Most important takeaways…
- About half of U.S. states plus D.C. now grant nurse practitioners full practice authority as of 2026.
- FNPs hold the widest patient age span of any NP specialty, covering newborns through older adults.
- Full practice authority increases NP self-employment probability by 374.1%, expanding access in underserved communities.
- Collaborative agreement requirements vary widely, and your intended practice state should shape your program choice.
Twenty-seven states plus D.C. and two U.S. territories now grant nurse practitioners full practice authority, with Utah and New York joining the column in the past two legislative cycles and bills active in at least six more states heading into 2026. That number was 22 in 2020.
For a working RN weighing a $35,000 MSN-FNP program, this matters in concrete ways. Your state's classification (full, reduced, or restricted) dictates whether you can prescribe Schedule II controlled substances without a collaborating physician, whether you can open your own clinic, and whether a hospital will pay you closer to $115,000 or $145,000. It also shapes whether a collaborative agreement will cost you $500 a month out of pocket. Understanding how nurse practitioner salary by state and specialty connects to practice authority can sharpen your program calculus considerably.
The regulatory map is no longer static, and program choice, license portability, and starting salary are all downstream of it.
What Is NP Scope of Practice and Why Does It Matter?
An NP in New Mexico can open an independent clinic on day one after licensure, while an NP in California with identical credentials must work under a physician's supervision for years before gaining that same autonomy. The difference comes down to scope of practice, and understanding it shapes every career decision you will make.
Scope of Practice Defined
Scope of practice is the legal framework that defines exactly which clinical activities a nurse practitioner can perform. This includes conducting patient assessments, ordering and interpreting diagnostic tests, diagnosing conditions, prescribing medications (including controlled substances), and developing treatment plans. Think of it as the boundaries of your professional authority. Everything inside those boundaries is something you can legally do; everything outside requires referral or collaboration with another provider.
Here is the critical point most nursing students miss: scope of practice is determined at the state level, not federally. Congress does not set these rules. Each state legislature and board of nursing establishes its own regulations. This means your clinical authority changes the moment you cross a state line. Two family nurse practitioners who graduated from the same program, passed the same national certification exam, and have the same years of experience may have completely different legal powers depending on their practice location. Our breakdown of nurse practitioner practice authority by state maps exactly which states grant full, reduced, or restricted authority.
Why Scope Matters Beyond Patient Care
The impact of scope of practice extends well beyond your clinical responsibilities:
- Reimbursement eligibility: In states with full practice authority, NPs can bill Medicare and most private insurers directly at 85 to 100 percent of physician rates. Restricted states may require billing through a supervising physician, which can complicate payment and limit your earning potential.
- Practice ownership: Full practice authority allows you to open and operate your own clinic without a collaborating physician. Restricted scope may legally prevent independent ownership or require ongoing physician relationships that cost money and limit flexibility.
- Malpractice exposure: Collaborative agreements can shift some liability to supervising physicians, but they also create documentation requirements and may limit your clinical decision-making. The legal structure affects your insurance rates and risk profile.
- Rural healthcare access: Many underserved communities lack physicians. In full practice authority states, NPs can fill these gaps independently. Restricted scope creates barriers that leave some communities without adequate primary care.
Scope vs. Certification vs. Licensure
These three terms are often confused, but they represent distinct concepts. Certification comes from passing a national board examination through organizations like the American Academy of Nurse Practitioners or the American Nurses Credentialing Center. It validates your knowledge and specialty training. Licensure is the state-issued permission to practice nursing at all. You cannot work as an NP without an active license in your state. Scope of practice then defines what that license actually allows you to do, and that varies dramatically depending on where you hold it.
