Most important takeaways…
- Most primary care pediatric NPs see 18 to 25 patients per day across well-child and acute visits.
- Documentation and care coordination consume nearly half the workday, rivaling time spent with patients.
- Many pediatric NPs work predictable weekday schedules with no overnight shifts, supporting strong work-life balance.
- NP employment is projected to grow 46 percent from 2023 to 2033, far outpacing most other occupations.
What does a pediatric nurse practitioner actually do between 8 a.m. and 5 p.m.? No two days are identical, but a clear rhythm emerges: a morning packed with well-child visits and developmental screenings, an afternoon of sick calls and parent counseling, and the invisible hours of charting that stretch past the last patient.
This article focuses on the primary care clinic setting, the most common workplace for pediatric NPs, with other environments like urgent care, school-based clinics, and telehealth covered in a later section. The daily reality involves balancing 18 to 25 patient encounters against a documentation burden that can rival direct care time, all while maintaining the kind of predictable schedule that draws many nurses to the specialty in the first place. If you are exploring this career path, browsing accredited online pediatric nurse practitioner programs is a practical way to start mapping out the education required.
A Typical Pediatric NP Schedule, Hour by Hour
The real tension in a pediatric NP's day is not the patient load itself. It is everything that happens around the patients that most people never see coming. Here is what a realistic Monday looks like at an outpatient pediatric primary care clinic.
Before the First Patient Arrives
Most primary care pediatric NPs arrive between 7:30 and 8:00 AM, a full thirty minutes before the schedule officially kicks off.1 That window is not free time. It is when you pull up the day's appointment list, flag the complex cases that will need extra attention, review any lab results that came back overnight, and work through the patient portal messages that accumulated since Friday afternoon. Parents send a lot of messages over the weekend, and clearing that queue before clinic starts keeps the day from unraveling by 9 AM.
Many clinics build a short morning huddle into this block as well. You and your two medical assistants or nurses briefly run through the schedule together, confirm which rooms are stocked, and surface anything unusual before the first family walks through the door.2
The Morning Block: Well-Child Visits and Physicals
Patient visits typically begin between 8:00 and 8:30 AM.3 Mornings tend to fill with well-child checks and annual physicals, which run roughly 20 to 25 minutes each.3 These are the thorough appointments: developmental screening, immunizations, growth chart review, anticipatory guidance for parents. They take focus, and scheduling them early, when you and the family are both fresh, is a pattern many clinics follow deliberately.
Sprinkled into the morning you will also find two or three medication follow-up visits, often for kids managing ADHD or asthma, running about 10 to 15 minutes each.3
Midday Catch-Up and the Afternoon Shift
Lunch runs from roughly noon to 1:00 PM, but calling it a full break oversells it.2 Charting that did not get finished between morning appointments tends to spill into this hour. The goal is to surface from lunch with a clean note queue before the afternoon block begins.
Afternoon slots fill differently than mornings. Acute sick visits (runny noses, ear pain, rashes, fevers) are shorter at 10 to 15 minutes each, and same-day add-ons are common.3 Families call in the morning and need to be seen by 3 PM. That schedule compression is real, and experienced pediatric NPs learn to anticipate it rather than be surprised by it.
The afternoon patient block closes around 4:30 PM, leaving 30 to 60 minutes for end-of-day administrative work: finalizing charts, sending referral orders, returning phone calls, and signing off on any documentation that requires a second look.3
Wrapping Up
Most primary care pediatric NPs are out the door between 4:30 and 5:30 PM on a standard clinic day.3 Full-time roles average 40 hours per week, typically spread across four or five clinical days. Some practices offer a half-day dedicated to documentation or administrative tasks each week, which meaningfully reduces the after-hours charting that can otherwise eat into personal time. Part-time arrangements, often one or two clinic days per week, are also available for NPs who need additional flexibility. Shared call schedules mean on-call nights rotate among colleagues, which is covered in more detail in the work-life balance section ahead. If you are considering this career path, exploring online PNP programs is a practical first step toward building the clinical foundation this role demands.
