Most important takeaways…
- Twenty seven states plus D.C. now grant nurse practitioners full practice authority, with more legislatures considering similar bills in 2026.
- NP led primary care delivers patient outcomes comparable to physician led care across satisfaction, chronic disease management, and hospitalization rates.
- The Bureau of Labor Statistics projects 40.1% NP employment growth between 2024 and 2034, outpacing nearly every other healthcare occupation.
- AI driven clinical decision support and telehealth are expanding what NPs can manage independently, especially in underserved and rural communities.
More than 385,000 nurse practitioners are in active practice in the United States, and that number is climbing fast enough that health systems, policymakers, and training programs are all struggling to keep pace. NPs now serve as primary care providers for tens of millions of Americans, particularly in rural and underserved communities where physician shortages have made them the default point of first contact.
Three tensions define the profession in 2026. Scope-of-practice authority still varies dramatically by state, meaning the same credential carries different legal weight depending on your zip code. Technology, particularly AI-assisted diagnostics and telehealth infrastructure, is restructuring the clinical day in ways that training programs have not fully caught up to. And the evidence on outcome parity with physician-led care, while increasingly favorable to NPs, continues to sit at the center of an unresolved debate about professional autonomy and reimbursement equity.
For working nurses weighing an NP credential, these are not abstract policy questions. They shape salary ceilings, hiring decisions, and the day-to-day reality of practice. If you are exploring best online MSN nurse practitioner programs, understanding this landscape will help you choose a path that fits both your clinical goals and the regulatory environment ahead. The profession's trajectory over the next decade will be determined as much by legislation and technology adoption as by clinical performance.
A Brief History: How the NP Role Has Evolved Since the 1960S
How did nurse practitioners go from physician assistants in pediatric clinics to independent providers managing complex patient panels across all fifty states?
The nurse practitioner role was born out of necessity. In 1965, pediatric nurse Loretta Ford and physician Henry Silver launched the first nurse practitioner program at the University of Colorado, responding to a critical shortage of primary care physicians, especially in rural and underserved communities. That pilot program trained registered nurses to perform physical exams, assess child development, and provide health education under physician supervision. The model worked. Within five years, similar programs were sprouting nationwide, expanding into family practice, women's health, and adult care. To learn more about the pioneers behind this movement, read about the women who built the nurse practitioner profession.
Legislative Milestones That Shaped the Profession
The road from experimental role to autonomous practitioner was paved by key federal policy decisions:
- 1977 Rural Health Clinic Services Act: Authorized NPs and physician assistants to staff federally qualified health centers, recognizing them as legitimate primary care providers and opening the door to Medicaid reimbursement.
- 1997 Balanced Budget Act: Granted NPs the right to bill Medicare directly, rather than only through supervising physicians, a watershed moment for professional autonomy and practice viability.
- 2010 Affordable Care Act: Positioned NPs as essential to expanding primary care access under healthcare reform, spurring state-level scope-of-practice debates and accelerating the move toward full practice authority.
- 2020-2022 COVID-19 Emergency Waivers: More than thirty states temporarily lifted supervision requirements to address pandemic surges, and many of those changes became permanent law, cementing independent practice as the new standard in much of the country.
From Dependent Role to Doctoral Pathway
In the 1960s, an NP worked only under direct physician oversight, could not prescribe controlled substances, and held at most a master's degree. By 2026, NPs in twenty-seven full practice authority states practice without any physician collaboration agreement, hold full Drug Enforcement Administration prescriptive authority including schedule II opioids, and increasingly enter the workforce with a Doctor of Nursing Practice degree.
That doctoral shift reflects the American Association of Colleges of Nursing's 2004 recommendation that the DNP become the terminal degree for advanced practice by 2015. While the transition remains voluntary and master's-prepared NPs continue to sit for certification, the DNP has become the dominant credential in new-graduate cohorts. If you're weighing the pros and cons, consider exploring DNP entry-to-practice and what it means for the profession's future. The trajectory is clear: the NP of today looks nothing like the nurse of sixty years ago.
