, dual certification is an option, earning both AGACNP and FNP, for instance, but this requires completing two distinct certification pathways and maintaining both.
Telehealth: A Gray Area
Some acute care NPs perform post-discharge virtual follow-ups, and many primary care NPs staff telehealth urgent care platforms. Legally, your certification scope still applies. If a patient's condition escalates into an acute or critical presentation, the primary care NP may be practicing outside scope unless they have appropriate protocols and backup. Boards have not issued a blanket ruling, so review your state practice act carefully before taking on a hybrid role.
How to Choose: A Decision Framework for Working Nurses
The Bureau of Labor Statistics projects a 40% growth in NP jobs through 2033, but where those jobs appear, and how they fit your life, depends on the specialty track you choose. RNs making this decision benefit from a structured self-assessment across four dimensions: clinical interests, lifestyle priorities, state practice environments, and long-term career goals.
Assess Your Clinical Interests and Patient Acuity Preference
Your day-to-day satisfaction hinges on the type of patients you find most energizing. If you thrive on rapid clinical decision-making, complex acute conditions, and hospital-based teamwork, the acute care NP path aligns with that drive. These roles demand comfort with unpredictable shifts, invasive procedures, and high-acuity scenarios.
- Acute care orientation: You enjoy managing pressing inpatient problems, interpreting real-time diagnostics, and stabilizing patients in fast-paced units.
- Primary care orientation: You prefer building sustained relationships, emphasizing prevention, and managing chronic conditions across the lifespan in outpatient settings.
Evaluate Lifestyle, Scheduling, and State Practice Laws
Your personal life and geographic location play an outsized role. Many acute care NP positions require rotating shifts, on-call coverage, and weekend or holiday work, while primary care roles more often offer predictable weekday schedules. However, this varies by employer.
- Scheduling: If you need a set routine for family or other commitments, primary care may be a better fit. If you can tolerate shift variability and higher-intensity blocks, acute care might be acceptable.
- State practice environment: In reduced-practice or restricted-practice states, primary care NPs may face more collaborative agreement requirements that affect autonomy and job availability. Acute care NPs typically work in hospital systems where physician collaboration is built into the model, making scope-of-practice laws less of a daily barrier. Research your state's nurse practice act and talk to local NPs.
Consider Long-Term Career Trajectories
Both tracks offer advancement paths that can shape your earnings and professional identity. Acute care NPs can pursue critical care fellowships, surgical first-assist roles, or hospital administration. Primary care NPs often move into community health leadership, practice ownership, or academic faculty positions. Sub-specialization, such as cardiology for acute care or endocrinology for primary care, can further refine your path. Exploring the full range of nurse practitioner specialties can help you identify which sub-specialty aligns best with your interests.
- Acute care growth: Hospital-based roles may lead to director of advanced practice or clinical nurse leader positions.
- Primary care growth: Outpatient roles can lead to population health management, telehealth program development, or independent practice ownership where permitted.
Let Your RN Experience Guide You
The unit where you currently work is a strong signal of which track will feel natural and where your clinical hours will be most relevant. If you've spent years in an ICU, ED, or step-down unit, an acute care NP program will build directly on that foundation. If your background is in ambulatory care, community health, or labor and delivery, primary care programs, like Family NP or Adult-Gerontology Primary Care NP, will map more closely to your expertise. Admissions committees also value this alignment, and you'll likely find the coursework and clinical rotations more intuitive.
Next Step: Compare Programs and Talk to NPs
Before committing, compare accredited online programs for each track, focusing on clinical placement support and specialty certification pass rates. Reach out to NPs currently working in acute care and primary care settings and ask about their typical week, frustrations, and what they wish they had known. If possible, arrange a shadowing day in the opposite setting to test your assumptions. A few hours observing can reveal whether the environment truly matches your expectations.
Frequently Asked Questions About Acute Care Vs. Primary Care NP
Choosing between acute care and primary care is one of the most important decisions in your NP education. Below are answers to the questions working nurses ask most often when weighing these two tracks.
- Can an acute care NP work in primary care?
- Generally, no. Certification bodies such as ANCC and AACN define your scope of practice by population focus. An acute care NP is certified to manage complex, unstable, or critically ill patients, not to deliver routine wellness or preventive care in an outpatient office. Working outside your certification scope creates legal and liability risks. Some states may have limited exceptions, but employers typically require certification that matches the care setting.
- What is the difference between an acute care NP and a family nurse practitioner?
- The core difference is patient population and care setting. A family nurse practitioner (FNP) provides primary, preventive, and chronic disease management across the lifespan in outpatient clinics and community health centers. An acute care NP focuses on episodic, complex, or critical illness in hospitals, ICUs, and specialty units. Their curricula differ accordingly: acute care programs emphasize advanced pathophysiology of acute illness, while FNP programs center on health promotion and longitudinal care.
- What is the salary difference between acute care and primary care nurse practitioners?
- Salaries overlap significantly, but acute care NPs often earn somewhat more due to hospital shift differentials, specialty complexity, and critical care premiums. The Bureau of Labor Statistics reports median NP pay above $126,000 nationally as of 2025. Acute care NPs in surgical subspecialties or ICU settings may exceed that figure, while primary care NPs in rural or community health roles may earn slightly less. Geography, experience, and employer type all influence the gap.
- What certifications do you need for acute care vs. primary care NP?
- For acute care, you would pursue the Adult Gerontology Acute Care NP (AGACNP) certification through ANCC or AACN. Pediatric acute care NPs earn the CPNP-AC credential. For primary care, common certifications include the Family NP (FNP-BC) through ANCC or AANP, or the Adult Gerontology Primary Care NP (AGPCNP-BC). Your graduate program must align with the certification exam you plan to sit for, so choose your track before enrolling.
- Can you switch from primary care NP to acute care NP?
- Yes, but it requires additional education. You would need to complete a post-master's certificate program in an acute care specialty, including new didactic coursework and clinical hours in acute or critical care settings. After finishing the program, you sit for the corresponding acute care certification exam. The reverse path, from acute care to primary care, follows the same process. Expect a post-master's certificate to take roughly one to two years part time.
- Is an acute care NP the same as an emergency room NP?
- Not exactly. Emergency departments employ both acute care and family NPs depending on the patient population and state regulations. An acute care NP is well suited for high-acuity ED patients because of training in managing unstable conditions. However, some EDs also hire FNPs to handle lower-acuity visits. The "emergency NP" is not a separate certification. Your eligibility depends on your existing certification and the employer's scope requirements.
- Do acute care NPs work longer hours than primary care NPs?
- Schedules differ more by setting than by specialty label. Acute care NPs in hospitals often work 12-hour shifts, nights, weekends, and holidays, which can mean fewer total workdays per week but less predictable hours. Primary care NPs typically follow a Monday through Friday, 8- to 10-hour day schedule with more regularity. Both roles average around 40 hours per week, though overtime and on-call expectations vary by employer and patient volume.