How Many Patients Does a Pediatric NP See per Day?
Nurse practitioners nationwide provided an estimated 1 billion patient visits in 2025-2026, reflecting the growing role of NPs in primary care.1 For pediatric nurse practitioners in a typical primary care setting, daily patient volume usually falls between 18 and 25 patients. This range aligns with national NP workforce data and practice management benchmarks, though actual numbers vary by clinic type, staffing, and patient complexity.2
What Shapes Daily Patient Volume?
Several factors push that number up or down. A practice with a dedicated medical assistant who rooms patients and documents vitals can shave minutes off each visit, allowing an NP to see two or three more children per day. EMR efficiency matters, too: a streamlined system cuts charting time, while a clunky one can make a 15-minute visit feel like 30. Payer mix and practice size also play a role. Smaller, independent clinics may schedule longer blocks to accommodate more detailed conversations with families, while larger, high-volume practices often optimize for throughput.
Blending telehealth visits into the day can further shift volume. A morning of in-person sick visits followed by a telehealth block for follow-ups or minor concerns keeps the schedule tight but manageable. When telehealth is woven in thoughtfully, many PNPs report a smoother flow without sacrificing total patient count. The right nurse practitioner tools can make a real difference in streamlining these workflows.
Visit Types and Scheduling Blocks
The mix of visits directly dictates how many patients an NP can see. A standard sick visit (ear infection, rash, fever) is often slotted at 15 minutes, while a well-child check or a new-patient visit may need 20 to 30 minutes. When a schedule stacks mostly acute complaints, volume sits near the high end of the range; when it is heavy with well-child exams or new patients, the count drops.
Complex behavioral health screenings, such as an initial ADHD evaluation, can extend to 30 or 45 minutes. Even one of these can pull a day's total from 24 down to 18 patients. Many PNPs build in catch-up time or block these longer visits at the end of a session to protect the rest of the day.
Comparing Settings: Primary Care vs. Urgent Care
In pediatric urgent care, the pace quickens. PNPs in these settings often see 25 to 35 patients a day, with visits compressed to 10-15 minutes focused on a single, acute problem. There is less anticipatory guidance, no lengthy developmental screenings, and a team that handles much of the paperwork. Understanding the difference between acute care vs primary care is essential for a PNP considering a career move: primary care offers deeper relationships and more variety, while urgent care rewards speed and triage skills with higher volume but less continuity.
What the Data Tells Us
While national surveys like the AANP's ongoing Practice Survey track the profession's broad footprint, granular pediatric-specific volume figures are harder to pin down.1 The ranges shared here (18 to 25 for primary care, 25 to 35 for urgent care) come from a synthesis of published practice reports, discussions with practicing PNPs, and large-scale workforce analyses.2 They are not one-size-fits-all guarantees but offer a realistic window into what a typical day holds. As EMRs evolve and team-based care expands, these numbers may shift, but they remain a solid starting point for anyone shadowing, job hunting, or simply curious about the pulse of a pediatric NP's day.
