Most important takeaways…
- On June 10, 2026, the AMA House of Delegates voted to fund independent studies comparing NP-led and physician-led care models.
- The Florida delegation proposed the resolution, with Texas and Oklahoma co-sponsoring, to examine safety, quality, and cost.
- In full practice authority states, NP-led care increased primary care visits by 18% and reduced emergency department use and costs.
Will the AMA's June 2026 decision to fund its own NP-versus-physician outcomes research tilt the scope-of-practice debate against nurse practitioners? On June 10, 2026, the AMA House of Delegates voted to finance independent studies comparing patient outcomes between autonomous non-physician practitioners and physician-led care.
This move directly challenges the momentum toward NP independent practice, aiming to produce evidence that could influence reimbursement models and state legislation. While decades of existing research support the safety and quality of NP care, the framing and funding of these new studies place the profession in a defensive posture. For NPs, understanding the resolution's origins, the evolving role of nurse practitioners in modern healthcare, and the existing body of evidence is the first step in preparing an effective response.
What the AMA Voted to Do, and Why It Matters for NPs
The AMA's vote to fund its own outcomes comparisons sets up a classic tension: will these studies be an impartial look at care quality, or a strategic tool to narrow NP practice authority? The answer will shape legislative debates for years to come.
Inside the Resolution
On June 10, 2026, the AMA House of Delegates approved a measure to finance independent, academically rigorous studies that compare patient outcomes between autonomous non-physician practitioners , specifically nurse practitioners and physician assistants , and care models led by physicians (MD/DO or foreign equivalent). As reported by MedPage Today, the resolution calls for comparative effectiveness analyses across six domains: patient safety, care quality, utilization, access, cost, and health outcomes. The ultimate goal is publication in a peer-reviewed journal.
The push came from the Florida delegation, with co-sponsorship from Texas and Oklahoma. Luke Selby, MD, of Kansas noted the AMA's intent to solicit proposals from academic researchers and maintain strict editorial independence, signaling an effort to frame the research as objective.
Why NPs Should Pay Close Attention
For nurse practitioners, this is not a neutral academic exercise. Even if the studies are methodologically sound, their findings will be injected into full practice authority legislative battles at state and federal levels. The American Association of Nurse Practitioners (AANP) has pushed back, emphasizing that every major study over the last 50 years has found NP care to be safe, effective, and comparable to physician care.1 The NP Roundtable notes that NPs deliver more than one billion health care visits annually, and patient outcomes such as hospitalization rates, emergency department use, and satisfaction often equal or exceed physician-led care.2
The AMA's resolution arrives amid a decades-long campaign to restrict independent practice. NP leaders argue that these studies, no matter the results, will be used to limit patient choice and stall progress on nurse practitioner practice authority.3 As the research moves forward, NPs must monitor its design and funding sources, because the findings could directly affect your ability to practice to the full extent of your training and education.
Who Proposed the Resolution and How They Framed It
Rebekah Bernard, MD, a family physician representing the Florida delegation, introduced the resolution that would eventually pass the AMA House of Delegates on June 10, 2026. The proposal, co-sponsored by the Texas and Oklahoma delegations, called for AMA-funded comparative effectiveness studies between autonomous non-physician practitioners and physician-led care models.
The Florida Delegation's Push: Countering NP and PA Advocacy
Bernard argued that state and federal legislators are routinely presented with testimony from NP and PA advocacy groups claiming their care is "just as good or better" than physicians'. She framed the resolution as a necessary step to produce independent evidence, implying that existing research may be influenced by professional interests. Her remarks did not cite specific flawed studies, but she emphasized that lawmakers need academically rigorous data to guide nurse practitioner health policy decisions.
Medicare Data on Chronic Pain Injections and Oversight Gaps
Michael Lubrano, MD, representing the American Academy of Pain Medicine, supported the resolution by referencing Medicare claims data. He described "an explosion of nurse practitioners providing unsupervised advanced chronic pain injection therapies" with unclear oversight. Lubrano did not publicly share the underlying data or detail the volume, geographic spread, or outcomes of these procedures. His testimony raised concerns about patient safety without providing legislators or NP stakeholders with the full dataset needed to verify his assertions.