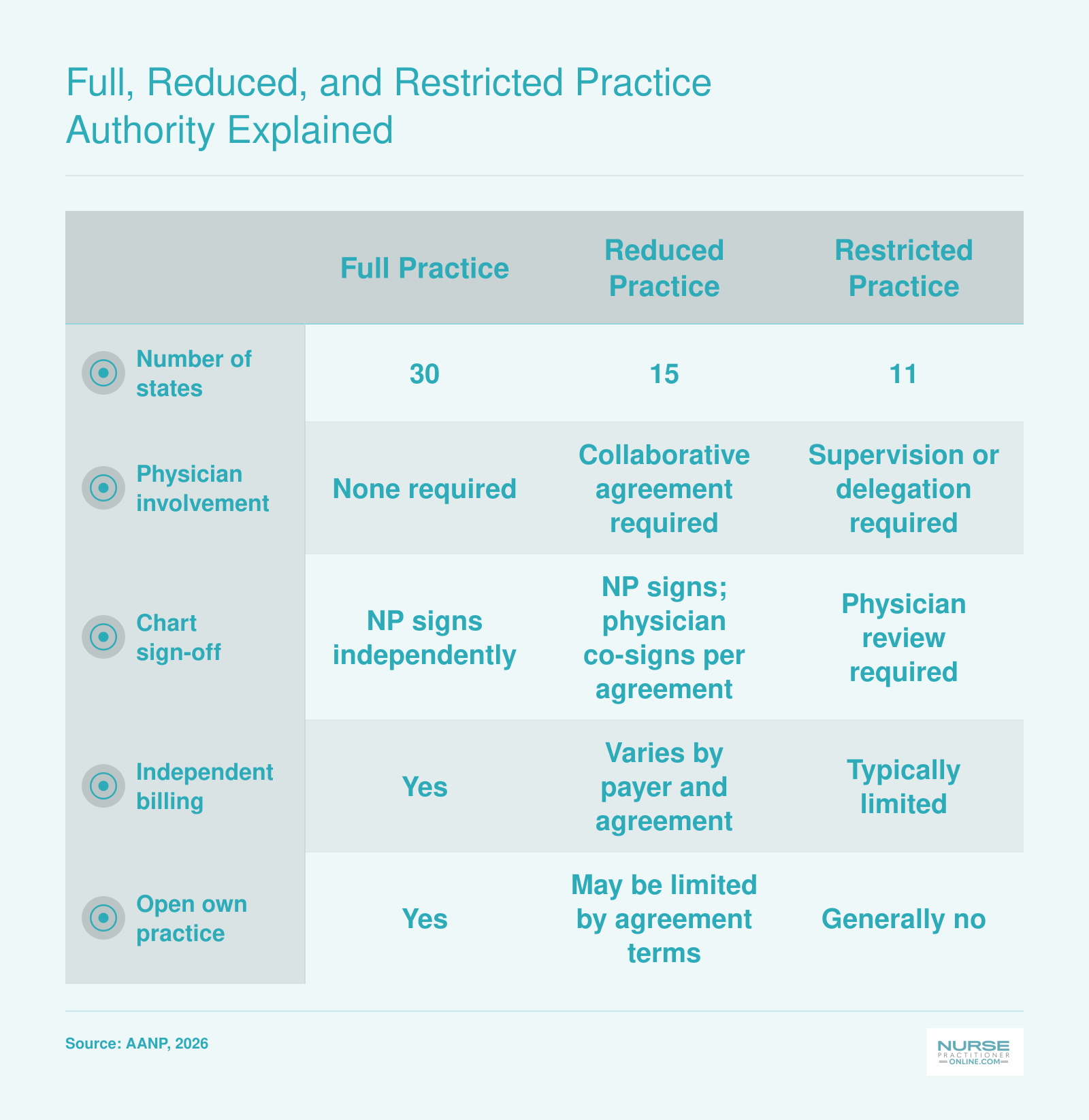
Full, Reduced, and Restricted Practice Authority Explained
The American Association of Nurse Practitioners classifies every state (plus D.C.) into one of three practice authority categories. Understanding which category your state falls into tells you how independently you can practice, whether you need a collaborating physician, and how easily you can launch your own clinic. As of 2026, no states have changed classification since 2024, so these counts remain stable.
NP Scope of Practice by State: The 2026 Landscape
The map keeps tilting toward independence. As of 2026, roughly half of U.S. states plus the District of Columbia grant nurse practitioners full practice authority, and several state legislatures have active bills that would push more jurisdictions into that column over the next two years.1 For working nurses planning a degree investment, where you live (or plan to license) increasingly shapes what your FNP role will actually look like day to day.