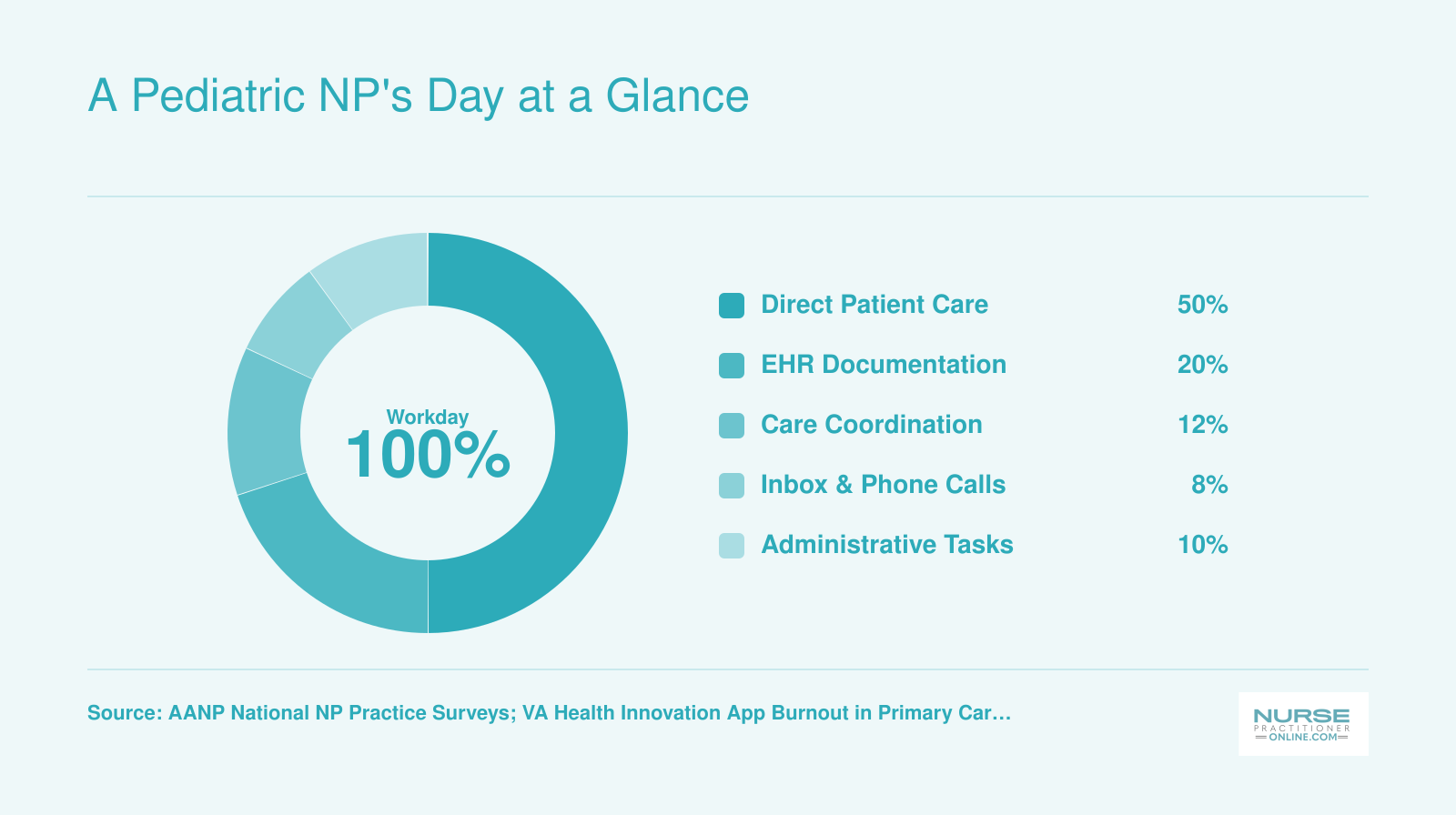
A Pediatric NP's Day at a Glance
How do primary care pediatric nurse practitioners actually divide their workday? While exact percentages vary by practice setting, national surveys and time-allocation studies consistently show that direct patient encounters account for roughly half the day, with the rest split among documentation, care coordination, and administrative responsibilities. About 13% of primary care advanced practice providers report spending overtime hours on electronic health record tasks alone.
Direct Patient Care Vs. Indirect Work: Where the Time Really Goes
The documentation burden in pediatric primary care has grown so substantial that many nurse practitioners now spend nearly as much time on electronic health records as they do with patients in the exam room. This reality represents the part of the job description that recruitment materials rarely advertise, yet it shapes every workday.
The Hidden Weight of EHR Documentation
Research examining primary care workflows reveals a striking imbalance: for every 30-minute patient visit, clinicians spend an average of 36.2 minutes on EHR-related tasks.1 That total includes 7.8 minutes managing inbox messages and 6.2 minutes of what the field calls "pajama time," the charting that happens after clinic doors close, often from a couch at home.