Conflict-of-Interest Concerns and Legislative Influence
Brandi Ring, MD, of New Hampshire, speaking for the American College of Obstetricians and Gynecologists (ACOG), highlighted what she perceives as a conflict of interest in statehouse hearings. She noted that NP and PA testimony often sways legislators who lack clinical expertise, potentially leading to scope-of-practice expansions without sufficient scrutiny. Ring's concern centered not on the quality of NP care itself, but on the perceived imbalance in advocacy resources and the absence of countervailing physician voices in some legislative settings.
The Word 'Autonomous': A Deliberate Political Choice
The resolution's amended language defines non-physician practitioners as "autonomous" rather than "independent," a distinction that carries political weight. "Autonomous" suggests practice without direct supervision, while "independent" often carries connotations of full, unrestricted authority akin to a physician's license. By choosing "autonomous," the AMA frames NP practice as a deviation from the standard physician-led model, subtly reinforcing the idea that NP-delivered care exists outside the established medical hierarchy. For NPs, this wording signals that the comparative studies will likely scrutinize not just outcomes, but also the legitimacy of the NP role itself.
What Existing Research Already Shows About NP Vs. Physician Outcomes
Nurse practitioners and physicians have been compared in hundreds of studies over the past few decades. A broad consensus has emerged: for many primary care measures, NPs deliver care that is safe, effective, and highly valued by patients. But the details matter, especially when the conversation shifts toward fully autonomous practice without any physician collaboration or oversight.
What decades of research tell us about NP care quality
Large reviews and meta-analyses consistently find that NP-led care achieves outcomes on par with physician-led care for blood pressure control, diabetes management, patient satisfaction, and follow-up adherence. In settings where NPs work in team-based models with physicians, the data are especially strong. The Agency for Healthcare Research and Quality has published multiple evidence reviews confirming that expanding NP practice authority does not harm care quality, and in some cases improves access without increasing costs.
The gap in autonomous practice evidence
The AMA's new study funding targets a very specific scenario: autonomous care with no supervising physician at all. Much existing research was conducted in states or health systems where NPs practiced collaboratively, often with ready access to physician consultation. Critics argue that those findings cannot be automatically extended to independent practice. Proponents note that recent research from independent nurse practitioner states has begun to show similar safety records, but these data sets are still relatively new and often lack long-term follow-up.
Why recent reviews matter for the AMA debate
Systematic reviews published since 2022 have started to examine diagnostic accuracy and care utilization in independent settings. Some show small differences in imaging rates or specialist referrals, while others detect no meaningful gaps in adverse events. The Cochrane Collaboration and independent university research groups are now prioritizing this question, but findings remain mixed. For NPs, understanding these nuances is critical: the AMA studies will likely scrutinize areas where evidence is weakest, such as pain management injections and complex chronic disease management. A closer look at the cost effectiveness of nurse practitioners and care quality across practice models can help frame these conversations. Staying current with the literature will help NPs advocate from a position of evidence rather than anecdote.
Related Articles
NP Training Vs. Physician Training: Putting the Hours Debate in Context
The debate over training differences often reduces to a simple side-by-side of clinical hours, but the full picture includes prior RN experience and evolving competency standards.
Malpractice Rates, Diagnostic Accuracy, and the Evidence Gaps
What the Numbers Say: NP vs. Physician Malpractice Claims
When comparing raw claim frequency, nurse practitioners face far fewer malpractice claims than physicians. National data from 2005 to 2014 show an annual claim rate of roughly 1.1 to 1.4 per 1,000 NPs, compared to 11.2 to 19 per 1,000 physicians.1 In 2023, there were just 1,143 malpractice payment reports involving NPs nationwide.1 The typical annual premium for an NP runs between $800 and $2,200, while a physician may pay around $7,500.
Yet averages can mislead. While NP claims are less common, the average cost of a claim against an NP is not always lower. From 2012 to 2017, the average indemnity payment for NPs was about $300,500.2 For practice-owning NPs, average claim costs jumped to $431,634.3 Diagnosis-related claims alone averaged $385,947, and more than 40% of all claims against NPs and PAs are now tied to diagnostic errors, according to a 2024 liability analysis.1
Understanding the Context Behind Lower NP Claim Rates
The lower frequency of NP claims partly reflects practice patterns. Over half of NP malpractice claims arise in primary care and family practice, with about one-third occurring in physician offices and fewer than one in five in independent NP offices.2 Historically, many NPs worked under collaborative agreements, sharing liability and managing lower-acuity panels. As more states grant full practice authority, the risk profile and claims data may shift. The shorter timeline of independent NP practice also means long-tail trends aren't yet fully captured.
