Most important takeaways…
- Healthcare workers face 72.8% of all nonfatal workplace violence injuries, making de-escalation a critical NP skill.
- Tailoring your communication strategy to the specific behavior pattern (angry, anxious, manipulative, non-adherent) produces better outcomes than a generic approach.
- Objective, contemporaneous documentation of difficult encounters is your strongest legal safeguard against complaints and liability.
- When dismissing a patient, you must provide written notice and a 30-day transition period to avoid abandonment claims.
Nearly three out of four nonfatal workplace violence injuries in the United States occur in healthcare and social assistance settings, making clinics and hospitals statistically more dangerous than construction sites or law enforcement offices. For nurse practitioners managing their own patient panels, dealing with difficult patients is not an occasional disruption. It is a recurring, high-stakes clinical skill that directly affects outcomes, liability exposure, and personal well-being.
The tension is real: NP programs devote hundreds of hours to pharmacology, diagnostics, and pathophysiology, yet formal training in conflict management in healthcare often amounts to a single lecture or elective rotation. That gap between clinical preparation and daily reality means most practitioners build their approach to difficult patient encounters through trial and error, absorbing lessons that carry professional and emotional costs.
Why Some Patient Encounters Feel 'Difficult', and Why the Label Matters
Some encounters leave you energized, feeling like you made a real difference. Others drain you, trigger your sympathetic nervous system, or keep you awake at night replaying what you could have done differently. The distinction between a routine visit and a difficult one often hinges on factors far beyond the patient's diagnosis.
What Makes an Encounter 'Difficult'?
Healthcare settings define difficult encounters in various ways, but most share common threads: patients or family members who exhibit verbal aggression, refuse recommended treatment without engaging in shared decision-making, make unrealistic demands, violate boundaries, or display manipulative behaviors. Bureau of Labor Statistics data on nonfatal occupational injuries consistently shows that healthcare workers face some of the highest rates of workplace violence across all industries, with verbal threats and physical assaults occurring far more frequently in clinical settings than in most other professional environments. The American Nurses Association has published position statements and reports on workplace violence that underscore the prevalence of these encounters, noting that a significant percentage of nurses and nurse practitioners experience some form of hostility or aggression during their careers.
Yet the term "difficult patient" carries clinical and ethical weight. Research published in nursing management and clinical care journals suggests that labeling a patient as difficult can create a self-fulfilling prophecy, subtly shifting how clinicians approach care, document findings, and allocate time. When a chart note flags someone as difficult, subsequent providers may enter the room with heightened defensiveness, shortened patience, or unconscious bias, all of which can degrade therapeutic rapport and outcomes.
The Impact of Language on Care Quality
The Joint Commission's sentinel event database and Quick Safety newsletters have documented cases where poor communication and unaddressed escalation contributed to adverse events, including medical errors and patient harm. When we label the person rather than the behavior, we risk overlooking the root cause: uncontrolled pain, fear, cognitive impairment, cultural misunderstanding, or a history of trauma. A patient who appears manipulative may be using the only coping strategy they know to manage overwhelming anxiety. A family member who seems confrontational may be grieving or advocating fiercely because they feel unheard. These dynamics underscore why nurse practitioner advancement opportunities should include communication and de-escalation training, not just clinical skill-building.
Reframing the Conversation
Instead of asking "How do I deal with this difficult patient?", consider "What is driving this behavior, and how can I respond in a way that preserves safety, dignity, and therapeutic alliance?" That subtle shift in framing opens the door to evidence-based de-escalation, trauma-informed care, and documentation practices that protect both you and the patient. It also acknowledges a hard truth: some encounters are objectively unsafe, and recognizing that reality is not a failure of empathy but a necessary act of professional self-preservation.
Recognizing the Warning Signs of Escalation
The earlier you spot escalation, the more options you have to redirect it.
Most confrontations in clinical settings do not erupt without warning. They follow a predictable arc, and learning to read the early signals gives you time to intervene before a tense moment becomes a dangerous one.
The Escalation Continuum
Think of difficult encounters as moving along a continuum rather than flipping a switch. A patient typically moves through stages: anxiety first, then defensiveness, then verbal aggression, and finally a physical threat. Each stage is its own window for intervention. A patient who is simply anxious and pacing can often be redirected with a calm, unhurried greeting. A patient already using profanity requires a different response entirely. Knowing where someone sits on that continuum shapes every decision you make next.