Across primary care settings, studies show clinicians devote roughly 66.7% of their workday to indirect care activities, while direct face-to-face patient contact accounts for just 12.5% of total work hours.2 For nurse practitioners and physician assistants specifically, daily EHR time averages 176.5 minutes, nearly three hours spent clicking, typing, and navigating digital systems.2
What Indirect Work Actually Includes
The tasks that pile up beyond exam room encounters touch every stage of patient care:
- Chart prep before visits: Reviewing growth trends, immunization status, recent specialist notes, and outstanding lab results before the family arrives
- After-visit summaries: Writing clear instructions that parents can reference at home, especially for complex diagnoses or new medications
- Prescription refills: Processing requests for maintenance medications, ADHD stimulants, and asthma inhalers between scheduled appointments
- Prior authorizations: Spending 15 to 30 minutes justifying medical necessity for specialty referrals, imaging, or certain prescriptions that insurers flag
- Parent portal messages: Answering questions about fevers, rashes, behavioral concerns, and whether symptoms warrant an urgent visit
- Referral letters: Composing detailed summaries for subspecialists, developmental pediatricians, or mental health providers
- School and camp paperwork: Completing physical forms, medication administration orders, allergy action plans, and 504 accommodation documentation
The Growth of After-Hours Charting
Recent data from Virginia primary care settings found that 35.5% of advanced practice providers report substantial after-hours EHR time as a contributor to burnout.3 As patient portal adoption has increased, inbox time per visit has risen by approximately 29%, and after-hours charting per visit has climbed by roughly 40%.4 The convenience patients gain through digital messaging has translated directly into additional evening work for clinicians.
Strategies for Managing the Load
Pediatric NPs have developed practical approaches to protect their time and reduce documentation spillover into personal hours:
- Medical scribes: Some practices employ scribes who document the visit in real time, freeing the NP to focus entirely on the child and family
- Voice-to-text dictation: Dragon, Nuance, and similar tools allow clinicians to narrate notes rather than type, cutting documentation time by 30% or more
- Dot-phrase templates: Pre-built text blocks for common scenarios (normal well-child exams, standard anticipatory guidance, routine vaccine conversations) reduce repetitive typing
- Batched inbox time: Rather than responding to messages throughout the day, many PNPs set two daily windows, typically mid-morning and late afternoon, to process portal messages and refill requests in focused bursts
Understanding this balance between direct care and administrative work helps prospective pediatric NPs set realistic expectations. The exam room moments remain rewarding, but the work surrounding those encounters requires deliberate systems to keep it from consuming evenings and weekends. If you are weighing a career move into advanced practice, exploring how to enroll in NP school online can help you plan the transition without stepping away from your current role.
Work-Life Balance, On-Call Duties, and Schedule Flexibility
One of the most appealing benefits of being a pediatric nurse practitioner in primary care is the predictable, family-friendly schedule. Many PNPs work standard 4x10 or 5x8 shifts Monday through Friday, with no weekend rotations and no overnight shifts. This structure represents a major lifestyle upgrade for RNs transitioning from hospital floors, where 12-hour shifts, night rotations, and weekend coverage are the norm. Pediatric nurse practitioner work-life balance is often cited as a top reason experienced nurses pursue the role, particularly those with growing families of their own.
On-Call Responsibilities in Primary Care
Most outpatient pediatric practices share a phone-triage rotation to field after-hours questions from anxious parents. You might be on call one evening per week and one weekend every four to six weeks, depending on the size of your practice group. On-call typically means staying accessible by phone to answer questions about fevers, rashes, medication dosing, or whether a child needs to be seen in the emergency room. Physical visits are rare. You will not usually need to go into the clinic unless a true emergency arises, and even then, you would direct families to the nearest urgent care or ED rather than reopening the office. Contrast this with inpatient pediatric NPs or those in urgent care settings, who may work rotating weekends, evening shifts, or even 24-hour on-call blocks that require in-person response.
Beyond the Schedule
The benefits extend well past clock-out time. Primary care pediatric NPs enjoy significant clinical autonomy, ordering tests, diagnosing conditions, and managing treatment plans independently (within collaborative practice agreements where required). You build long-term relationships with patients and families, watching infants grow into teenagers and partnering with parents through every developmental milestone. There are no overnight shifts in most outpatient settings, meaning you sleep in your own bed every night and can plan family dinners, school events, and weekend trips with confidence.