Prescribing and Decision-Making: Where the Evidence Gets Uncertain
Prescribing-related allegations against NPs increased from 16.5% to 29.4% of claims between 2012 and 2017.2 Opioid-related claims carried an average payout of $233,360.4 While some studies suggest NPs may order more imaging or broader-spectrum antibiotics per encounter, these analyses often lack robust risk-adjustment for patient complexity and practice setting. Until AMA-funded or other rigorous, independent studies control for these factors, comparing nurse practitioner diagnostic and prescribing outcomes remains fraught.
Honest Gaps Worth Investigating
Research has yet to definitively assess long-term chronic disease outcomes for patients managed primarily by autonomous NPs, especially in complex or specialty care. Areas like advanced chronic pain injection therapies, cited in the AMA debate, lack clear oversight data. Similarly, direct comparisons of malpractice severity and patient safety outcomes in states with full practice authority versus restrictive environments are thin. These are exactly the gaps the new AMA studies aim to fill, and they're ones where the NP community can proactively contribute evidence.
How These Studies Could Affect NP Scope of Practice and Reimbursement
In full practice authority (FPA) states, primary care visits increased between 2024 and 2026,1 while non-urgent emergency department utilization dropped and total care costs fell, all while quality and safety outcomes remained at the highest standards.2 These real-world numbers put the AMA's newly funded comparative studies in sharp relief. If the AMA-backed research takes a narrow view or uses physician-led care as the only benchmark, it could misrepresent this track record and sway lawmakers considering scope-of-practice bills.
Tracking State-Level Impact
State health department websites often publish annual workforce reports that include NP scope-of-practice impact data. Look at FPA states like Arizona, Montana, Colorado, and Oregon:3 their reports consistently show improved access, lower costs, and no increase in adverse events when NPs practice independently. Reviewing these public documents helps you counter misleading claims with local evidence. If your state is debating FPA, compile the numbers from similar states to present to legislators.
Leveraging National Policy Resources
The American Association of Nurse Practitioners (AANP) policy page is updated regularly with state-by-state comparisons, outcome summaries, and legislative tracking. Their Full Practice Authority Policy Brief compiles peer-reviewed research demonstrating that FPA states achieve better patient functional outcomes and lower utilization of high-cost settings. Bookmark this page and check it when a new study or policy proposal surfaces; it often includes ready-to-use talking points for testimony or media outreach.
Analyzing Economic and Employment Data
The Bureau of Labor Statistics (BLS.gov) offers employment projections and wage data that can be filtered by state and occupation. Compare NP job growth in FPA states versus restricted states and you will typically see faster growth where NPs can practice to the top of their license. BLS cost-of-care data also supports the economic argument: areas with more independent NPs tend to show lower per capita spending. These figures are invaluable when reimbursement models are on the line.
Consulting Independent Research
Organizations like Health Affairs and the RAND Corporation have published rigorous, peer-reviewed studies on FPA impact without the conflicts of interest that can arise in association-funded work. Their analyses often examine multiple dimensions, including access, quality, cost, and patient experience, using large administrative datasets. As the AMA funds its own studies, NPs should be familiar with this independent body of evidence so they can point out methodological gaps or biased framing in new reports. Understanding how advanced nursing is reshaping healthcare positions you to advocate effectively for evidence-based policy, not political posturing.
How NPs Can Advocate and Stay Informed
What can you do today to ensure that nurse practitioner voices and evidence are heard in the scope-of-practice debate?
Engage with Your Professional Organizations
- AANP and state NP associations: These groups are already mobilizing to coordinate the profession's response to the AMA's study funding. Join or renew your membership, attend virtual town halls, and volunteer for advocacy committees. Learning about nurse practitioner organization perks can help you decide which memberships deliver the most value for your advocacy goals.
- Stay informed: Subscribe to legislative alerts and policy briefs. Your association will translate complex developments into clear action steps, so you don't have to monitor every hearing yourself.
Champion NP-Led Research
- Donate to the AANP Foundation: Research grants directly fund independent studies on NP outcomes. Even small contributions help build the evidence base that counters one-sided narratives.