What the Three Tiers Actually Mean
The American Association of Nurse Practitioners groups states into three categories. Full practice states let NPs evaluate patients, diagnose, order and interpret tests, and prescribe (including controlled substances) under the exclusive licensure authority of the state board of nursing. Reduced practice states require a regulated collaborative agreement with another health provider for at least one element of practice. Restricted practice states require career-long supervision, delegation, or team management by another health provider for the NP to provide patient care.
Where Each State Stands in 2026
The table below reflects publicly reported classifications as of early 2026.1 Because legislation moves quickly, always confirm current status with your state board of nursing before making a licensure decision.
- Full practice authority: Alaska, Arizona, Colorado, Delaware, Hawaii, Idaho, Kansas, Maine, Maryland, Massachusetts, plus additional states historically in this group (Connecticut, Iowa, Minnesota, Montana, Nebraska, Nevada, New Hampshire, New Mexico, North Dakota, Oregon, Rhode Island, South Dakota, Vermont, Washington, Wyoming) and the District of Columbia.
- Reduced practice authority: Alabama, Arkansas, Illinois, Indiana, Kentucky, Louisiana, Mississippi, New Jersey, Ohio, Pennsylvania, along with other states in this tier (Utah, West Virginia, Wisconsin, and historically New York under transition-to-practice rules).
- Restricted practice authority: California, Florida, Georgia, Michigan, Missouri, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, and Virginia.
What to Watch
A handful of states have shifted classification or carved out partial independence pathways in the last 24 months, often by letting experienced NPs drop a collaborative agreement after a set number of supervised hours. New York's transition-to-practice model and California's AB 890 phased independence rules are well-known examples of this hybrid approach. Pending bills in several reduced and restricted states would either expand prescriptive authority for controlled substances or eliminate physician collaboration requirements outright.
If your state sits in the reduced or restricted tier, factor two things into your FNP program decision: the cost and availability of a qualifying collaborating physician, and whether multistate licensure through the APRN Compact (still rolling out in 2026) could give you a workaround. Staying informed on these legislative shifts is easier than you might think; our nurse practitioner health policy toolkit walks you through practical ways to track and influence bills in your state.
Questions to Ask Yourself
What Can a Family Nurse Practitioner Do? FNP-Specific Scope
Family nurse practitioners hold the widest age span of any NP role.1 Where a psychiatric mental health NP focuses on behavioral health and an adult-gerontology nurse practitioner works with hospitalized adults, an FNP cares for patients across the entire lifespan: newborns, children, adolescents, adults, pregnant patients, and older adults. That generalist scope is what makes FNPs the most versatile primary care NPs and the most in-demand hire in family medicine clinics, community health centers, retail clinics, and rural practices.
Clinical Tasks an FNP Performs Every Day
The day-to-day clinical work of an FNP looks a lot like a primary care physician's. Typical responsibilities include:
- Assessment and diagnosis: Comprehensive history-taking, physical exams, and diagnosis of acute and chronic conditions such as hypertension, type 2 diabetes, asthma, depression, and anxiety.1
- Diagnostics: Ordering and interpreting labs, imaging, ECGs, spirometry, and point-of-care testing.
- Treatment planning: Developing and adjusting care plans, prescribing medications, and counseling on lifestyle modifications.
- Procedures: Laceration repair, cryotherapy of skin lesions, punch biopsies, joint and trigger-point injections, and splinting.
- Women's health: Pap smears, contraceptive counseling, IUD insertion and removal, and contraceptive implant placement. In California, FNPs can also provide first-trimester abortion care under SB 1375.3
- Lifespan care: Well-child visits, ADHD management, geriatric syndrome assessment, multimorbidity management, and advance care planning.
- Care coordination: Referrals to specialists, transitions of care, and preventive health counseling.
What an FNP Can Do That an RN Cannot
The RN-to-FNP jump is significant. As an RN, you implement a plan of care. As a family nurse practitioner, you create it. FNPs make independent clinical decisions, assign diagnoses, prescribe medications, order diagnostics, and refer patients to specialists, all of which fall outside the RN scope. That diagnostic and prescriptive authority is the legal core of what separates advanced practice from registered nursing.