Seasonal Trade-Offs
Honesty requires acknowledging the downsides. Pediatric primary care has pronounced seasonal surges. August brings a flood of back-to-school physicals, sports clearances, and immunization catch-ups. December through February is peak respiratory illness season, with daily patient counts climbing well above the usual 15 to 20. During these windows, you may see 25 or more patients a day, squeeze in urgent same-day visits between scheduled slots, and stay late charting. Burnout risk spikes when high volume persists for weeks. Many practices try to mitigate this by blocking extra appointment slots in advance, bringing on temporary staff, or offering telehealth overflow, but the reality is that flu season and physical season are intense. Planning vacation around these peaks and building recovery time into your calendar becomes essential for sustaining a career in pediatric primary care.
Questions to Ask Yourself
Is Being a Pediatric Nurse Practitioner Stressful?
Yes, being a pediatric nurse practitioner can be stressful, but the sources of that stress often surprise new clinicians. The pressures that weigh most heavily are rarely the clinical decisions themselves. Instead, they tend to cluster around documentation demands, productivity expectations, and the emotional complexity of caring for vulnerable children and their families.
Understanding the Burnout Landscape
Research consistently places primary care nurse practitioners in a high-risk category for burnout, with rates ranging from 30 to 50 percent across national surveys.1 A 2026 analysis of advanced practice providers in Virginia found burnout rates between 33 and 50 percent in primary care settings.2 Pediatric NPs experience emotional exhaustion levels comparable to or slightly higher than their colleagues in adult primary care, though they tend to report somewhat lower depersonalization, likely because the nature of pediatric relationships keeps them more emotionally engaged with patients.2
Despite these challenges, the picture is not entirely bleak. More than 70 percent of primary care nurse practitioners report high career satisfaction.3 That paradox, where clinicians simultaneously experience stress yet find their work deeply meaningful, reflects the unique protective factors built into pediatric practice: long-term patient relationships, the satisfaction of watching children grow, and the autonomy to shape care decisions.
The Top Stressors Pediatric NPs Face
The stressors that pediatric NPs identify most consistently include:2
- Workload and EHR burden: Documentation requirements eat into face-to-face time with patients and extend the workday into evenings and weekends.
- Productivity pressure: Many employers set visit volume targets that can feel at odds with providing thoughtful pediatric care.
- Emotional weight: Cases involving suspected abuse, new chronic illness diagnoses, or behavioral health crises take a toll that accumulates over time.
- Family dynamics: Parents bring their own anxieties, expectations, and sometimes frustrations into the exam room, adding a layer of emotional labor.
- Scope-of-practice limitations: State laws vary widely, and restrictions on prescriptive authority or practice independence create friction in some settings.
- Compensation: Pediatric NPs often earn at the lower end of NP compensation scales, which can compound feelings of being undervalued.4
Strategies That Actually Help
Experienced pediatric NPs have developed practical approaches to managing stress that go beyond generic self-care advice:
- Peer support groups: Regular debriefs with colleagues who understand the specific challenges of pediatric practice provide both emotional support and practical problem-solving.
- Bounded charting windows: Setting firm limits on after-hours documentation, such as completing notes within 30 minutes of the last patient rather than late at night, protects personal time.
- Collaborative relationships: Using the collaborating physician as a sounding board for difficult cases distributes the emotional and clinical burden.
- Scheduled decompression: Building in brief recovery time after heavy cases, even a ten-minute walk or coffee break, prevents emotional spillover into the next patient encounter.
Why Many PNPs Stay Despite the Stress
The factors that protect against burnout mirror what draws clinicians to pediatric practice in the first place. Supportive leadership, reasonable patient panel sizes, adequate staffing, and opportunities for professional growth all correlate with lower burnout and higher retention. For PNPs considering additional credentials to expand their options, post-master's pediatric nurse practitioner certificate programs can open new pathways without requiring a full degree. When these elements are present, the autonomy and meaningful relationships that define pediatric NP work serve as powerful counterweights to the daily pressures. Most pediatric NPs, even those who acknowledge significant stress, describe their career choice as deeply rewarding.