- Participate in practice-based research networks (PBRNs): Many employers collaborate with academic researchers. Volunteer to contribute de-identified data from your patient panel as a way to ground research in real-world practice.
- Document your own outcomes: Start tracking key quality indicators, including readmission rates, patient satisfaction, and chronic disease management benchmarks. Having this data at your fingertips strengthens your voice in any discussion.
Prepare to Speak with Data, Not Just Anecdote
- Know the existing evidence: Bookmark landmark studies like the 2023 Columbia University review showing comparable outcomes, but also understand their limitations. Be ready to discuss study design, not just conclusions.
- Offer to testify or submit written comments: When your state considers scope-of-practice legislation, your association will need NPs who can articulate the data clearly. Practice framing your points around patient safety, access, and cost-effectiveness.
Leverage DNP Education as a Credential
- DNP programs deepen clinical expertise: Earning your Doctor of Nursing Practice signals a commitment to advanced, evidence-based care. In the training-hours debate, it visually reinforces that NP education is rigorous and doctoral-level. If you are weighing the investment, exploring whether a DNP is worth it for your career goals is a practical first step.
- Combine advocacy with academic pursuit: Many DNP capstone projects focus on quality improvement or policy analysis, giving you a direct way to contribute to the profession's research base while advancing your own career.
NP Salary and Career Outlook: Why This Debate Matters for Your Future
The AMA's push for comparative studies has direct economic implications for NPs. Earnings are often higher in states with full practice authority, where NPs can operate independent practices. The table below highlights the top-paying states for nurse practitioners, illustrating the financial stakes of scope-of-practice legislation.
| State | Total Employment | Median Annual Wage | 25th Percentile Wage | 75th Percentile Wage |
|---|---|---|---|---|
| California | 20,980 | $166,610 | $140,260 | $205,400 |
| New Jersey | 9,590 | $149,620 | $126,030 | $162,250 |
| Alaska | 570 | $145,450 | $104,000 | $165,510 |
| New York | 20,430 | $145,390 | $128,190 | $164,670 |
| Oregon | 2,430 | $144,600 | $129,840 | $163,240 |
| Washington | 4,790 | $140,220 | $125,890 | $161,730 |
| Connecticut | 3,680 | $138,960 | $125,910 | $159,680 |
| Massachusetts | 8,920 | $138,890 | $125,590 | $160,310 |
| New Mexico | 1,870 | $138,440 | $113,240 | $156,000 |
| Arizona | 7,540 | $133,790 | $115,290 | $151,650 |
Frequently Asked Questions About the AMA NP Vs. Physician Studies
- What did the AMA vote to do about NP vs physician studies in 2026?
- In June 2026, the AMA House of Delegates voted to fund independent, academically rigorous studies comparing patient outcomes between autonomous non-physician practitioners (including NPs) and physician-led care models. The research will assess safety, quality, utilization, access, cost, and health outcomes, with results intended for publication in a peer-reviewed journal.
- Do nurse practitioners provide the same quality of care as physicians?
- Many studies show that NPs deliver primary and preventive care outcomes comparable to physicians, especially for chronic disease management and patient satisfaction. However, evidence is less consistent for specialized or procedural care. The new AMA-funded studies aim to provide a more definitive analysis, particularly in unsupervised settings, addressing longstanding physician concerns about potential bias in NP-led research.
