Most important takeaways…
- Marcy Markes challenges Missouri's $50,000 annual CPA fee in court.
- Missouri NPs face $10,000 fines per patient without a CPA.
- Thirty-five states do not restrict nurse practitioner practice with CPAs.
In Missouri, a nurse practitioner with over 30 years of experience pays $50,000 a year for a signature. Marcy Markes runs an allergy and asthma clinic in Columbia but cannot order lab tests or write prescriptions without a collaborative practice agreement (CPA) with a physician. Her lawsuit challenging that requirement could reshape NP clinical rotations and placement costs nationwide.
For NP students, the case strikes at the heart of a broken system: if practicing NPs are forced to pay exorbitant fees just to work, the financial strain trickles down to students who already pay preceptor placement fees and face limited clinical sites. A ruling in Markes's favor would not only end her annual payment but also weaken the legal foundation for other costly collaboration mandates, potentially freeing students and working NPs to focus on patient care instead of paperwork.
What the Missouri NP Lawsuit Is About
For many nurse practitioners, the path to providing care splits into two distinct directions. In most states, NPs can practice independently, evaluating patients, prescribing medications, and ordering tests without physician oversight. In Missouri and a handful of other states, however, NPs remain legally tethered to a physician through a collaborative practice agreement that comes with a hefty price tag and strict limitations. The lawsuit filed by Marcy Markes challenges this system head-on, arguing that the CPA requirement is not only costly but unconstitutional.
The CPA Requirement in Missouri
Missouri law requires nurse practitioners to hold a signed collaborative practice agreement with a physician in order to perform tasks central to patient care, including ordering routine lab tests and writing prescriptions. Physicians can charge any fee they wish for these agreements, and they are also limited in the total number of CPAs they can hold. This creates a seller's market in which NPs have little leverage, particularly in underserved areas where physicians are scarce.
Markes, who holds degrees from the University of Missouri and has over 30 years of experience in intensive care and small-town clinics, now runs an allergy and asthma clinic in Columbia. Under her current arrangement, she pays between $50,000 and $52,800 annually for the signature that keeps her practice legal.1 According to the Pacific Legal Foundation, which represents her, the collaboration consists primarily of a retrospective chart review rather than any day-to-day supervision or clinical guidance.2
The Cost and Consequences for NPs
The financial burden is just one part of the equation. Practicing without a valid CPA carries severe penalties: license revocation, a fine of up to $10,000 per patient, and a felony charge that could lead to up to seven years in prison.3 These consequences effectively lock NPs into whatever terms physicians set. For Markes, the cost amounts to a substantial portion of her practice's revenue, yet she cannot legally provide allergy and asthma care without the agreement.
Challenging the Status Quo
Markes's case, Marcy Markes v. Andrew Bailey et al., was filed in Missouri Circuit Court in August 2025 and remains active as of mid-2026. The lawsuit argues that the CPA requirement violates the Missouri Constitution's protection of the "gains of their own industry" by forcing NPs to pay physicians for permission to work.3 It highlights that roughly 80% of Missouri is considered a physician desert, where limited access to primary care makes it even more critical for NPs to practice to the full extent of their training.
The case has drawn national attention, including a Washington Post op-ed published in June 2026, because it reflects a broader shift in nurse practitioner practice authority across the country. Today, 35 states have moved to independent practice, eliminating CPA requirements.4 Missouri is one of just 12 states that still mandate full collaborative agreements. If the court sides with Markes, it could not only erase a significant financial barrier for NPs in Missouri but also set a precedent for similar challenges in the remaining states with restrictive CPA laws.
How Collaborative Practice Agreements Drive up NP Costs
Collaborative practice agreements create an uncapped, unregulated marketplace where physicians can charge nurse practitioners whatever they wish for a required signature, funneling tens of thousands of dollars away from patient care every year.
An uncapped seller's market for physician signatures
In states like Missouri, a CPA is a legal contract that gives a physician oversight of an NP's prescribing and diagnostic authority. Physicians set the fee, and there is no legal ceiling. Marcy Markes pays $50,000 annually to maintain hers, but she is not an outlier. NPs in restrictive states routinely report monthly CPA costs ranging from a few hundred to several thousand dollars. Because Missouri limits the total number of CPAs a single physician can hold, the pool of available collaborators shrinks, giving physicians even greater leverage to demand steep payments. The result is a classic seller's market where NPs must either pay whatever the market bears or abandon their practice.