NP Scope of Practice by State: Full, Reduced, and Restricted Authority
Where you practice matters almost as much as how you practice. Every state (and the District of Columbia) assigns nurse practitioners one of three authority levels, and those classifications directly shape the patients you can see, the prescriptions you can write, and whether you need a collaborating physician on record. Understanding the landscape is essential before you choose a program, accept a position, or consider relocating.
The Three Tiers, Explained
The American Association of Nurse Practitioners classifies each state's practice environment into three categories:1
- Full Practice Authority (FPA): NPs can evaluate patients, diagnose conditions, order and interpret diagnostic tests, and prescribe medications (including controlled substances) without a mandatory physician oversight agreement. This is the least restrictive model.
- Reduced Authority: NPs can practice to some extent independently, but at least one element of practice, often prescribing, requires a collaborative agreement with a physician or other specified provider.
- Restricted Authority: NPs must work under direct supervision or a formal oversight arrangement for virtually all aspects of clinical practice, including diagnosis and prescribing.
As of mid-2026, the breakdown across all 50 states and D.C. looks like this:
States With Full Practice Authority
A total of 27 jurisdictions now grant FPA: Alaska, Arizona, Colorado, Connecticut, Delaware, the District of Columbia, Hawaii, Idaho, Iowa, Kansas, Maine, Maryland, Massachusetts, Minnesota, Montana, Nebraska, Nevada, New Hampshire, New Mexico, New York, North Dakota, Oregon, Rhode Island, South Dakota, Utah, Vermont, Washington, and Wyoming.1 These states allow NPs to practice to the full extent of their education and certification from day one or after a brief transition period.
States With Reduced Authority
Twelve states currently operate under reduced authority: Alabama, Arkansas, Illinois, Indiana, Kentucky, Louisiana, Mississippi, New Jersey, Ohio, Pennsylvania, West Virginia, and Wisconsin.1 In most of these states, NPs enjoy a good deal of clinical independence but still need a collaborative or supervisory agreement, particularly for prescriptive authority.
States With Restricted Authority
Eleven states maintain the most restrictive framework: California, Florida, Georgia, Michigan, Missouri, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, and Virginia.1 NPs here typically cannot practice without a formalized physician relationship, and the requirements can limit where and how they deliver care.
Recent Trends and What to Watch
No state moved from one category to another between 2024 and mid-2026, which may seem surprising given the momentum of earlier years.1 Advocacy efforts continue in several restricted and reduced states, but legislative progress can be slow. For a deeper look at the forces driving these changes, see our guide on scope of practice for nurse practitioners. If you are weighing career options across state lines, keep an eye on pending bills in states like California and Florida, where large NP workforces have been pushing for broader authority.
Why This Matters for Your Education and Career
Scope-of-practice laws influence more than just day-to-day clinical work. They affect:
- Job availability: FPA states tend to have more independent practice openings, especially in rural and underserved communities.
- Earning potential: Greater autonomy can translate into higher compensation, particularly for NPs who open their own practices.
- Program selection: Some online NP programs tailor clinical placements and coursework to prepare graduates for the regulatory environment in their home state.
- Long-term career planning: If you aspire to lead a clinic or telehealth service, practicing in an FPA state removes a significant administrative hurdle.
Before committing to a program or a new role, check your state's current classification through the AANP's State Practice Environment resource. Rules can shift with a single legislative session, so staying informed protects both your career trajectory and your patients.
Questions to Ask Yourself
How NP Patient Outcomes Compare to Physician-Led Care
The evidence base comparing nurse practitioner and physician outcomes in primary care has grown substantially, and the headline finding is now difficult to dispute: for the vast majority of primary care situations, NPs deliver results that are equivalent to, and in some areas better than, physician-led care.
What the Research Shows on Clinical Outcomes
A two-year randomized trial published in the early 2000s laid important groundwork, finding no meaningful difference between NP and physician patients in health status, hospitalization rates, or overall satisfaction with care.1 That study's findings have held up remarkably well. A 2023 narrative review in the International Journal of Clinical Practice confirmed that clinical outcomes are generally comparable across the two provider types in primary care settings.2 More recent work, including a 2025 systematic review focused on chronic disease management, found that HbA1c levels in patients with diabetes differed by only 0.1 to 0.2 percentage points between NP-led and physician-led panels, a margin too small to carry clinical significance.3 Blood pressure control and other chronic disease markers showed equivalent results as well.