Prescriptive Authority and Controlled Substances
FNPs in full-practice states (Arizona, Colorado, Oregon, Washington, New York, and roughly 20 others as of 2026) prescribe Schedule II through V controlled substances independently.2 In reduced or restricted states, you'll need a collaborative or supervisory arrangement to prescribe. Every prescribing FNP needs a federal DEA registration, and many states layer on their own controlled substance certificate plus mandatory opioid prescribing CE.
Hospital Privileges
Most FNPs work in outpatient primary care, but hospital credentialing is increasingly common. Many health systems grant FNPs admitting, rounding, or co-management privileges, particularly in rural hospitals and integrated delivery networks where the FNP follows their primary care panel through inpatient stays.
FNP vs PA vs Physician: How Scope of Practice Compares
The lines between advanced practice providers and physicians are blurring in some areas while remaining distinct in others, making it more important than ever to understand how these three roles compare structurally. If you are weighing an FNP career against other clinical paths, or simply want to articulate your value to employers and patients, knowing these differences will serve you well.
Education Pathway and Training Model
Family nurse practitioners follow a nursing model of education, building on RN experience and completing a graduate degree (typically an MSN or DNP) with population-focused clinical training.1 Physician assistants complete a medical model program, usually a master's degree, with generalist training across specialties.1 Physicians pursue the most extensive path: four years of medical school followed by three to seven years of residency, with fellowship training for subspecialties.
These different foundations shape how each provider approaches patient care. FNPs often emphasize holistic, patient-centered care rooted in nursing theory, while PAs and physicians typically train within a disease-centered medical framework.
Supervision and Collaboration Requirements
This is where structural differences become most apparent:
- FNPs: In full practice authority states (28 or more as of 2023), FNPs practice independently with no required physician oversight. In reduced or restricted states, collaborative agreements with physicians remain mandatory.
- PAs: Historically required a formal supervisory relationship with a physician. However, the PA profession is increasingly advocating for Optimal Team Practice, which removes mandatory supervision requirements in favor of collaborative care.3
- Physicians: Practice independently and often serve as supervisors for other providers.
Both FNPs and PAs are trending toward greater autonomy, though through different regulatory channels. FNPs work through state boards of nursing, while PAs typically fall under medical boards.4
Prescriptive Authority
Prescribing medications, including controlled substances, is essential for primary care. In full practice authority states, FNPs prescribe independently without physician sign-off. PAs generally have prescriptive authority that is conditional on their collaborative agreement with a supervising physician.5 Physicians, of course, prescribe without restriction. For FNPs interested in delivering primary care autonomously, this prescriptive independence is a major professional advantage, and it strengthens the case for nurse practitioners as primary care providers.
Practice Independence and Business Ownership
FNPs in full practice authority states can own and operate their own practices, a significant advantage for those interested in entrepreneurship or rural healthcare delivery.6 PA practice ownership is more limited, typically requiring a physician relationship to meet state requirements.6 Physicians face no such restrictions.
Specialty Flexibility: A Key Structural Difference
Here is a distinction that surprises many nurses considering advanced practice: FNP scope is specialty-locked to your certification population. As a certified family nurse practitioner, you are certified to provide primary care across the lifespan. If you want to practice in a field like psychiatric-mental health nurse practitioner care, you need additional certification.
PAs, by contrast, are trained as generalists who can shift specialties based on their supervising physician's practice. A PA can move from orthopedics to family medicine without additional certification, though they may need on-the-job training.1
Physicians have specialty flexibility after completing residency, but changing specialties typically requires additional fellowship or residency training.
The Convergence Trend
Both NPs and PAs are moving toward greater independence, though through different mechanisms. NPs are pursuing full practice authority state by state through nursing boards. PAs are advocating for Optimal Team Practice through medical boards and state legislatures.4 The practical result is that both professions are trending toward autonomous practice, which may reshape how healthcare teams function in the coming decade.
Understanding these distinctions helps you make informed decisions about your career path and communicate your value clearly to employers, collaborators, and patients.