From NP to student: the downstream squeeze
The financial strain of CPAs does not stop with working NPs. When seasoned clinicians are forced to divert large sums toward a collaborative agreement, they have fewer resources and less bandwidth to mentor the next generation. This contributes directly to the preceptor shortage that plagues NP education. In CPA-heavy states, students frequently encounter placement delays and, increasingly, requests to pay for preceptor time. Some third-party matching services now charge students hundreds or even thousands of dollars per clinical rotation. The chilling effect on practice formation also means fewer NP-owned clinics, which are often the most likely sites to train students. What begins as a fee on an experienced NP cascades into higher educational costs and longer time-to-degree for students.
Evidence of a barrier, not a safeguard
Defenders of CPAs argue the agreements protect patient safety, but the evidence does not support that claim. A 2018 study found that independent NP practice reduces travel times, improves scheduling convenience, and increases continuity of care. Patients see consistent providers and gain more timely access. Nurse practitioners as primary care providers face the CPA requirement as an added layer of administrative friction with no demonstrable quality gains. It is a regulatory hurdle that restricts care access while extracting revenue from NP professionals.
Rural America pays the price
The human impact is sharpest in rural areas. According to the University of Washington's Rural Health Research Center, in 2025 there were 1,761 NPs serving rural communities versus only 1,358 primary care physicians. Nurse practitioners in rural healthcare are already the backbone of primary care in these communities. Yet when a rural NP cannot afford a CPA, the clinic may close, eliminating the only local option for hundreds of patients. The fees that physicians charge for collaborative agreements effectively tax the very providers who are filling the nation's physician desert gaps, making it harder to recruit and retain NPs where they are needed most.
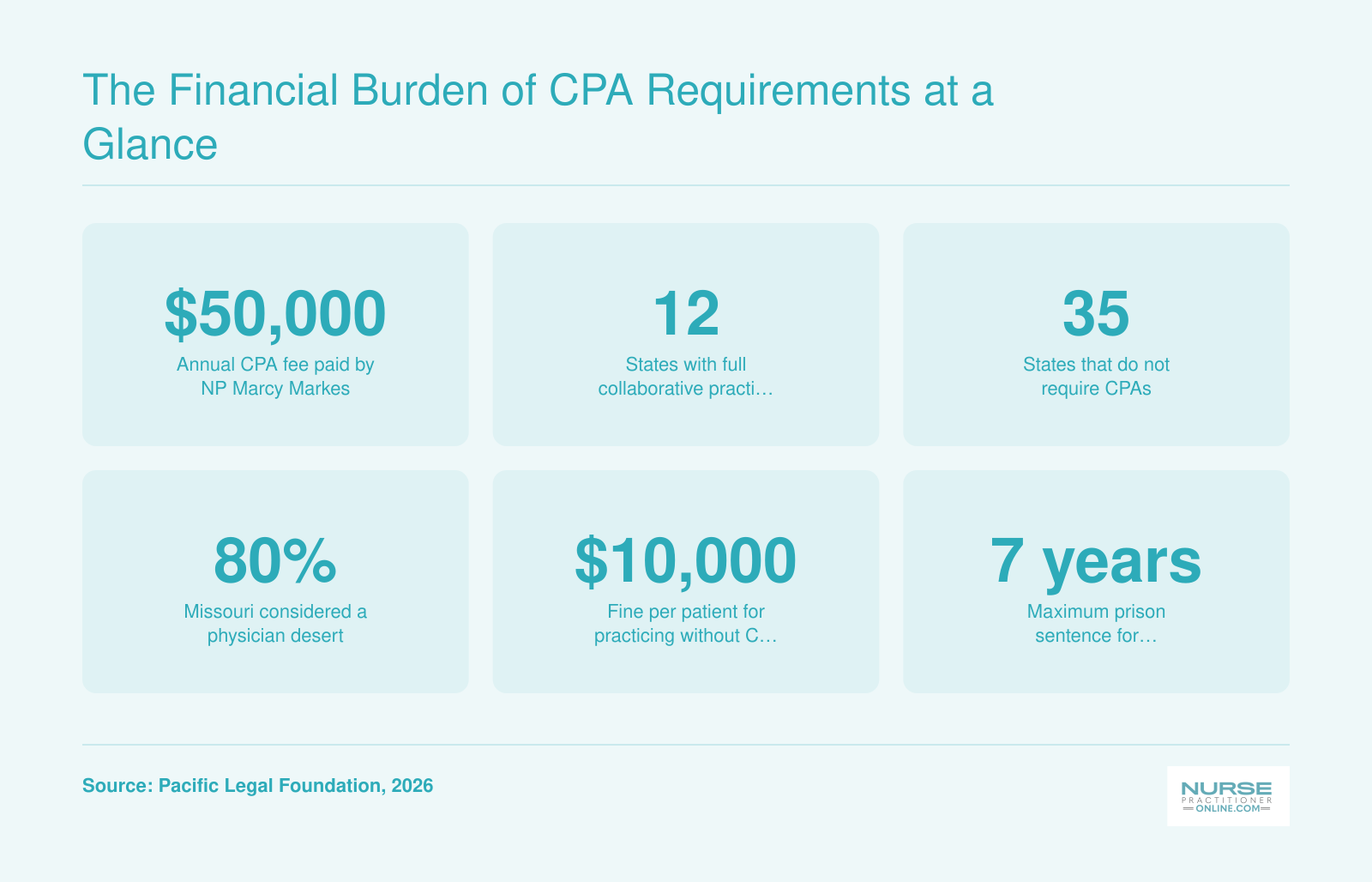
The Financial Burden of CPA Requirements at a Glance
The collaborative practice agreement (CPA) mandate in Missouri imposes heavy financial and legal burdens on nurse practitioners. Marcy Markes's $50,000 annual fee is just one example of how these restrictions drive up costs and limit practice autonomy.