Behavioral Cues to Watch
Your eyes and ears are your earliest warning system. Watch for:
- Posture and movement: clenched fists, crossed arms held tight, pacing, or a sudden stillness that feels charged
- Proxemics: moving closer than the situation calls for, crowding your space, or positioning between you and the exit
- Voice and speech: a raised or unnaturally flat voice, rapid-fire speech, repeated demands, or a shift into profanity
- Eye contact: a fixed, unblinking stare or the opposite, eyes darting and scanning the room
None of these cues is definitive on its own. Read them in clusters and in context.
Environmental Risk Factors
The room itself can accelerate escalation. Overcrowded waiting areas, long delays without explanation, lack of privacy during sensitive conversations, and cluttered exam rooms with heavy objects within reach all raise the baseline risk. When you walk into an environment with several of these factors stacked together, treat your alertness level accordingly.
Telehealth-Specific Signals
Virtual visits remove body language from the equation, which means you have to work harder with the cues that remain. An abrupt threat to disconnect, hostile messages typed into a chat window, a sudden shift in tone with no obvious trigger, or a voice that tightens and clips short sentences all warrant the same attentiveness you would give a behavioral cue in person. The platform is different; the escalation continuum is not. NPs who are considering a transition into psychiatric care, where de-escalation skills are especially critical, may find it helpful to explore how to transition from FNP to PMHNP.
Healthcare and social assistance workers account for 72.8% of all nonfatal workplace violence injuries in the U.S., according to the American Association of Critical-Care Nurses. That makes healthcare more dangerous than any other industry when it comes to on-the-job violence.
De-Escalation Techniques Every NP Should Know
The Crisis Prevention Institute's Verbal Intervention model operationalizes the American Nurses Association and American Association of Critical-Care Nurses standards for de-escalation at the bedside, providing nurse practitioners with a structured framework to defuse tension before it escalates into aggression.1 De-escalation is not an instinctive skill for most clinicians. It requires deliberate training, repeated practice, and familiarity with evidence-based techniques that have been shown to improve staff confidence, reduce the use of restraints, and lower the incidence of aggressive incidents in healthcare settings.2
Evidence-Based De-Escalation Frameworks
Two widely adopted frameworks guide nurse practitioner de-escalation training. The CPI Crisis Development Model describes four behavior levels: anxiety, defensive, risk behavior, and tension-reduction.1 CPI's Verbal Intervention principles include remaining calm, isolating the individual when safe to do so, watching body language, keeping communication simple, using reflective questioning, deploying strategic silence, and monitoring your own paraverbals (tone, volume, cadence).2 When verbal techniques alone are insufficient, CPI's limit-setting algorithm provides a stepwise approach: explain which behavior is inappropriate, explain why it matters, offer reasonable choices with clear consequences, allow time for the individual to decide, and enforce consequences consistently if the behavior persists.2
The STAMP framework offers a complementary early-warning tool. STAMP stands for Staring, Tone (of voice), Anxiety (visible signs), Mumbling, and Pacing. Research shows these behaviors are significantly associated with subsequent aggression, and training clinicians to recognize STAMP components prompts earlier intervention, often before the patient or family member reaches the defensive or risk-behavior stages.1
Concrete Verbal Scripts for Common Scenarios
- Angry patient demanding a specific medication: "I hear that you're frustrated, and I want to help you feel better. Let's talk about what's going on with your pain right now. I'm not able to prescribe that medication because [clinical reason], but I have two other options that may work well for you. Which would you like to discuss first?"
- Family member yelling about perceived neglect: "I can see you're upset, and I understand you're worried about your mom. I want to make sure we address your concerns. Can we step over here so I can explain what we've done and what comes next? I have her chart right here."
- Patient refusing recommended treatment: "It sounds like you have some concerns about this treatment. Can you tell me what's worrying you most? I want to make sure you have all the information you need to make the decision that's right for you."
Non-Verbal De-Escalation Techniques
Your body language often speaks louder than your words. Maintain an open posture: avoid crossing your arms, pointing, or standing directly in front of a patient in a way that feels confrontational. Position yourself at a 45-degree angle when possible, respect personal space (at least an arm's length), and lower your own voice volume and pace as tension rises. These non-verbal cues signal safety, respect, and a willingness to listen. Certain nurse practitioner tools can also help you log behavioral observations in real time, supporting better documentation of de-escalation efforts.