How the Day Differs by Setting: Clinic, Urgent Care, School-Based, and Telehealth
A pediatric nurse practitioner's daily life is far from one-size-fits-all. Your schedule, patient volume, and core tasks transform across clinic, urgent care, school-based, and telehealth settings.
Primary Care Clinic
In a traditional primary care clinic, a pediatric NP sees 18 to 26 patients each day through scheduled visits.1 The mix includes well-child checkups, immunizations, acute sick visits, and follow-ups for chronic or behavioral conditions. The schedule is predictable: Monday through Friday, roughly 8:00 AM to 5:00 PM, with seasonal ebb and flow (for example, more respiratory illnesses in winter). Team-based care with medical assistants and registered nurses is the norm, and a significant portion of the day goes to in-basket tasks like reviewing labs, responding to parent messages, and documenting developmental screenings. After-hours call responsibilities may also rotate among providers.
Pediatric Urgent Care
Urgent care flips the script: patient volumes climb to 25 to 40 or more per shift, and the pace is driven by walk-in demand during extended hours.2 Evenings, weekends, and holidays are peak times. Visits center on acute complaints such as high fevers, wheezing, lacerations, sprains, and rashes. There are no well-child exams here. Workflow is protocol-driven and high-throughput, with on-site diagnostics like rapid strep or x-ray guiding quick decisions on whether to treat, refer to the emergency department, or send home. While continuity is minimal, the NP often communicates findings back to the child's primary care provider.
School-Based Health Center
A school-based health center operates on a school-day schedule, typically 7:30 AM to 3:30 PM.3 A pediatric NP here manages 10 to 20 students per day with a blend of scheduled appointments for chronic disease management (asthma, ADHD, mental health) and walk-in visits for acute issues like headaches, stomachaches, or minor injuries. The role uniquely bridges healthcare and education: NPs coordinate closely with teachers, school nurses, and counselors, obtain consents, and monitor public health trends such as immunization compliance or infectious outbreaks. A strong focus on social determinants of health is embedded in daily practice.
Telehealth
Virtual care has become a distinct daily rhythm, with NPs handling 20 to 30 or more encounters during a shift that may include evenings or weekends.4 Visits are often low-acuity, covering pink eye, rashes, upper respiratory infections, behavioral health check-ins, and medication follow-ups. The NP must excel at virtual triage, deciding who can be managed remotely versus who needs an in-person visit or emergency care. The physical exam relies on parent assistance and home devices, and documentation and messaging loads can be high. Many telehealth roles require navigating multistate licensure and integrating on-demand visits between scheduled blocks.
Related Articles
Pediatric NP Salary and Job Outlook
The nurse practitioner field as a whole is among the fastest-growing occupations tracked by the federal government, which is worth keeping in mind as you weigh the return on an advanced degree.
What the Data Actually Says
The Bureau of Labor Statistics (BLS) Occupational Outlook Handbook covers nurse practitioners under SOC code 29-1171. As of the most recent projections, the BLS forecasts employment growth in this category well above the average for all occupations through the early 2030s. The exact growth rate and salary figures are updated periodically, so the most reliable approach is to visit the BLS Occupational Outlook Handbook directly and look up nurse practitioners to pull the current numbers. The same page carries median annual wage data broken down by industry and, in some editions, by state.
For pediatric-specific demand and specialty salary benchmarks, the American Association of Nurse Practitioners (AANP) publishes workforce and salary reports that go deeper than the broad BLS category. These reports often capture trends in primary care focus areas, including pediatrics, and can give you a clearer picture of where hiring activity is concentrated.