Are NP Preceptor Fees Legal? A State-By-State Overview
Most nurse practitioner students and practicing NPs encounter two distinct kinds of fees tied to clinical collaboration: collaborative practice agreement (CPA) fees, which are paid by licensed NPs to supervising physicians in states that require CPAs, and preceptor placement fees, which are payments made by NP students, often through third-party matching services, to secure a clinical training site. While CPA fees are clearly permitted (and sometimes capped) under state law, preceptor fees exist in a murky regulatory gray area. Neither federal law nor most state boards of nursing explicitly prohibit or regulate a student's ability to pay for clinical placement.
State practice models directly influence preceptor access and costs
States with the most restrictive practice laws, those requiring full CPAs, tend to have the tightest preceptor markets. When physicians must supervise NPs, there is often a financial incentive for them to charge for that supervision, which can cascade down to students seeking clinical hours. In contrast, states that grant full practice authority to NPs typically have more clinical sites available without added fees, because practicing NPs can serve as preceptors without physician oversight. The table below summarizes the current landscape for a sample of states.2
| State | NP Practice Authority | CPA Required? | Preceptor Fee Regulation |
|---|---|---|---|
| Texas | Restricted | Yes | No explicit regulation |
| Florida | Restricted | Yes | No explicit regulation |
| North Carolina | Restricted | Yes | No explicit regulation |
| California | Reduced | Yes (with recent changes) | No explicit regulation |
| Arkansas | Reduced | Time-limited CPA | No explicit regulation |
| Virginia | Reduced | Time-limited CPA | No explicit regulation |
| New York | Full | No | No explicit regulation |
| Arizona | Full | No | No explicit regulation |
*Note: "Reduced" practice authority indicates states with some barriers to full practice, such as time-limited CPA requirements.*
What this means for NP students and working NPs
Because preceptor placement fees are largely unregulated, students in restrictive or reduced-practice states often face significant out-of-pocket costs, sometimes thousands of dollars per semester, just to complete required clinical hours.1 Meanwhile, NPs who pay CPA fees as part of their employment may find that those costs indirectly reduce the pool of willing preceptors, as physicians may prefer supervising NPs who already pay them. Understanding how NP preceptors get paid can help students negotiate arrangements more confidently and spot when fees cross into exploitation. As the Missouri case progresses, a ruling against CPA requirements could increase the number of available preceptors and potentially ease the financial burden on students nationwide. For now, NP students should check their state board of nursing's website for any guidance on preceptor payments and document all arrangements in writing.
Related Articles
What Accreditation Bodies and Professional Organizations Say About Preceptor Fees
The Markes lawsuit has brought long-simmering tensions over preceptor fees and collaborative practice mandates into sharp focus, yet the organizations that shape NP education and policy have offered few clear directives.
Where Accreditors Stand on Preceptor Fees
Accrediting bodies like the CCNE and ACEN set the standards for nursing programs, but their language on paid preceptors remains notably noncommittal. The CCNE's 2024 standards (effective January 1, 2025) emphasize that programs are responsible for ensuring "quality clinical learning arrangements" and that the preceptor role must be clearly defined and communicated1, yet they do not explicitly prohibit students from paying for their own preceptors. Similarly, ACEN's standards require programs to evaluate clinical site effectiveness but stop short of addressing the financial strain placed on students. For NP students, this silence translates into a patchwork reality: some schools arrange placements at no extra cost, while others leave students to secure and pay for their own preceptors, with fees sometimes reaching thousands of dollars per semester. Understanding nursing program accreditation standards is a helpful starting point for evaluating how your program handles clinical placement responsibility.