Patient satisfaction tells a similar story. Across multiple studies, satisfaction scores between NP and physician patients differ by roughly 0.1 to 0.3 points on a five-point scale, a gap that falls well within normal measurement variation.3 Hospitalization rates and emergency department use are similar or, in some analyses, slightly lower for NP patients, which may reflect NPs' tendency to invest more time in patient education and follow-up.
Cost-Effectiveness: A Compelling Case
Perhaps the most practically important finding involves cost. Analyses of Medicare claims and large health system data consistently show that NP-led primary care is cost-saving compared with physician-led care, with estimates clustering around 20 to 30 percent lower costs.4 Lower ordering patterns for unnecessary tests and procedures, combined with comparable outcome quality, drive that difference. For health systems grappling with shrinking margins, that figure carries real weight.
Where the Evidence Gets Thinner
Honesty matters here. Most outcome-parity research focuses on primary care, and study designs vary enough that drawing sweeping conclusions across all settings is a stretch. Evidence in acute care vs primary care contexts, complex surgical follow-up, and highly specialized subspecialties is considerably thinner, and the few studies that do exist are harder to compare directly. This is not a reason to dismiss NP competence in those areas; it simply means the research has not caught up yet.
The Practical Takeaway
For primary care, the evidence is clear enough to act on. NP-led care is safe, effective, and meaningfully less expensive, and NPs in 2025 systematic reviews showed higher rates of adherence to clinical guidelines than their physician counterparts.3 That combination makes a strong practical argument for expanding NP scope of practice, particularly in underserved communities where access to any qualified provider is the more pressing concern. If you are considering how to broaden your own impact, exploring nurse practitioner advancement opportunities is a natural next step.
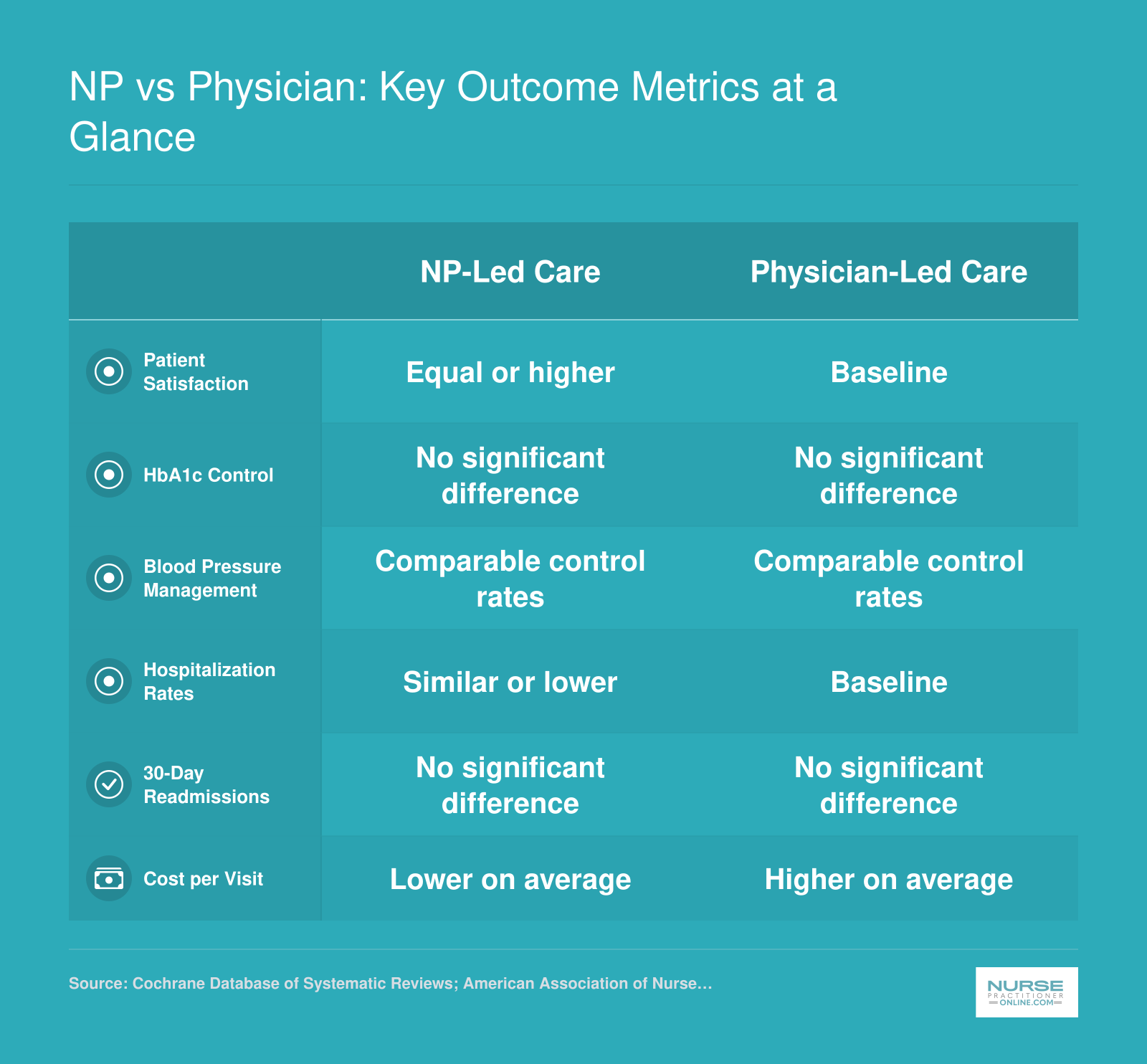
NP vs Physician: Key Outcome Metrics at a Glance
Research consistently shows that nurse practitioner-led primary care delivers outcomes comparable to, and in some cases better than, physician-led care. Here is how the two models stack up across key quality and cost measures.
NP Workforce Growth, Salary, and Employment Snapshot