Telehealth Adaptation: De-Escalating Without Physical Presence
De-escalation over video or phone requires intentional modulation of tone and strategic use of pauses. Slow your speech, lower your pitch slightly, and pause after the patient speaks to signal that you are listening rather than rushing to counter their concerns. If a patient becomes agitated, name the emotion you observe ("I can hear that you're really frustrated right now") and offer a choice: "Would it help to take a five-minute break and come back to this? I want to make sure we have the best conversation possible." Offering to reschedule when emotions are high is not avoidance; it is boundary-setting that protects both parties and increases the likelihood of a productive follow-up encounter.
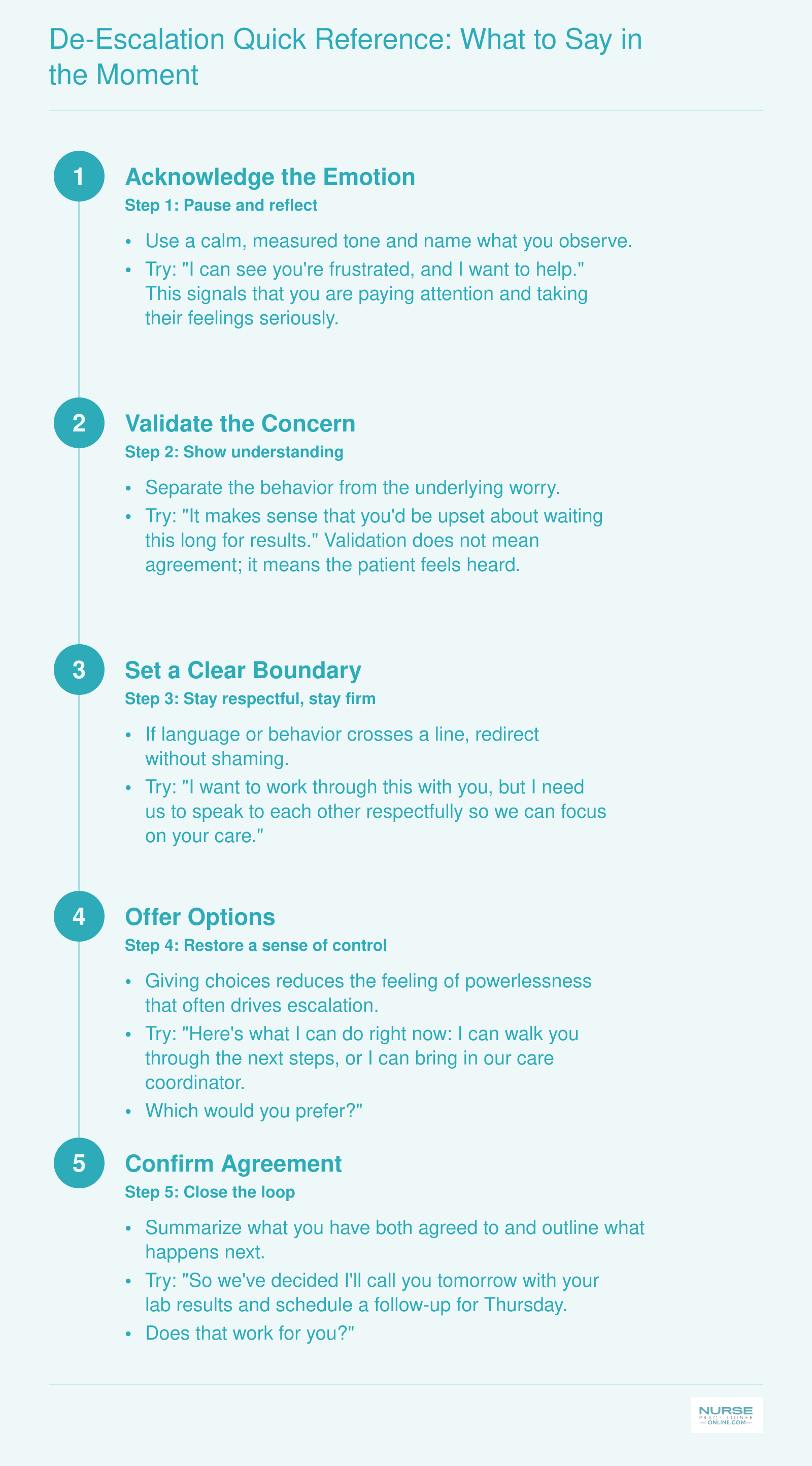
De-Escalation Quick Reference: What to Say in the Moment
Keep this five-step sequence handy on your phone or posted in your workstation. When a patient or family member begins to escalate, moving through these steps in order can help you regain a productive conversation quickly.