How Professional Associations Frame the CPA Debate
In contrast, professional organizations like the AANP and ANA have been vocal, not necessarily about preceptor fees directly, but about the broader regulatory environment that fuels them. Both organizations have long championed full practice authority, arguing that modern NP training makes collaborative practice agreements redundant. The AANP's policy compendium states that CPAs impose unnecessary administrative and financial burdens on providers without improving care quality. The Markes lawsuit echoes this stance: if Missouri's CPA requirement is struck down, the economic pressure to pay physicians for supervision, and by extension the pressure on students to pay for clinical access, could lessen significantly.
What Students Actually Need from These Bodies
For NP students caught in the preceptor fee dilemma, the current landscape is confusing. No accreditor explicitly bans student-paid preceptorships, leaving programs to set their own policies. Meanwhile, the AANP and ANA's advocacy focuses on post-licensure practice rather than the clinical training pipeline, even though the two are intimately linked. Nurse practitioner networking strategies can help fill the gap, giving students a practical path to finding preceptors outside of paid placement services. As the lawsuit unfolds, these positions and their gaps will shape whether preceptor fees become a relic or a lasting norm.
Your Legal Rights as an NP Student Paying Preceptor Fees
Understanding your legal protections is the first step to pushing back against potentially unfair preceptor fees.
Checking State Board Disciplinary Records
State boards of nursing maintain public records of disciplinary actions and complaints. Many boards post enforcement records online, making it possible to search for any previous sanctions against preceptor placement services. These records may include license revocations, fines, or other penalties. If you find relevant actions, that information can guide your decision to work with a particular service. Start with a simple search of the board's website, often under a "consumer protection" or "disciplinary actions" tab.
Searching the National Practitioner Data Bank
The National Practitioner Data Bank (NPDB) collects adverse action reports on healthcare practitioners and organizations. Although access typically requires a formal request, the database can reveal red flags such as fraud allegations or other misconduct by placement agencies. While not all NP students will need to query the NPDB, it is a resource worth considering if you encounter serious concerns. Your school's clinical coordinator may be able to help you navigate the process.
Reviewing School Policies and Contracts
Your school's clinical placement office should provide a list of approved preceptor agencies. Ask directly about how agencies are vetted and whether any complaints have been received. Many schools require students to use only pre-approved agencies, but the quality of oversight varies. If you need guidance on finding NP clinical preceptors independently, that process also reveals what reasonable placement looks like. Read contracts carefully for arbitration clauses that might restrict your ability to take disputes to court. If terms seem unclear, seek clarification from a student legal services office or an attorney familiar with education contracts.
Filing Complaints When Something Goes Wrong
If you suspect fraud, overcharging, or deceptive practices, file a complaint with your state attorney general's consumer protection office. Some states publish annual reports on deceptive business practices, which can also help you research a company's history. Additionally, report your experience to the nursing board and your school's administration. Beyond state avenues, consider the Federal Trade Commission if the issue involves interstate commerce. Keep detailed records of all communications and payments: organized documentation strengthens any complaint and helps protect your financial interests.
What Happens Next: Timeline and Potential Outcomes
Legal challenges to practice restrictions take two main paths: a swift settlement that changes policy quietly, or a protracted courtroom battle that sets binding precedent. For Missouri NP Marcy Markes, the latter is unfolding.
Expected Procedural Steps and Timeline
A constitutional challenge of this type typically begins with motions to dismiss by the state. If the court allows the case to proceed, the discovery phase follows, where both sides gather evidence on the financial and healthcare-access harms of Missouri's collaborative practice agreement (CPA) mandate. Expert depositions from health economists, physicians, and NPs will likely shape the record. A trial court ruling could arrive between 12 and 24 months after filing, though appeals are nearly certain from whichever side loses. A final resolution by a federal appellate court, or the U.S. Supreme Court if the constitutional question is novel, could take three to five years.
Impact on Other States: Binding or Persuasive Precedent?
A federal district court ruling striking down Missouri's CPA requirement would apply only within that district. For the 11 other states with full CPA mandates, the decision would serve as persuasive precedent, not binding law. However, a strong opinion grounded in economic liberty or equal protection could inspire copycat lawsuits elsewhere, especially in states with the most need for nurse practitioners where rural healthcare access mirrors Missouri's shortages. If a federal appellate court upholds such a ruling, its weight increases substantially, potentially emboldening NPs in multiple circuits to challenge similar restrictions.