How Collaborative Agreements and Supervision Actually Work
What a Collaborative Agreement Actually Covers
A collaborative agreement is not just a piece of paper. It is a legally binding contract that dictates how, when, and under what conditions you can assess, diagnose, and treat patients. The specifics vary by state, but most agreements include several common elements.
- Chart review frequency: In Texas, for example, the supervising physician must review at least 10% of the NP's patient charts each month. Some states mandate quarterly reviews; others leave it to the agreement itself.
- Consultation protocols: The agreement spells out when you must contact your collaborating physician, for instance, for new diagnoses outside your core specialty, abnormal test results, or patient deterioration. It may require immediate phone availability or simply a callback within a certain timeframe.
- Physician availability: Some states require the physician to be physically on-site a set number of hours per week or month. Others allow off-site availability by phone or electronic communication. On-site requirements can make it difficult to practice in rural or underserved areas where a physician simply is not present.
- Prescriptive authority delegation: This is often a separate layer. In Georgia, prescriptive authority is delegated through a nurse protocol agreement that must be filed with the state medical board.1 In Texas, the NP needs a separate prescriptive authority agreement that names the supervising physician and lists the drugs or categories the NP may prescribe.
Together, these components create a supervisory net that can range from active clinical mentoring to a costly contractual obligation that rarely involves meaningful oversight.
The Hidden Price Tag: What NPs Pay for Supervision
The financial burden of collaborative agreements is rarely discussed openly, but it is a very real line item for many NPs. In restricted and reduced practice states, NPs often must pay a physician for the privilege of being supervised, because the physician is assuming legal liability and sometimes lending their name and license to the practice.
Monthly payments can range from $500 to well over $2,000, depending on the specialty, geographic area, and the physician's perceived risk. That adds up to $6,000 to $24,000 or more annually, a significant overhead cost that can make the difference between a thriving independent practice and one that never gets off the ground. For NPs who want to open a clinic in a community where a physician collaborator is scarce, the price is not just financial; it can be an insurmountable barrier to care access.
State-by-State: How Requirements Actually Differ
- Texas (restricted practice): NPs must have a written delegation and supervision agreement with a physician. That agreement must include a quality assurance plan, and the physician must review at least 10% of charts monthly. Prescriptive authority requires a separate agreement, and the physician's name appears on every prescription. The physician does not need to be on-site at all times but must be available for consultation.
- California (reduced practice, with a new FPA pathway): For NPs who have not met the AB 890 requirements (3 years and 4,600 hours of practice), they still operate under standardized procedures developed in collaboration with a physician.3 Those procedures define the scope of practice and prescribing. Under the 103 NP pathway, after meeting experience requirements, NPs can apply for full independent practice authority with no collaborative agreement required. However, the transition is ongoing, and many NPs still work under the older framework.
- Georgia (restricted practice): An NP must practice under a nurse protocol agreement with a delegating physician. The agreement is filed with the state and specifies the medical acts the NP may perform, the drugs they can prescribe, and the circumstances requiring physician consultation. The physician is not required to be on-site but must be available for immediate consultation by phone or in person. Chart review requirements are not specified in law but are typically outlined in the protocol.1
These differences highlight just how much your daily work depends on a single contractual document. You can explore the full landscape in the AANP's state practice environment overview.
Cosmetic Collaboration and the Push for Full Practice Authority
In many settings, the collaborative agreement functions more as a legal formality than a genuine clinical safeguard. A physician signs off on charts they have never actually read, or nods to a protocol that was drafted years ago and never updated. This is often called "cosmetic collaboration." It satisfies the letter of the law but does little to improve patient safety, and it creates a false sense of oversight while costing NPs money and professional autonomy.
This gap between paper compliance and real clinical oversight fuels the advocacy for full practice authority (FPA). NPs argue that if the collaboration is not actually improving care, then the regulatory burden should be lifted so NPs can practice independently, as the evidence shows they are safe and effective primary care nurse practitioners. The movement toward FPA is driven not by a rejection of teamwork, but by the recognition that mandatory, often superficial agreements waste resources and restrict patient access to care.