Strategies by Behavior Type: Angry, Manipulative, Non-Adherent, and Anxious Patients
Not every difficult encounter calls for the same playbook. Recognizing the pattern behind a patient's behavior lets you select a communication strategy that actually fits the situation, rather than defaulting to a one-size-fits-all response that may escalate things further. Below are four common behavior types you will encounter in NP practice, along with practical approaches, sample language, and the pitfalls that trip up even experienced clinicians.
Angry or Hostile Patients
These patients may yell, use abusive language, or make threats.1 Your first priority is always safety: position yourself near the door, keep your body language open, and avoid crossing your arms.
Once you have assessed that the situation is safe to continue, validate the emotion before redirecting the conversation. A phrase like "I can see you're very angry about what's been happening" signals that you hear them without agreeing to unreasonable demands. Keep your voice calm and your statements concrete. The biggest pitfall here is arguing, lecturing, or trying to prove the patient wrong. That almost always fans the flames.1
Manipulative or Splitting Patients
Splitting behavior looks like idealizing one clinician as "the only good one" while devaluing the rest of the team. These patients may pit staff members against each other, sometimes without anyone realizing it until the damage is done.1
The antidote is team consistency. When the entire care team communicates with one voice, there is little room for triangulation. Stay neutral and avoid power struggles. You might say, "It sounds like you've had different experiences with different staff. I'm not able to speak for them, but I can explain our team's plan with you." Never take sides or criticize a colleague, even if the patient's complaint sounds legitimate. Address concerns through proper channels later. In settings like hospice nurse partnerships, where emotions run especially high, this kind of unified messaging is even more critical.
Non-Adherent or Resistant Patients
Repeatedly missed medications, declined tests, and pushback on recommendations are frustrating, but resistance is rarely simple defiance. It often signals fear, misunderstanding, financial barriers, or competing priorities.2
Instead of repeating instructions more firmly, get curious. Motivational interviewing techniques work well here. Try asking, "Many people find it hard to take a new medication every day. What gets in the way for you?" That question respects autonomy, checks comprehension, and opens a door to problem-solving. The trap to watch for is shaming, blaming, or moralizing. Phrases like "You really should know better" shut down dialogue instantly.2
Anxious or Fearful Patients
High anxiety can present as rapid-fire questions, tearfulness, refusal of procedures, or even anger that masks deeper fear. These patients need you to slow down and provide clear, digestible information.1
Start by naming the emotion: "What's worrying you the most right now?" Then offer reassurance grounded in specifics rather than vague platitudes. Explain what will happen step by step, and give the patient as much control as possible (choosing which arm for a blood draw, for example). The most common mistake is minimizing or dismissing the anxiety with phrases like "There's nothing to worry about." To the patient, the worry is very real, and brushing it off erodes trust.
Pulling It All Together
No matter which behavior type you are facing, a few principles apply across the board:
- Pause before reacting: A few seconds of silence can prevent an impulsive response you will regret.
- Label the behavior, not the person: Thinking of a patient as "expressing anger" rather than "being a difficult patient" keeps your empathy intact.
- Debrief with colleagues: Talking through a tough encounter helps you refine your approach and protects your well-being.
With practice, matching your approach to the behavior pattern in front of you becomes second nature, turning encounters that once felt impossible into moments of genuine clinical skill.
Questions to Ask Yourself
Navigating Difficult Family Conversations
Family dynamics shift the challenge from managing one patient relationship to orchestrating multiple stakeholders with competing emotional, cultural, and legal interests. You are simultaneously clinician, mediator, educator, and advocate, often for parties whose goals do not align. Research from 2024 shows that nearly 40% of nurse practitioners report weekly conflict between patient preferences and family demands, yet few graduate programs offer structured training in family facilitation beyond basic communication skills.
When Surrogates Disagree with the Patient's Wishes
A healthcare power of attorney grants legal authority, not moral license to override known patient preferences. If a surrogate disagrees with documented advance directives or clearly stated wishes, your role is to reorient the conversation toward the patient's voice. Start by asking, "Can you help me understand what your mother told you she wanted in this situation?" or "Your brother filled out these forms last year. Do you recall what was important to him when he made these choices?" Document the patient's prior statements in the chart and share them with the surrogate in writing. If disagreement persists, involve your institution's ethics committee early. You are the patient's advocate first, and that includes protecting their autonomy even when they can no longer speak for themselves.