The nurse practitioner profession is expanding faster than nearly any other occupation in the country. According to the Bureau of Labor Statistics, NP employment is projected to grow 40.1% between 2024 and 2034, making it the fastest growing healthcare occupation and the third fastest growing occupation overall. The table below highlights the top 25 states by median annual salary, along with total employment in each state, to help you gauge where opportunity and compensation are strongest.
| State | Total Employment | Median Annual Salary | 25th Percentile Salary | 75th Percentile Salary |
|---|---|---|---|---|
| California | 20,980 | $166,610 | $140,260 | $205,400 |
| New Jersey | 9,590 | $149,620 | $126,030 | $162,250 |
| Alaska | 570 | $145,450 | $104,000 | $165,510 |
| New York | 20,430 | $145,390 | $128,190 | $164,670 |
| Oregon | 2,430 | $144,600 | $129,840 | $163,240 |
| Washington | 4,790 | $140,220 | $125,890 | $161,730 |
| Connecticut | 3,680 | $138,960 | $125,910 | $159,680 |
| Massachusetts | 8,920 | $138,890 | $125,590 | $160,310 |
| New Mexico | 1,870 | $138,440 | $113,240 | $156,000 |
| Arizona | 7,540 | $133,790 | $115,290 | $151,650 |
| Montana | 1,050 | $133,640 | $112,180 | $141,050 |
| New Hampshire | 1,790 | $132,440 | $120,270 | $143,010 |
| District of Columbia | 790 | $131,380 | $119,240 | $143,960 |
| Hawaii | 470 | $130,940 | $121,410 | $158,100 |
| Rhode Island | 1,200 | $130,710 | $126,200 | $160,030 |
| Texas | 21,690 | $129,880 | $110,570 | $143,860 |
| Colorado | 4,130 | $129,750 | $110,300 | $139,440 |
| Vermont | 680 | $129,740 | $115,650 | $139,930 |
| Iowa | 2,810 | $129,420 | $115,950 | $137,900 |
| Florida | 24,690 | $129,010 | $109,670 | $143,670 |
| Idaho | 1,570 | $128,940 | $119,290 | $140,920 |
| Illinois | 9,560 | $128,620 | $111,450 | $138,420 |
| Wisconsin | 4,950 | $128,580 | $117,630 | $137,150 |
| Minnesota | 8,690 | $128,570 | $103,250 | $139,590 |
| Indiana | 7,470 | $128,280 | $111,210 | $134,840 |
Related Articles
How AI, Telehealth, and Technology Are Reshaping NP Practice
Technology is moving faster than most practice settings can absorb, and nurse practitioners sit squarely at the intersection of that tension. The tools arriving in clinical workflows right now carry real potential to reduce cognitive load and extend what a single NP can accomplish in a day, but adoption is uneven, evidence is still accumulating, and the data specific to NP practice is not yet fully published.
