Most important takeaways…
- Mississippi, Alabama, Texas, Missouri, and Arizona rank as the five states with the greatest unmet need for nurse practitioners in 2026.
- Over 137 million Americans live in designated mental health shortage areas, driving intense demand for psychiatric NPs nationwide.
- NP employment is projected to grow 40.1% from 2024 to 2034, roughly ten times the average for all occupations.
- States with restricted scope of practice laws account for a disproportionate share of primary care shortage areas.
More than 85 million Americans live in federally designated primary care Health Professional Shortage Areas, and the ratio of nurse practitioners to patients in the hardest-hit states is less than half the national average. The gap is not closing on its own. Schools are graduating more NPs each year, but enrollment remains concentrated in states that already have the strongest supply, while communities with the deepest shortages struggle to attract and retain providers.
This article identifies the five states where the gap between NP supply and patient demand is widest, measured by per-capita ratios, HPSA designations, and projected workforce growth. It also examines the psychiatric mental health NP shortage, how scope-of-practice laws amplify or mitigate demand, and what working in a high-need state means for salary, autonomy, and career trajectory. You can compare compensation across the profession in our highest paid nurse practitioner specialties breakdown.
For nurses considering NP school, understanding where the shortage is most acute is not just a labor-market question. It shapes licensure strategy, specialization choice, and whether relocation becomes a practical necessity or a career advantage.
How We Measured NP Need: Methodology
Five Criteria for Ranking NP Shortages
To identify the states with the greatest unmet need for nurse practitioners, we evaluated each state across five weighted criteria:
- NP-to-population ratio: We calculated the number of actively practicing NPs per 100,000 residents, using the most recent workforce data. A lower ratio signals a thinner provider base relative to the population served.
- HPSA primary care shortage designations: We tallied all primary care Health Professional Shortage Area (HPSA) designations per state. HRSA defines an HPSA as an area with a population-to-primary-care-physician ratio of at least 3,500:1 (or 3,000:1 in high-need areas).1 Because NPs increasingly fill primary care gaps, a high concentration of HPSA designations points to communities that would benefit most from expanded NP services. Nationally, there are 8,467 primary care HPSA designations covering more than 92 million residents, and only 48.18% of the need is currently being met.2
- Rural population without nearby NP: We incorporated the percentage of each state's rural population living more than a 30-minute drive from an NP practice. This measures geographic access, a critical dimension of shortage often missed by headcount ratios alone.
- Projected job growth: We factored in state-level BLS projections for NP employment growth through 2034, capturing the expected increase in demand beyond current staffing levels.
- Scope-of-practice restrictiveness: States with full practice authority enable NPs to practice to the top of their license, reducing barriers to care in underserved areas. We included a restrictiveness index as a modifier, because even where need is high, regulatory hurdles can prevent NPs from fully addressing that need.
Data Sources and Their Limits
All criteria relied on the most recent publicly available data, not current-year snapshots. NP workforce counts came from the Bureau of Labor Statistics' 2024 employment estimates, which place the national primary care NP count at 374,970.3 HPSA designations and population figures reflect HRSA data as of December 31, 2025.2 State workforce projections draw from the same BLS release cycle. It is important to note that HPSA designations are based on physician shortages; they do not directly count NP openings. However, because NPs provide a growing share of primary care, especially in shortage areas, the HPSA framework remains the strongest proxy for where additional NP services are most urgently needed.
Why Per-Capita Need Outperforms Job Listings
Many published rankings rely on raw counts of online job postings or median salary data. While useful, those metrics can be distorted by high turnover, seasonal hiring, or a concentration of travel-contract positions. A state may have many postings yet still suffer from a maldistribution of providers. Our per-capita approach, anchored to population ratios, designated shortage areas, and geographic access, reveals the chronic, structural undersupply that hiring ads alone cannot capture. It better reflects the experience of residents in rural counties or inner-city communities who wait months for an appointment, even when job boards look busy.