Structuring a Family Meeting When Conflict Runs High
When family members disagree about a care plan, a structured family conference often prevents escalation. Invite all decision-makers (or use a conference line), the bedside nurse, a social worker, and, if prognosis or goals are contested, a palliative care nurse practitioner or ethics consultant. Set ground rules at the start: one person speaks at a time, the patient's values guide decisions, and the goal is consensus, not debate. Open with, "We're here to make sure we're all hearing the same information and honoring what matters most to [patient's name]." Present the medical facts without jargon, then ask each family member, "What do you understand about where things stand?" and "What would your dad say if he could tell us what he wants now?" When voices rise, pause and name it: "I hear frustration. Let's take a breath and come back to what [patient] told us."
Cultural and Language Considerations
Cultural norms shape how families discuss illness, prognosis, and end-of-life decisions. In some cultures, direct disclosure of a terminal diagnosis to the patient is considered harmful; in others, collective family decision-making supersedes individual autonomy. When language barriers exist, always use a professional medical interpreter, not a family member. Family interpreters filter information, withhold bad news, or inject their own opinions. A professional interpreter translates your words and the family's responses without editorial interference. Ask about cultural expectations early: "Are there customs or beliefs I should understand as we talk about your wife's illness?" Adjust your approach while maintaining medical and ethical standards.
Verbal Scripts for Common Family Scenarios
Explaining a poor prognosis: "I wish I had better news. The tests show that the cancer has spread to her liver and lungs. With treatment, we're looking at months, not years. I know this isn't what you were hoping to hear. What questions do you have right now?"
Responding to 'do everything possible': "I hear that you want us to do everything we can. Can you tell me more about what 'everything' means to you? Sometimes families mean 'everything that helps him live comfortably and spend time with loved ones,' and sometimes they mean 'every machine and medication even if it prolongs suffering.' Help me understand what your dad would want."
Addressing a family member who undermines the plan: "I notice you've been telling your mom not to take her blood pressure medication because you're worried about side effects. I understand your concern, and I want to make sure we're all on the same page so she gets the best outcome. Can we talk through your questions together so you feel confident in the plan?"
How to Document Difficult Patient Encounters
A thorough, objective chart note is your strongest legal safeguard after a difficult patient encounter. Documentation protects both you and the patient by creating a contemporaneous record of exactly what happened, what you did, and why. Every note you write is a legal document that can be reviewed years later, so it must be factual, accurate, complete, and timely, principles often remembered as FACT.1
Why Documentation Matters
When a complaint, lawsuit, or regulatory inquiry arises, the clinical record is often the first and most critical piece of evidence. Risk-management experts emphasize that a well-documented note can mean the difference between a dismissed claim and a costly settlement.1 It demonstrates your clinical reasoning, communication efforts, and adherence to standards of care. Remember: if it is not documented, it did not happen in the eyes of the law.
What to Include in Your Note
Your note should capture the encounter in a structured format. SOAP, SBAR, or a chronological narrative all work. Be sure to document the following elements:
- Context: Why the patient was there and any relevant background.
- Objective behavior: Record specific actions and verbatim quotes. For example, "Patient shouted, 'I'm not doing that test!' and slammed the table."
- Your assessment: Note the patient's emotional state, capacity, and any barriers to care. Use neutral language: "Patient appeared frustrated and raised her voice during discussion of the plan."
- Interventions attempted: Describe what you did to de-escalate, educate, or negotiate. "I acknowledged the patient's frustration and offered a break before continuing."
- Communication: Log calls to the supervising physician, referrals, or notifications to family. Include times and responses.
- Refusal details: If the patient declined care, document that you provided information, assessed their understanding, and evaluated decision-making capacity. Note whether a signed refusal form was obtained.
- Follow-up plan: Outline next steps, safety instructions, and any agreed-upon modifications.
- Witnesses: Record the names of staff members who were present or involved.
- Timing: Date and time each entry. If you are charting late, label it as a "late entry" and include the actual time of the note.1
Objective vs. Subjective Language
Never label a patient as "difficult," "abusive," or "drug-seeking" in the chart. Such terms are subjective and can appear judgmental, undermining your credibility.1 Instead, describe observable behaviors and use neutral phrasing. For instance, write "Patient repeatedly interrupted and used profanity, stating, 'This is a waste of my time'" rather than "Patient was aggressive and rude."
Replace words like "noncompliant" with "patient declined to take prescribed medication after discussion of risks." Swap "claims" for "reports," and "refused to cooperate" for "declined." Avoid absolutes like "always" or "never." The goal is to paint a factual picture that a third reader could clearly interpret.