What the Broader Health System Data Tells Us
A 2024 survey of health systems found that 86 percent had adopted artificial intelligence in some capacity, and 60 percent reported that AI had improved diagnostic accuracy within their organizations.1 A follow-up analysis published in 2025 found that the most common starting points for AI implementation were radiology interpretation, sepsis alerts, readmission risk prediction, and documentation assistance. Clinical decision support, operational efficiency, and population health management rounded out the primary deployment areas.2
These findings matter for NPs because most of those use cases map directly onto primary and specialty care settings where primary care nurse practitioners practice. Sepsis alert tools, for example, are already present in many emergency and acute care environments where NPs hold independent or collaborative roles. Documentation assistance tools, which use ambient voice capture or natural language processing, are reducing charting burden in outpatient clinics, freeing time that can return to direct patient interaction.
Where NP-Specific Data Stands Right Now
Here is the honest picture: program-level and occupation-specific data on AI adoption rates and telehealth utilization among NPs is not yet available for the 2024 to 2026 window. The AANP's detailed NP Practice Survey, which will capture this information, is expected to release in 2027.3 Until that data is public, claims about how many NPs are using specific tools or platforms should be read with caution.
What is documented is that during and after the COVID-19 pandemic, nurses internationally expanded their use of telehealth, mobile health applications, and remote monitoring platforms for triage, chronic disease follow-up, and patient education.4 NPs, as advanced practice nurses with prescriptive authority and diagnostic responsibility, were among those driving that expansion in primary care and specialty settings.
Practical Technology Shifts Worth Watching
Separate from AI, mobile device use is reshaping point-of-care workflows. Roughly 69 percent of providers now use mobile devices to access patient information, a shift that has changed how NPs document, communicate with teams, and review results between appointments.5 If you are looking for tools that can streamline your clinical day, our roundup of best apps for nurse practitioners is a good place to start.
For NPs considering how to future-proof their practice, a few areas stand out:
- Clinical decision support: AI-assisted tools are entering EHR platforms that NPs already use, often without a separate adoption decision.
- Remote patient monitoring: Chronic disease management, particularly for hypertension and diabetes, is increasingly supported by devices that feed data directly into the patient record.
- Telehealth continuity: What began as a pandemic-era workaround has stabilized into a standard care modality in many states, particularly for behavioral health and follow-up visits.
The NPs who will navigate this shift most effectively are those who stay close to peer networks, read emerging AANP and HIMSS guidance as it publishes, and treat technology as a workflow question rather than a purely technical one. The tools are changing; the clinical judgment required to use them well is still yours.
For anyone tracking nurse practitioner practice, the AANP's National NP Practice Survey is a must-read, but you might be surprised that its 2024 edition contained no publicly reported data on telehealth adoption rates, a statistic that has become critical as virtual care reshapes healthcare delivery.
NP Specializations Driving the Profession Forward
Generalist family practice still anchors the profession, but specialty practice is where the fastest growth, the highest reimbursement, and the most interesting clinical evolution are happening right now. If you are mapping a long career, choosing a specialty track shapes your patient population, your earning ceiling, and how portable your credentials will be across state lines. For a broader look at how different paths compare, explore our guide to nurse practitioner specialties.
Five Specialties Reshaping the Field
- Psychiatric-Mental Health NP (PMHNP): Demand is the highest in the profession, driven by a national mental health crisis, a shrinking psychiatrist workforce, and the fact that psychiatric care translates exceptionally well to telehealth. The role has evolved from medication management under physician oversight to full diagnostic and therapeutic responsibility, with many PMHNPs running independent telepsychiatry practices that carry waitlists of weeks to months.