What This Ranking Doesn't Capture
No single composite index can cover every facet of a nursing shortage. NP-to-population ratios do not reveal specialty-specific gaps; a state may have adequate primary care NPs but critically low numbers of psychiatric or pediatric NPs. Telehealth expansion has also changed access patterns, and our rural-access metric may undercount patients who now receive care virtually. Finally, scope-of-practice laws continue to evolve, so the restrictiveness factor represents a snapshot that can shift with new legislation. Our ranking should be viewed as a practical, multi-signal starting point, not a substitute for on-the-ground workforce planning.
The 5 States With the Greatest Unmet Need for Nurse Practitioners
The table below ranks five states where the gap between available primary care providers and community need is most severe, based on federal Health Professional Shortage Area (HPSA) data compiled by KFF. These figures reflect designated shortage areas and the estimated number of additional practitioners required to close each state's gap. Because scope of practice laws, rural geography, and population demographics all play a role, the raw numbers only tell part of the story. We explore each state's unique challenges in the sections that follow.
| State | HPSA Designations | Population in Shortage Areas | Percent of Need Currently Met | Additional Practitioners Needed |
|---|---|---|---|---|
| Georgia | 233 | 2,720,812 | 39.0% | 563 |
| Missouri | 344 | 1,837,226 | 21.5% | 475 |
| Mississippi | 159 | 1,353,860 | 34.9% | 303 |
| Alabama | 124 | 2,251,179 | 67.0% | 239 |
| Arkansas | 152 | 1,123,775 | 53.5% | 177 |
A Closer Look: What Makes Each State's Shortage Unique
Not every NP shortage looks the same. The tension running through all five of these states is that high need does not automatically translate into high opportunity unless the regulatory environment, geography, and workforce pipeline align. Here is what sets each state apart.
Mississippi: Rural Access as the Core Problem
Mississippi's shortage is overwhelmingly a geography story. Roughly 80 of the state's 82 counties contain at least one federally designated Health Professional Shortage Area, leaving enormous stretches of the Delta and hill country with almost no primary care presence. The state has taken steps to expand NP authority in recent years, and pending legislation aims to streamline the pathway to full practice authority, which could shift demand noticeably if it passes. Mississippi's primary care gap is among the most severe of any state in the country, though its psychiatric NP shortage runs a close second. If you are considering practicing in Mississippi, exploring nurse practitioner programs in Mississippi can help you understand the local training landscape.
Texas: Population Boom Outrunning Supply
Texas adds hundreds of thousands of residents each year, and NP training programs simply have not kept pace. The state currently has one of the lowest NP-to-population ratios among large states, with some estimates placing it below 50 NPs per 100,000 residents in its fastest-growing metro corridors. Texas also maintains a supervised practice model, meaning every NP must work under a physician collaboration agreement, which creates a structural bottleneck that limits where NPs can practice independently. A push to move toward full practice authority has gained momentum in the legislature, but no final action had been taken as of mid-2026.
Alaska: Isolation Amplifies Every Gap
With fewer than 60 NPs per 100,000 residents statewide, Alaska's numbers look manageable on paper until you account for geography. Many communities are accessible only by small aircraft, making recruitment and retention extremely difficult. Alaska does allow full practice authority, which removes one barrier, but the sheer physical isolation keeps vacancy rates high. The psychiatric NP shortage here is particularly acute, with many rural residents going years without access to any behavioral health provider. For NPs willing to work in remote settings, locum tenens nurse practitioner assignments can be one way to fill these gaps while testing whether a permanent move makes sense.
Missouri: Regulatory Restriction Holding Back Capacity
Missouri has long operated under a restrictive collaborative practice requirement, and that framework has historically discouraged NPs from setting up practice in underserved areas. Approximately 114 counties have been designated as primary care shortage areas. The state began moving toward modernizing its practice laws in 2025, and if those changes hold, rural Missouri could see a meaningful increase in available NP slots within a few years. For a deeper look at how these regulations compare across the country, see our nurse practitioner scope of practice guide. Primary care access is the dominant concern here, though psychiatric services are severely limited as well.
Georgia: A Two-Track Shortage
Georgia presents a split picture: rapidly growing suburban counties around Atlanta that cannot recruit NPs fast enough, alongside deeply rural counties in the south and coastal plains that have had persistent shortages for decades. More than 100 of Georgia's 159 counties are designated primary care shortage areas. Georgia's psychiatric NP gap is arguably the most pronounced of the five states, with wait times for mental health appointments in many areas stretching beyond six months. The state has expanded NP training capacity at several universities, but graduates tend to cluster in urban centers, leaving rural gaps largely unchanged.