When to File an Incident Report
Routine charting is not a substitute for an incident report when a safety event occurs. File a formal incident report for any situation involving actual harm, a near miss, elopement, threats, physical assault, or medication and treatment errors. Do not mention the incident report in the medical record; it is a separate risk-management tool.1 The chart note should contain only clinical facts, while the incident report captures the safety analysis.
Nurse practitioners in high-acuity settings, such as emergency nurse practitioners, often face these scenarios regularly and benefit from having documentation templates ready before a crisis unfolds. By approaching difficult encounters with documentation that is thorough, objective, and timely, you protect your license and your patients while ensuring continuity of care.
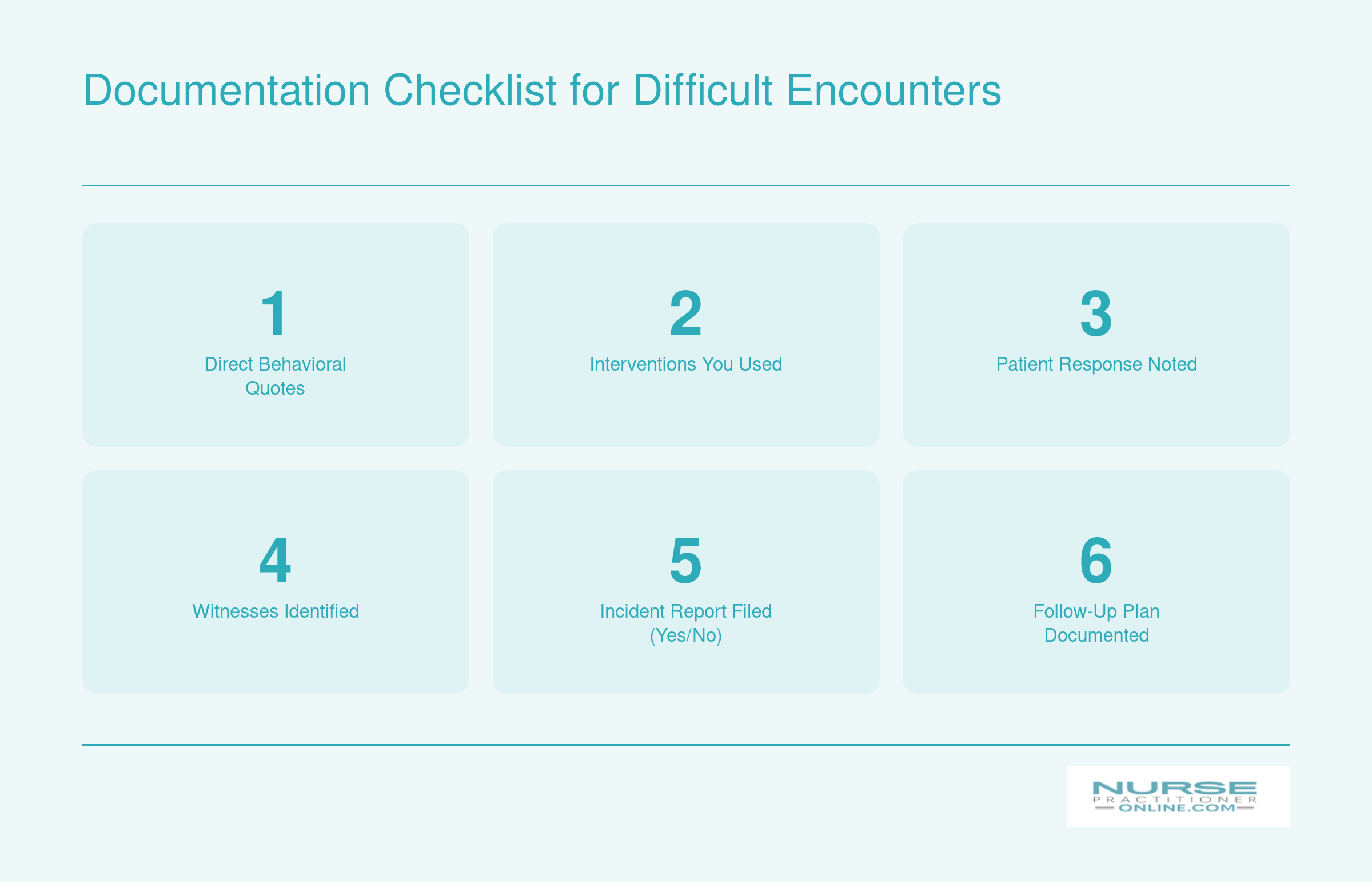
Documentation Checklist for Difficult Encounters
After a difficult patient or family encounter, thorough documentation protects you, your practice, and the patient. Keep this quick-reference checklist nearby so you capture every essential element while the details are still fresh.