Why Pediatric Primary Care Demand Runs High
A few structural forces push demand for pediatric NPs beyond what the general NP growth rate might suggest on its own. Pediatrician shortages in rural and underserved communities have been documented for years, and many health systems have responded by expanding NP roles to cover primary care panels. You can read more about nurse practitioner shortage trends across the country for added context. Medicaid expansion in states that adopted it has brought more children into covered care, increasing visit volume without a corresponding increase in physician supply. Together, these pressures create consistent hiring demand, particularly in community health centers, federally qualified health centers, and school-based health programs.
Checking Regional Variation
National figures tell only part of the story. State-level nursing workforce reports, published by state boards of nursing or state health departments, can reveal meaningful differences in NP supply and demand by region. If you are deciding where to practice or whether to relocate, those reports are worth tracking down alongside any data your prospective graduate program provides.
Getting the Most Current Picture
Graduate programs that offer pediatric NP tracks often collect placement statistics and maintain relationships with clinical hiring partners. Exploring accredited online pediatric nurse practitioner programs is a practical way to compare placement data and connect with admissions or program faculty about current hiring demand. Pair that with the BLS handbook and AANP workforce data, and you will have a reasonably complete picture before making any program or career decision.
Nurse practitioner employment is projected to grow 46 percent from 2023 to 2033, according to the Bureau of Labor Statistics. This rate far outpaces average occupational growth, making the NP profession one of the fastest expanding careers in healthcare and signaling strong long term demand for pediatric primary care providers.
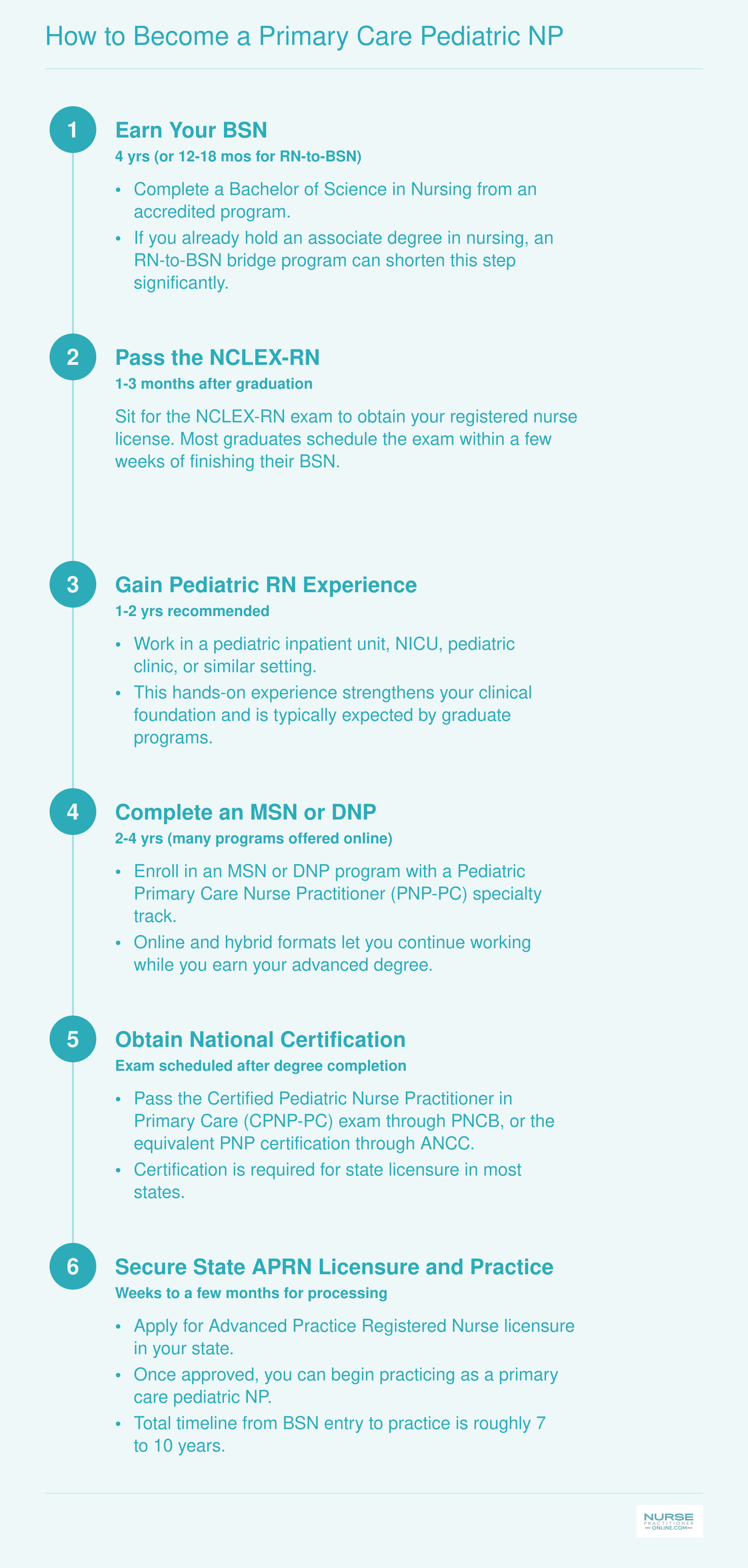
How to Become a Primary Care Pediatric NP
The road from bedside nurse to practicing primary care pediatric nurse practitioner follows a clear credentialing ladder. Here is each stage with realistic timelines so you can map out your own plan.