How Scope of Practice Affects FNP Salary and Career Outlook
Nurse practitioner compensation varies significantly by state, and that variation invites a natural question: do states with full practice authority (FPA) tend to pay more? The picture is nuanced. Several of the highest paying states, including California and Oregon, do grant FPA, while others near the top, such as New Jersey and New York, maintain reduced or restricted authority. Cost of living, regional demand, and employer type all play major roles alongside scope of practice. Keep in mind that the Bureau of Labor Statistics figures below reflect all NPs (not only family nurse practitioners) and represent approximate 2024 data. Research published through the National Institutes of Health found that, on average, NPs in FPA states earned a mean hourly wage of roughly $52 during the study period, and were notably more likely to practice in health professional shortage areas (about 29%), which can translate into loan repayment incentives and hiring bonuses that effectively boost total compensation.
| State | Practice Authority (2026) | Median Annual Salary | Total NP Employment |
|---|---|---|---|
| California | Full | $166,610 | 20,980 |
| New Jersey | Restricted | $149,620 | 9,590 |
| Alaska | Full | $145,450 | 570 |
| New York | Reduced | $145,390 | 20,430 |
| Oregon | Full | $144,600 | 2,430 |
| Washington | Full | $140,220 | 4,790 |
| Connecticut | Full | $138,960 | 3,680 |
| Massachusetts | Reduced | $138,890 | 8,920 |
| New Mexico | Full | $138,440 | 1,870 |
| Arizona | Full | $133,790 | 7,540 |
| Montana | Full | $133,640 | 1,050 |
| New Hampshire | Full | $132,440 | 1,790 |
| District of Columbia | Full | $131,380 | 790 |
| Hawaii | Full | $130,940 | 470 |
| Rhode Island | Full | $130,710 | 1,200 |
NP Median Salary at a Glance
Where you land on the nurse practitioner salary curve depends on several factors, including your state's practice authority level, the clinical setting you work in, and your geographic region. Here is the national salary distribution for nurse practitioners based on the latest federal data.
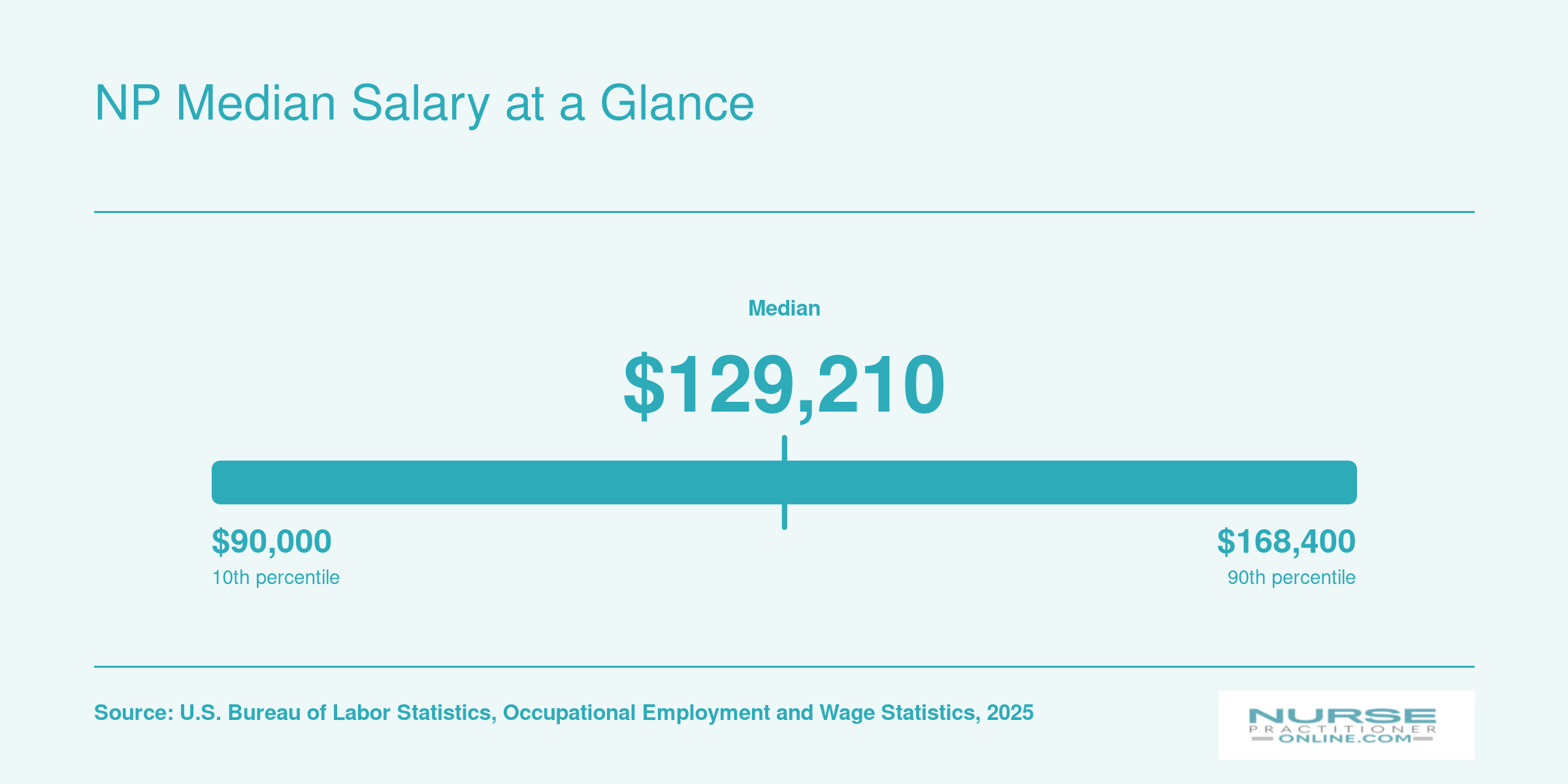
A peer-reviewed analysis found that full practice authority increases nurse practitioners' probability of self-employment by 374.1%, often leading to more independent primary care practices in rural and underserved communities and expanding healthcare access where it is needed most.
How to Factor Scope of Practice Into Your MSN-FNP Program Decision