What a Pro-NP Ruling Means for Students and Preceptor Access
If CPAs are struck down or reformed, the downstream effects on NP education could be significant. Easing practice restrictions often expands the pool of qualified preceptors willing to supervise students, since they no longer need to manage the legal and financial entanglement of a CPA. This could lower preceptor placement fees and reduce the financial strain on NP students, who currently pay thousands out-of-pocket for clinical placements. A more fluid pipeline from education to independent practice would strengthen the NP workforce, particularly in underserved rural and adult-gerontology care settings where demand is highest.
The Broader Workforce Pipeline
A ruling that removes CPAs would also increase the number of NPs who can open independent practices, especially in rural Missouri where primary care physicians are scarce. That expansion could create more clinical training sites for NP students, easing the bottleneck of preceptor availability that is often cited as a barrier to completing NP programs on time and within budget. Understanding advanced practice nursing trends helps put this evolving legal landscape in context for anyone planning their NP career.
Action Steps for NP Students and Working NPs
As a nurse practitioner student or working NP, taking proactive steps can protect your finances and support the push for fairer regulations. The following actions can help you navigate preceptor fees and collaborative practice agreements with confidence.
Vet Placement Services Thoroughly
Before paying, verify the service's reputation. - Check reviews: Search online for NP student experiences with the specific service. - Request written guarantees: Get commitments for placement timelines and refund policies in writing. - Confirm with your coordinator: Ensure the service meets your program's requirements and has a successful track record.
Know Your State's Regulatory Landscape
Rules for preceptor fees and collaborative practice agreements vary widely. Use AANP's state practice environment map to see whether your state requires CPAs, restricts paid preceptorships, or has pending legislation. In states like Missouri, full practice authority is not yet granted; staying informed helps you anticipate costs and legal risks before clinical rotations begin.
Engage in Advocacy for Lasting Change
Joining professional organizations amplifies your voice. AANP and state NP associations lobby for full practice authority and challenge laws like Missouri's CPA mandate. Understanding nurse practitioner organization perks can help you choose the memberships that offer the most leverage for advocacy and policy change. Tracking the Markes case outcome can inform your understanding of legal precedents. Even small actions, such as signing petitions or contacting legislators, contribute to reducing future financial barriers for NP students. For a structured approach, a nurse practitioner health policy toolkit can walk you through the most effective ways to engage with lawmakers.
Document All Contracts and Communications
Keep a paper trail of every placement contract, payment receipt, and email exchange with preceptor services. In the event of a dispute, this documentation can protect you legally. Screenshot online agreements and save voicemails if necessary. Organized records also help if you need to report unethical practices to your state board or seek a refund.
Frequently Asked Questions About NP Preceptor Fees and CPA Lawsuits
As NP preceptor fees and collaborative practice agreements face legal challenges, students and working NPs have pressing questions. Here are clear answers to the most common concerns, grounded in current law and recent developments.
- What is an NP preceptor honorarium?
- An honorarium is a payment made to a clinical preceptor for supervising an NP student's clinical hours. While some preceptors volunteer, many charge due to the time and liability involved. These fees vary widely and often fall on the student, adding to the financial burden of NP education.
- Are NP preceptor fees legal in every state?
- There is no federal ban on preceptor fees, and legality varies by state. Most states do not explicitly prohibit them, though some nursing boards discourage the practice. In states with restrictive laws like Missouri, demand for preceptors drives costs up, but paying for placements remains common across the U.S.
- Can a nurse practitioner be sued for practicing without a collaborative practice agreement?
- Yes. In Missouri and other states requiring collaborative practice agreements, practicing without one is illegal. Penalties can include license revocation, fines up to $10,000 per patient, and imprisonment up to seven years. This legal risk underscores the serious consequences of noncompliance.
- How much do NP students typically pay for preceptor placement services?
- Costs range from a few hundred to several thousand dollars per clinical rotation. Commercial placement services may charge $500, $2,000, or more per match. Over a program, these fees can total several thousand dollars, on top of tuition, making clinical training a significant financial challenge.
- Which states still require collaborative practice agreements for nurse practitioners?
- As of 2026, 12 states still require full collaborative practice agreements for NPs, including Missouri. The other states are typically concentrated in the Southeast and Midwest. This contrasts with 35 states allowing full independent practice, reflecting a national trend toward autonomy.
- What legal protections do NP students have when paying preceptor fees?
- Currently, few specific legal protections exist for students paying preceptor fees. The practice is largely unregulated, leaving students vulnerable to high costs or unscrupulous services. Professional organizations advocate for transparency, but until laws change, students must carefully vet agreements and explore financial aid options.