- Acute Care NP (ACNP): Hospital systems are leaning on ACNPs to staff ICUs, step-down units, and specialty inpatient services as hospitalist coverage tightens. The role has shifted from procedural support to leading rounds, managing ventilated patients, and serving as the continuity provider across shift changes.
- Oncology NP: An aging population and a growing pipeline of targeted therapies have created sustained demand for NPs who can manage survivorship, immunotherapy side effects, and complex symptom regimens. Many oncology NPs now run their own survivorship and chemotherapy education clinics.
- Neonatal NP (NNP): NICU coverage gaps, particularly in regional referral centers, keep NNP demand steady. The role has expanded into transport medicine, family conferencing, and end-of-life decision support.
- Dermatology NP: Cosmetic and medical dermatology continue to outpace dermatologist supply, and NPs increasingly own procedural workflows including biopsies, excisions, and aesthetic injectables.
Certification and Career Mobility
Specialty certification through the American Association of Nurse Practitioners (AANP) or the American Nurses Credentialing Center (ANCC) is not just a credential; it is your reimbursement key. Payers tie billing privileges to specific certifications, and hospital credentialing committees use them as the baseline for privileging. Holding a recognized specialty certification also makes interstate moves smoother, since most state boards map licensure tracks directly to AANP and ANCC categories. Understanding how NP specialties compare by salary can help you weigh the financial side of these decisions.
Emerging Frontier Roles
Keep an eye on three sub-specialties drawing experienced NPs: palliative care, gender-affirming care, and substance use disorder treatment. Each sits at the intersection of clinical complexity, workforce shortage, and policy momentum, and each is producing fellowship pathways that did not exist five years ago. If psychiatric care interests you, our deep dive into PMHNP sub-specialties and patient populations is a great place to start narrowing your niche.
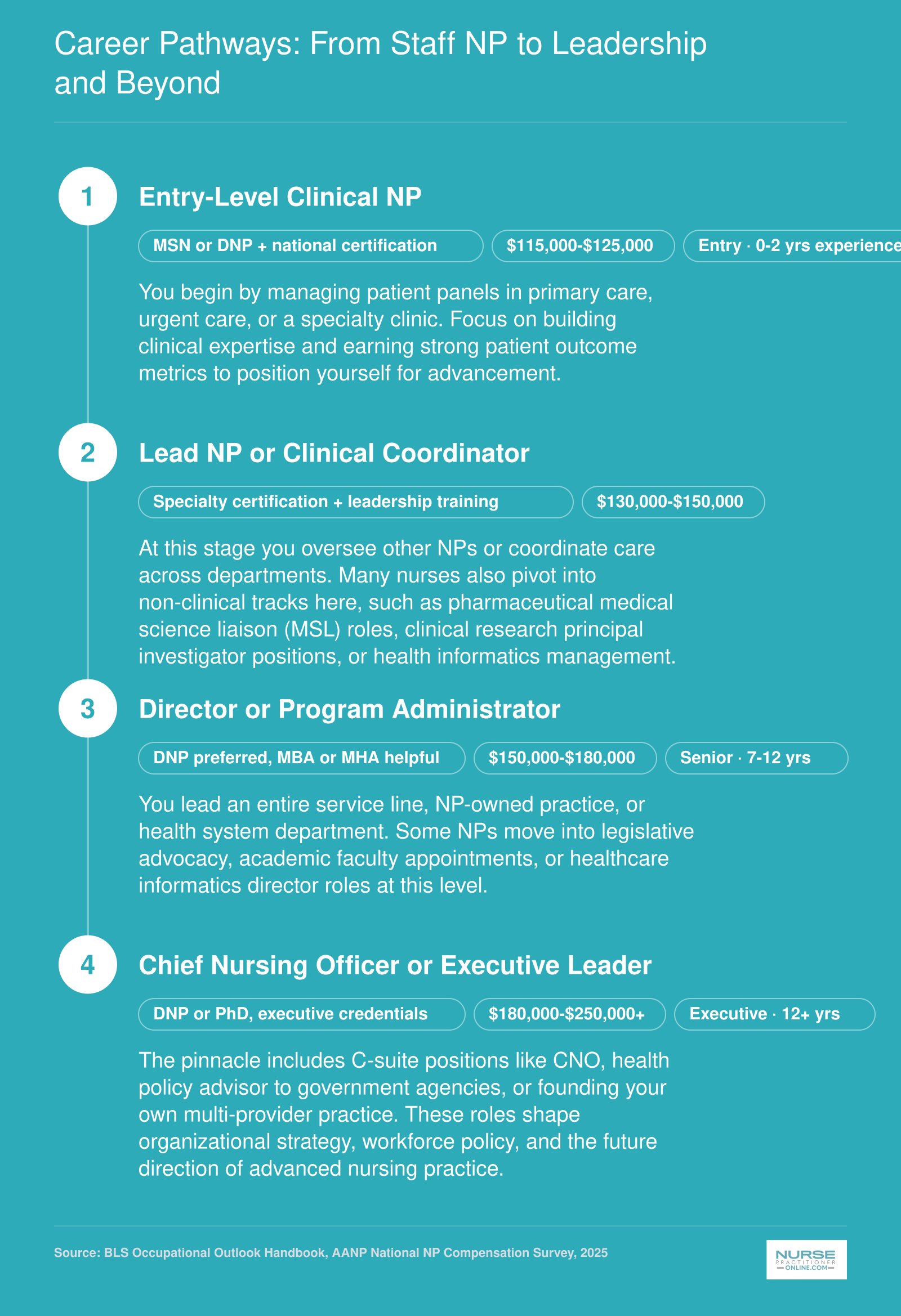
Career Pathways: From Staff NP to Leadership and Beyond
Your nurse practitioner degree opens far more doors than a single clinical role. Whether you want to lead a care team, shape health policy, or launch your own practice, there is a clear progression from your first NP position to senior leadership and beyond. Here is how working NPs typically map out their careers.
Barriers, Controversies, and What's Next for NPs
The nurse practitioner profession stands at an inflection point where hard-won clinical credibility now collides with structural obstacles that shape daily practice. For nurses considering the NP path, understanding these barriers alongside emerging opportunities offers essential context for career planning.
The Physician-NP Practice Authority Debate