Protecting Yourself: Safety, Legal Considerations, and When to Dismiss a Patient
Federal EMTALA rules require any hospital emergency department to evaluate and stabilize a patient regardless of whether you have formally ended the treatment relationship.1 That single fact frames everything else in this section: dismissing a patient from your panel is not the same as walking away from your duty of care, and the legal guardrails are real.
Personal Safety First
Before you get to the paperwork, get to the room. Your physical safety is the non-negotiable starting point.
- Position yourself near the exit: Never let an agitated patient stand between you and the door. Arrange seating so you have a clear path out.
- Use a buddy system: For patients with a known history of volatility, do not room alone. Bring a medical assistant, colleague, or security officer into the visit.
- Involve security early: If a patient is escalating, call security before the situation crosses a line, not after. Most workplace violence prevention policies are explicit that staff should not wait until they feel actively threatened.
- Know your facility's policy: Every practice setting should have a written workplace violence prevention plan. Read it before you need it.
Behavior Agreements
For patients who can be retained but whose conduct is straining the relationship (repeated no-shows, controlled-substance concerns, verbal aggression toward staff), a written behavior agreement can reset expectations. These documents typically spell out specific conduct requirements, the consequences for breaching them, and the patient's acknowledgment in writing. They are useful as a clear, documented warning, but they are not magic. A behavior contract does not waive the patient's rights, and it does not, on its own, protect you legally if you later dismiss without following proper termination procedures.2
The Formal Dismissal Process
If the relationship truly cannot continue, follow the standard protocol:
- Provide written notice: Most guidance points to a 30-day notice period as the national norm, during which you remain responsible for urgent and emergent care.2
- Send a certified termination letter: Include the effective end date, a clear statement that you will provide urgent care during the transition window, instructions for requesting medical records, and a neutral recommendation for finding a new provider. Keep the explanation factual and non-inflammatory.1
- Document the rationale in the chart: Note the reason for termination in objective terms. This is your record if the decision is later questioned.2
- Check your state and contract obligations: Rules vary. Florida statute 458.348, for example, addresses notice requirements specific to NP practice relationships.3 Your state nursing board, medical board, malpractice carrier, and payer contracts may each impose additional requirements.
Legal and Ethical Guardrails
Patient abandonment, defined as ending care without adequate notice or a reasonable opportunity for the patient to find another clinician, can trigger administrative penalties against your license.2 Equally important: you cannot dismiss a patient for discriminatory reasons. Race, religion, disability, pregnancy status, sexual orientation, and other protected characteristics are off the table as grounds for termination.2 NPs who serve as primary care nurse practitioners carry an added responsibility to ensure continuity during the transition, since patients may have limited alternatives. And regardless of whether you have ended the office relationship, EMTALA obligations and your general duty to treat in emergencies remain in force.1 When in doubt, call your malpractice carrier before sending the letter. That phone call is what the policy is for.
Managing Your Own Well-Being After Tough Encounters
What should you do immediately after a patient encounter leaves you shaken, angry, or emotionally drained?
Difficult patient encounters trigger genuine physiological stress responses. Your body doesn't distinguish between a verbal threat in an exam room and a physical danger: both activate fight-or-flight systems that flood your bloodstream with cortisol and adrenaline. A single tense conversation may resolve quickly, but cumulative exposure to challenging interactions contributes to burnout, compassion fatigue, and what researchers now call moral injury (the psychological distress that comes from being unable to provide the care you believe patients deserve, often due to system constraints). Acknowledging this emotional toll isn't a sign of weakness. It's a prerequisite for sustainable practice.
The Power of Structured Debriefing
Many NPs leave a difficult encounter and immediately move to the next patient, burying the emotional residue. Structured debriefing interrupts that cycle and turns raw experience into learning.
- Hot debrief: Within minutes of the encounter, take five minutes with a trusted colleague. Name what happened, how you felt, and what immediate support you need. This isn't full analysis; it's emotional triage. A brief peer check-in helps discharge the acute stress response and prevents rumination during the rest of your shift.
- Cold debrief: Within 48 hours, sit down (alone or with your team) and ask three questions: What went well? What would I change next time? What system issues made this harder than it needed to be? Cold debriefs build pattern recognition and surface opportunities for institutional change.