Choosing an MSN-FNP program is a balancing act between reputation, cost, and flexibility, but the most consequential factor is often invisible in glossy brochures: where you intend to practice. The same degree that lets you diagnose and treat independently in one state can relegate you to a subordinate role in another. Before you enroll, let scope of practice drive your decision-making, not the other way around.
Start with Your Target State, Not a Program Brochure
Programs will emphasize accreditation and national exam pass rates, but your daily reality hinges on state practice authority. Look up the practice category (full, reduced, or restricted) for your intended state. Then work backward: if you plan to practice in a full practice authority state, you'll need robust preparation in independent clinical decision-making. In a restricted state, you'll need to understand collaborative agreement structures and how much supervision you can expect. Ask programs pointed questions: Do they help arrange preceptors in high-demand locales, or do they leave you to find your own? Do their clinical hours align with the patient populations and practice settings common in your region? A program with prestigious name recognition means little if its clinical placements don't translate to your job market.
Look Beyond Accreditation: State-Specific Licensure Requirements
CCNE- or ACEN-accredited MSN-FNP programs all prepare you for the same national certifications, AANP or ANCC. But licensing boards add their own layers. Some states require extra pharmacology hours, controlled substance certificates, or specific coursework in state health policy. Ask the program how their curriculum maps to the licensure requirements of your target state. Understanding the differences between ACEN vs CCNE accreditation can also help you evaluate whether a program's credentials will be recognized smoothly by your state board. If you're considering practicing in multiple states over your career, pick a program that builds a broad foundation and offers electives that address common state-level variations. The time to uncover a missing requirement is before you graduate, not when your application stalls at the board.
Seek Out Business and Regulatory Coursework
If you're eyeing a full-practice state with the goal of opening your own clinic, clinical competence is only half the picture. Look for programs that embed practice management, billing and coding, and regulatory navigation into the curriculum. Understanding how to credential with insurers, negotiate payer contracts, and comply with state business regulations can be the difference between a thriving practice and a struggling one. Programs that emphasize these skills signal that they're serious about preparing FNPs for entrepreneurial roles, not just for hospital employment.