Frequently Asked Questions About Pediatric NP Daily Life
Below are answers to some of the most common questions working nurses ask when considering a career as a primary care pediatric nurse practitioner. Each response draws on the topics covered throughout this guide.
- What is a typical day for a pediatric NP?
- A typical day begins with a morning huddle and chart review, followed by a steady flow of well-child visits, sick appointments, and developmental screenings. Afternoons often include follow-up calls, care coordination with specialists, and documentation. Most primary care pediatric NPs work roughly 8 to 10 hours per weekday, though the exact pace depends on the practice setting.
- Is being a pediatric nurse practitioner stressful?
- Like any healthcare role, pediatric NP work involves emotional and logistical pressures, from managing anxious parents to keeping up with documentation. However, many practitioners report that the strong relationships they build with families and the variety of daily tasks offset the stress. Supportive colleagues, reasonable patient loads, and flexible scheduling options also help maintain well-being over the long term.
- How many patients does a pediatric nurse practitioner see per day?
- Most primary care pediatric NPs see between 18 and 25 patients per day, although the number varies by setting. Outpatient clinics with shorter well-child visits may push the count higher, while urgent care or complex care settings often mean fewer patients with longer encounter times. Telehealth days can also shift the volume depending on visit type.
- What are the benefits of being a pediatric nurse practitioner?
- Key benefits include meaningful long-term relationships with young patients and their families, strong earning potential, and a favorable job outlook. Pediatric NPs also enjoy variety in their daily work, a high degree of clinical autonomy in most states, and schedule flexibility that supports a healthy work-life balance, especially in outpatient settings.
- Where do pediatric nurse practitioners work?
- Pediatric NPs practice in a wide range of environments, including private pediatric offices, hospital-based outpatient clinics, federally qualified health centers, school-based health programs, and urgent care facilities. A growing number also deliver care through telehealth platforms, expanding access for families in rural or underserved communities.
- What is the difference between a pediatric NP and a family NP?
- A pediatric NP (PNP) is certified to care for patients from birth through young adulthood, typically up to age 21. A family NP (FNP) is trained across the entire lifespan. PNPs receive deeper, more focused education in childhood development, pediatric pharmacology, and age-specific conditions, making them especially well suited for dedicated pediatric practices.
- Do pediatric NPs work weekends?
- In most primary care outpatient settings, pediatric NPs work Monday through Friday with occasional Saturday morning hours. Urgent care and hospital-based roles are more likely to include weekend shifts. Some practices rotate weekend coverage among providers, giving each clinician regular weekends off while still meeting patient demand.
- What EMR systems do pediatric NPs use most?
- Epic and eClinicalWorks are among the most widely used electronic medical record platforms in pediatric primary care. Other common systems include Athenahealth and Office Practicum, which is designed specifically for pediatric practices. Familiarity with at least one major EMR is expected, and most employers provide training during onboarding.