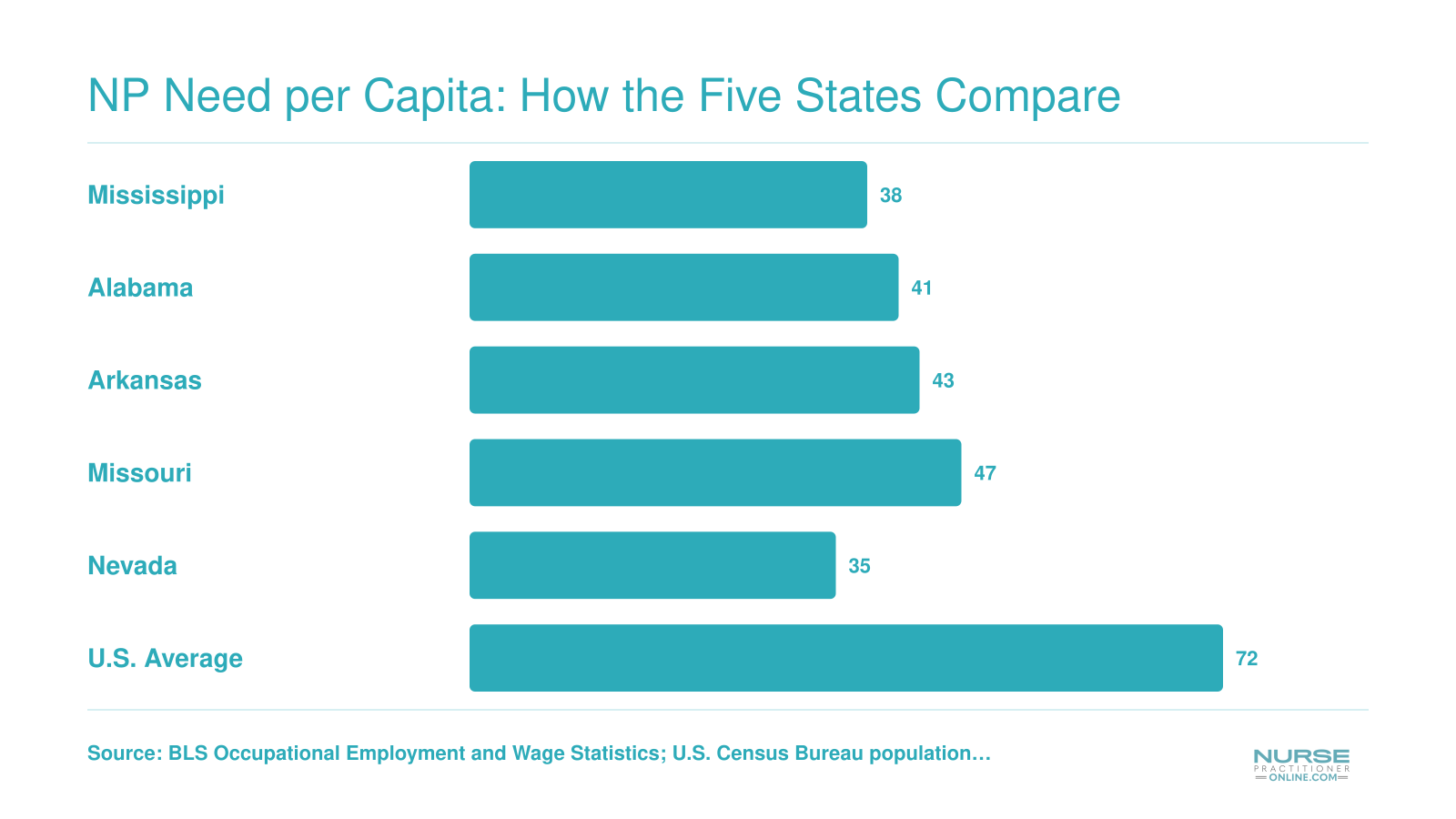
NP Need per Capita: How the Five States Compare
Not all shortages are created equal. When you adjust for population size, the gap between NP supply and patient demand becomes even more striking in certain states. The chart below shows estimated primary care NPs per 100,000 residents in each of the five highest-need states, compared with the national average.