Building Long-Term Resilience
No single strategy inoculates you against the cumulative weight of difficult work, but a combination helps:
- Peer support groups: Regular meetings with fellow NPs who understand the unique stressors of the role normalize your experiences and reduce isolation.
- Employee assistance programs (EAPs): Most employers offer confidential counseling. Use it early, not just in crisis.
- Mindfulness and stress-reduction practices: Even brief daily practices (five-minute breathing exercises, body scans, or short walks) help regulate your nervous system between encounters.
- Professional help: If you notice persistent nightmares, hypervigilance, cynicism, or dread about going to work, consult a mental health provider familiar with healthcare professionals. These are signs of secondary traumatic stress, not personal failure.
Advocate for Systemic Change
Individual resilience strategies matter, but they shouldn't be the only line of defense. Many difficult encounters are more frequent or more intense because of broken systems: inadequate staffing, lack of security presence, poor scheduling that rushes complex conversations, or cultures that tolerate patient aggression as "part of the job." If you're looking for concrete ways to shape policy at the organizational or legislative level, the nurse practitioner health policy toolkit offers a practical starting point.
Advocate within your organization for:
- Mandatory debriefing protocols after code-gray (behavioral emergency) events
- Zero-tolerance policies for violence or threats, with clear enforcement
- Staffing ratios and schedules that allow time for complex behavioral health needs
- Environmental design changes (panic buttons, safe exit routes, visibility from hallways)
When you push for these changes, you protect not only yourself but every colleague and patient who comes after you.
Common Questions About Handling Difficult Patient Encounters
Below are answers to some of the most common questions nurse practitioners ask about managing challenging interactions. Each response offers a brief overview, and you can find more detailed strategies in the corresponding sections of this guide.
- How do you deal with a difficult patient as a nurse practitioner?
- Start by pausing your own emotional reaction, then use active listening and empathic reflection to understand the patient's perspective. Offer limited choices so the patient feels some control over the encounter. Avoid labeling the person as 'difficult' and instead focus on the specific behavior that needs to be addressed. The section on why the label matters explores this mindset shift in depth.
- What are the best de-escalation techniques for healthcare professionals?
- Evidence-based frameworks such as LOWLINE (Listen, Offer, Wait, Look, Incline, Nod, Express) give you a structured approach. Key tactics include lowering your vocal tone, slowing your speech, paraphrasing the patient's concerns, and maintaining soft eye contact. Naming the emotion you observe ('I can see this is frustrating') often diffuses tension quickly. See the de-escalation techniques section for a full breakdown.
- How do you handle difficult family members in a healthcare setting?
- Acknowledge the family member's fear or frustration before redirecting the conversation. Set clear ground rules early: who the primary decision-maker is, when updates will happen, and what behavior is expected. Providing a structured communication plan often reduces anxiety-driven conflict. The section on navigating difficult family conversations walks through scenario-specific strategies.
- How should you document a difficult patient encounter?
- Record specific, observable behaviors using direct quotes rather than subjective labels. Include your risk assessment, the interventions you attempted, and the patient's response. For telehealth visits, also note the modality (video or phone), the platform used, and any technical problems that affected the encounter. The documentation checklist in this guide provides a step-by-step reference.
- When can a nurse practitioner dismiss a patient from their practice?
- Dismissal is generally appropriate when there is persistent abusive behavior, an irreparable breakdown in the therapeutic relationship, or an inability to provide safe care. You must follow your state's regulations and provide written notice with a reasonable transition period to avoid a claim of patient abandonment. The section on safety and legal considerations covers the specific criteria and process.
- How do you distinguish a 'difficult' patient from one experiencing pain or delirium?
- Always screen for reversible medical causes first. Agitation, confusion, or hostility can signal uncontrolled pain, delirium, hypoxia, or medication side effects. A brief cognitive and pain assessment before labeling behavior as intentional helps you intervene appropriately. The section on why some encounters feel difficult discusses how to separate clinical causes from behavioral ones.
- How do you handle a difficult patient encounter during a telehealth visit?
- Telehealth reduces your access to nonverbal cues, and technical issues like audio lag or disconnections can fuel a patient's frustration. Confirm the patient's identity and location at the start, set expectations around time and behavior, and optimize your own setup with good lighting and a neutral background. Watch for early agitation signs such as raised voice, rapid speech, or repeated demands. If abusive language persists after you name the behavior and set a limit, you may end the visit and document accordingly.