Plan for Portability and Future Moves
An FNP credential is recognized in all 50 states, but the scope you can exercise changes at every state line. Even if you're rooted today, career or life changes may relocate you. Ask yourself: could I practice to the full extent of my training if I moved to a neighboring state? Look at recent legislative trends. States like Florida and Texas have expanded NP authority, while others remain restrictive. Factor this into your long-term strategy. A program that teaches you to navigate varying scopes, rather than assuming a single regulatory environment, will serve you for decades.
Frequently Asked Questions About NP Scope of Practice
Scope of practice questions come up at every stage of the NP journey, from choosing a program to negotiating your first job offer. Below are answers to the questions nurses ask most often, with specifics grounded in the 2026 regulatory landscape.
- What is the scope of practice for nurse practitioners?
- NP scope of practice defines the clinical activities a nurse practitioner is legally authorized to perform, including assessment, diagnosis, ordering and interpreting tests, prescribing medications, and managing treatment plans. The exact boundaries vary by state law, national certification, and the NP's population focus. Some states allow NPs to practice independently, while others require a formal relationship with a collaborating physician.
- Which states have full practice authority for nurse practitioners in 2026?
- As of 2026, more than half of U.S. states plus the District of Columbia grant full practice authority, allowing NPs to evaluate patients, diagnose conditions, and prescribe treatments without physician oversight. States that recently transitioned or are phasing in full practice authority continue to expand that count. You can check your specific state's status through your state board of nursing or the AANP's regularly updated practice environment map.
- What does a collaborative agreement require for nurse practitioners?
- A collaborative agreement is a formal arrangement between an NP and a physician that outlines the scope of clinical services the NP may provide, prescriptive authority details, and protocols for physician consultation or chart review. Requirements differ by state: some mandate a specific physician to patient ratio, regular in-person meetings, or proximity limits. In reduced and restricted practice states, NPs cannot practice without this agreement in place.
- How does NP scope of practice differ from physician assistant scope of practice?
- NPs practice under state nursing board regulations and can gain independent practice authority in full practice states. PAs are regulated by medical boards and, in most states, must maintain a formal supervisory or collaborative relationship with a physician. NPs choose a population focus during education (such as family or adult gerontology), while PA training follows a generalist medical model. These structural differences shape where and how each provider practices.
- How is NP scope of practice changing in 2026?
- Several states are advancing bills to remove or reduce collaborative agreement requirements, continuing a trend accelerated by pandemic era emergency orders. Federal agencies, including the VA health system, have already granted NPs full practice authority regardless of state law. Professional organizations and bipartisan coalitions are pushing for broader independent practice, making 2026 an active year for scope of practice legislation across the country.
- What can a family nurse practitioner do that a registered nurse cannot?
- A family nurse practitioner can independently or semi-independently diagnose conditions, order and interpret diagnostic tests, prescribe medications (including controlled substances in most states), develop treatment plans, and manage chronic diseases across the lifespan. Registered nurses carry out physician or NP orders but are not authorized to diagnose or prescribe. Earning an MSN or DNP with an FNP focus is what unlocks this expanded clinical authority.
- Does scope of practice affect NP malpractice insurance rates?
- Yes. NPs in full practice authority states often carry higher individual liability because they practice without a supervising physician. That said, premiums for NP malpractice insurance remain significantly lower than physician rates. The exact cost depends on your specialty, state, and clinical setting. Many employers cover malpractice insurance, but understanding how scope of practice shapes your liability exposure is an important part of career planning.
Practicing in a full authority state vs. a restricted one is not just a lifestyle preference: it shapes what you can do on day one, how much you earn, and whether you can eventually hang your own shingle. The same MSN-FNP credential opens an independent clinic in New Mexico and requires years of physician supervision in California.
Before you commit to a program or a job offer, look up your target state's current practice authority classification and any pending legislation that could change it. With roughly half of states plus D.C. already granting full practice authority and more bills moving each session, the trend favors FNPs who plan ahead. Whether you are just beginning to explore how to become a nurse practitioner or are already comparing programs, build your career around where scope is heading, not just where it stands today.