The question of independent practice remains the profession's most visible fault line. The American Medical Association maintains that physician-led care teams produce the safest outcomes and that NP education, while rigorous, does not match the depth of medical residency training. From this perspective, collaborative practice requirements protect patients.
The American Association of Nurse Practitioners counters that decades of outcome data demonstrate NPs deliver equivalent care quality in primary settings, and that restricting practice authority limits healthcare access in underserved communities. Both sides present legitimate concerns rooted in patient welfare, though the practical effect of restrictive laws often falls hardest on rural and low-income populations.
As of 2026, the legislative trend favors expanded authority. More than half of states now grant full practice status, with several others actively debating reform bills. If you want to help shape these outcomes, our nurse practitioner health policy toolkit offers practical steps for getting involved.
Reimbursement Inequity and Its Ripple Effects
Beyond practice authority, payment structures create ongoing friction. Medicare reimburses NPs at 85 percent of physician rates for identical services, a policy established in 1997 that persists despite evolving evidence on care equivalence. This gap affects not only NP compensation but also employer hiring decisions and the financial viability of NP-led clinics in rural markets.
Reform efforts have gained momentum, with congressional proposals to equalize reimbursement appearing in recent sessions. Advocates argue that payment parity would strengthen the primary care pipeline precisely when workforce projections show growing demand.
Burnout and Workforce Retention
Workload sustainability presents an urgent challenge. National survey data from 2022 found that over 60 percent of NPs reported burnout symptoms, with 30 percent experiencing concurrent depression.1 Perhaps most concerning, 31 percent indicated intent to leave the profession entirely.1
Contributing factors illuminate systemic issues rather than individual resilience failures. Bureaucratic tasks topped the list at 49 percent, followed by insufficient compensation and perceived lack of respect, each cited by 43 percent of respondents. When asked what would help, 50 percent identified increased compensation and 40 percent pointed to greater professional respect.1
Regional data from primary care NPs in New Jersey and Pennsylvania showed that supportive practice environments could reduce burnout risk by 51 to 58 percent, underscoring how workplace culture shapes sustainability.2
The DNP Transition Debate
Whether doctoral preparation should become the standard entry point divides the profession. Proponents argue the Doctor of Nursing Practice degree elevates clinical competency, strengthens the profession's standing, and prepares NPs for increasingly complex care environments.