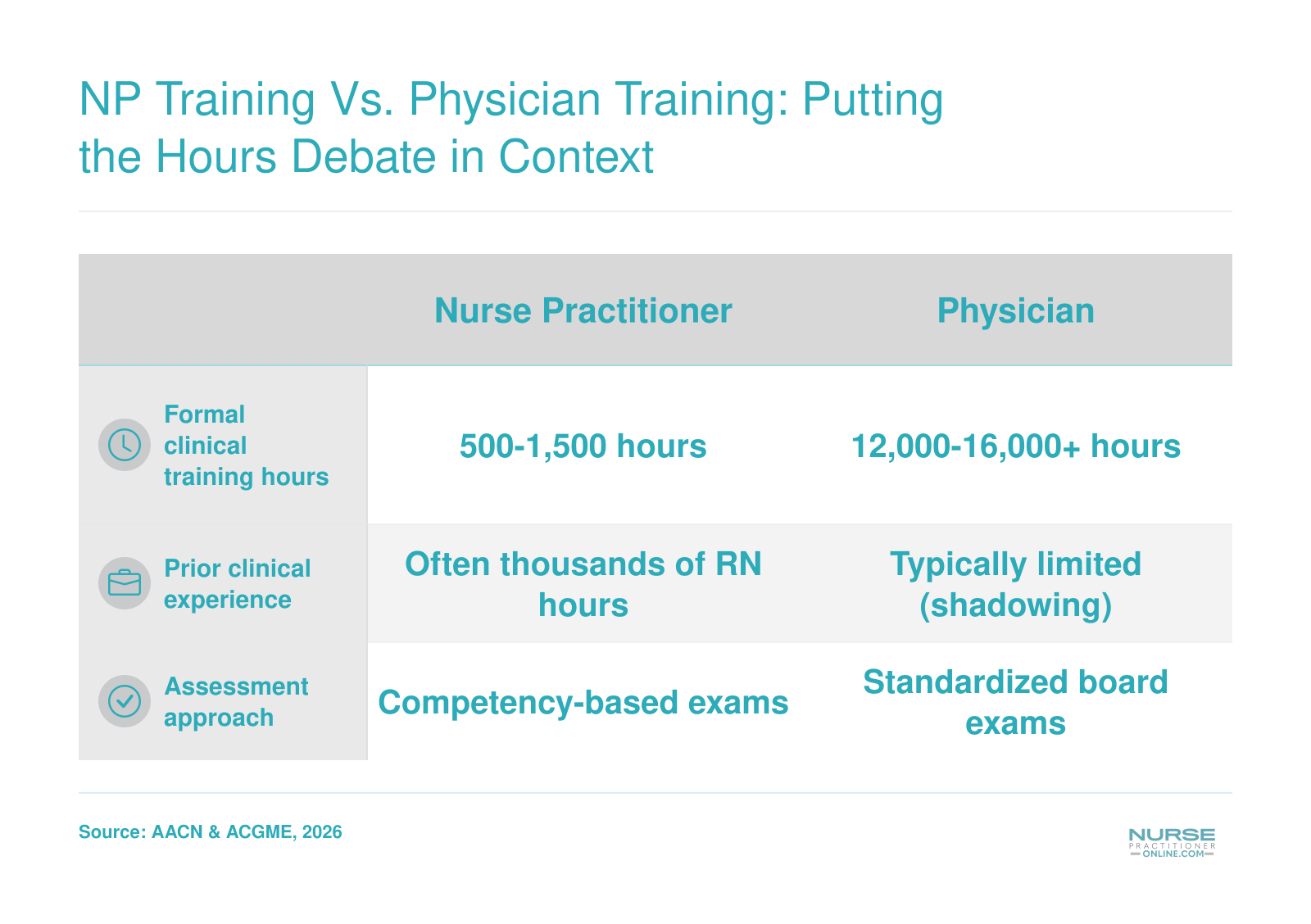
- How many clinical training hours do NPs have compared to physicians?
- NP programs require 500 to 1,500 clinical training hours, while physicians log 12,000 to 16,000 hours between medical school and residency. This disparity is frequently highlighted in scope-of-practice debates. However, NP education emphasizes direct patient care from the outset, whereas physician training includes extensive basic sciences and diagnostic rotations across specialties.
- Can nurse practitioners practice independently without physician oversight?
- As of 2026, more than half of U.S. states grant full practice authority to NPs, allowing them to evaluate, diagnose, and treat patients without physician oversight. Other states mandate collaborative agreements. The AMA's push for comparative studies often targets these independent practice laws, aiming to generate evidence that could either support or challenge the removal of supervision requirements.
- How could AMA-funded studies affect NP scope of practice laws?
- If the AMA-funded studies report poorer outcomes for independent NPs, they could catalyze legislative attempts to restrict scope of practice or reinstate oversight. Convincing positive findings, on the other hand, might accelerate the trend toward full practice authority. Because the AMA wields significant political influence, NPs must stay engaged with this research to ensure fair analysis and robust advocacy.
- What are NP malpractice rates compared to physicians?
- NP malpractice claim rates tend to be lower than those of physicians, particularly in primary care. However, robust data for unsupervised advanced procedures is lacking. The upcoming studies may include liability-related metrics, which could become a focal point in policy debates. NPs should be prepared to interpret such findings in the context of existing evidence and practice settings.