Critics worry that adding years and expense to training will shrink the applicant pipeline, particularly among working nurses balancing family obligations and student debt. With primary care shortages projected through the next decade, some question whether the timing serves workforce needs. Graduate programs continue offering both master's and doctoral pathways, and the debate remains unresolved.
Looking Forward Through 2030
Several forces will shape the NP role in coming years. Legislative momentum toward full practice authority continues, with advocacy organizations tracking active bills across multiple states. The states with the most need for nurse practitioners highlight where workforce gaps are most acute. Federal agency projections anticipate sustained demand for primary care providers as physician retirements accelerate and population health needs grow.
Technology adoption will likely expand NP capacity rather than replace it. Telehealth integration, clinical decision support tools, and AI-assisted documentation show early promise for reducing administrative burden while maintaining care quality. Outcome data collected at scale may ultimately inform both scope-of-practice debates and reimbursement reform.
For nurses evaluating the NP path today, the profession offers genuine opportunity alongside real structural challenges. Understanding both prepares you to navigate a career where advocacy and clinical excellence remain inseparable.
Frequently Asked Questions About Nurse Practitioners
These are some of the most common questions nurses and prospective NP students ask about the profession's trajectory. Each answer draws on themes explored throughout this guide, so you can dig deeper into any topic that resonates with your career goals.
- What is the evolving role of nurse practitioners in healthcare?
- Nurse practitioners have expanded well beyond their original 1960s scope as physician extenders in underserved clinics. Today, NPs diagnose conditions, prescribe medications, lead care teams, and practice independently in many states. As discussed in the history section of this guide, the role continues to grow into specialties such as psychiatric mental health, acute care, and population health management, driven by workforce shortages and policy changes.
- How do nurse practitioner patient outcomes compare to physicians?
- Multiple studies show that NP-led care produces comparable or equivalent patient outcomes in primary care settings, including patient satisfaction, chronic disease management, and hospital readmission rates. As outlined earlier in this article, research consistently demonstrates that NPs deliver safe, high-quality care. These findings have been instrumental in advancing full practice authority legislation across the country.
- What states allow nurse practitioners full practice authority?
- As of 2026, more than half of U.S. states and the District of Columbia grant NPs full practice authority, meaning they can evaluate patients, diagnose, order tests, and prescribe medications without physician oversight. The scope of practice section of this guide breaks down state-by-state classifications into full, reduced, and restricted authority categories so you can see exactly where your state stands.
- What is the future of nurse practitioners in the US?
- The future looks strong. The Bureau of Labor Statistics projects rapid growth in NP employment through the early 2030s, far outpacing the average for all occupations. Aging populations, expanded insurance coverage, and physician shortages in rural areas will continue driving demand. As this guide explores, NPs are also moving into leadership, policy, and entrepreneurial roles at increasing rates.
- How is AI changing the nurse practitioner role?
- Artificial intelligence is augmenting NP practice through clinical decision support, predictive analytics, and streamlined documentation. AI-powered tools can flag early warning signs in patient data and help NPs prioritize complex cases. As discussed in the technology section of this article, these tools are designed to support, not replace, clinical judgment, freeing NPs to spend more time on direct patient interaction and relationship building.
- What are the benefits of nurse practitioners in primary care?
- NPs improve access to care, especially in rural and medically underserved communities where physician availability is limited. They typically spend more time per visit with patients, emphasize preventive care and patient education, and often reduce overall healthcare costs. Studies cited throughout this guide show that NP-staffed primary care clinics report strong patient satisfaction scores and effective chronic disease outcomes.
- Can a nurse practitioner open their own practice?
- Yes, but it depends on your state's scope of practice laws. In full practice authority states, NPs can independently own and operate clinics without a collaborative agreement with a physician. In reduced or restricted authority states, you may need a formal physician partnership. The scope of practice section earlier in this article can help you determine the requirements in your state before taking the entrepreneurial leap.