Questions to Ask Yourself
NP Shortages in Rural Vs. Urban Areas
The shortage of nurse practitioners is not evenly distributed. In rural communities, the gap between the number of available providers and the number of patients who need care is far deeper than national averages suggest.
The Numbers Behind the Divide
According to data from the Health Resources and Services Administration, roughly 20 percent of the U.S. population lives in a primary care Health Professional Shortage Area.1 But when you look at where those shortage areas actually fall, the picture sharpens considerably. As of September 2024, more than 66 percent of designated primary care shortage areas are in rural locations.2 At the county level, 92 percent of rural counties carried a shortage designation in 2023, compared to 83 percent of non-rural counties.3 That nine-point gap understates the severity: rural shortage areas tend to be larger geographically, serve older and sicker populations, and have fewer resources to recruit replacements when a provider retires or relocates.
NPs as the Last Line of Care
In many rural counties, a nurse practitioner as primary care provider is not a supplement to a physician-led practice. The NP is the practice. The Rural Health Information Hub notes that in counties where no physician has an active primary care presence within 30 miles, NPs and other advanced practice providers often become the de facto medical home for entire communities. They handle everything from pediatric well visits to management of chronic disease to acute care that would otherwise go untreated or send patients hours down the road to the nearest emergency department.
Two of the five highest-need states illustrate how sharp the within-state divide can be. Mississippi's Jackson metro area has a functioning network of clinics and hospital-affiliated practices, while counties in the Delta region report stretches with no practicing primary care provider of any license type. West Virginia's state capital, Charleston, has established health systems drawing NPs from across Appalachia, yet the state's most mountainous counties remain chronically underserved regardless of statewide recruitment efforts.
Telehealth: Real Relief, Real Limits
The years since the pandemic created genuine momentum for telehealth as a bridge in rural areas. NP-led virtual visits expanded access for patients who could not reach a clinic, and some rural health systems reported meaningful gains in appointment volume and chronic disease monitoring. The Commonwealth Fund has documented modest but real improvements in primary care contact rates in states that moved quickly to enable telehealth practice.3
The gains are uneven, though. Broadband connectivity gaps leave portions of the most rural counties without the reliable internet needed for video visits. Several states retain telehealth-specific prescribing restrictions that limit what an NP can do remotely, even when they have full practice authority in person. Until those infrastructure and regulatory gaps close, telehealth functions as a partial fix rather than a solution. The sustained demand for in-person NPs in underserved areas also contributes to nurse practitioner burnout, making retention just as critical as recruitment. Rural patients deserve more than a partial fix.
Psychiatric NP Shortage: A Crisis Within the Crisis
What type of NP is most in demand right now, and why is it psychiatric mental health? Across the United States, over 6,800 mental health Health Professional Shortage Areas (HPSAs) leave more than 137 million people without adequate access to psychiatric care.1 In those areas, the average wait for a new psychiatric appointment can stretch longer than 30 days, and in many rural communities, no prescriber is available at all. A staggering number of U.S. counties, estimated at more than half, have no psychiatric-mental health nurse practitioner, psychiatrist, or other mental health clinician, putting the psychiatric NP shortage at the center of a broader behavioral health access crisis.
Why the Psychiatric NP Shortage Is So Acute
The demand for psychiatric mental health nurse practitioners (PMHNPs) has exploded for three converging reasons. First, the nationwide mental health need surged during and after the COVID-19 pandemic, with rates of anxiety, depression, and substance use disorders climbing sharply. Second, the psychiatrist workforce is aging out: nearly 60% of psychiatrists are over 55 and planning retirement, shrinking an already scarce physician pipeline.3 Third, PMHNP program capacity has not kept pace; relatively few NP programs offer the psychiatric specialty, and clinical placement sites are limited. The result is a perfect storm of rising patient volume, fewer traditional psychiatry providers, and a slow-growing NP specialty pool. HRSA projects that by 2033, the supply of psychiatric providers will meet only two-thirds of the demand nationally, and PMHNPs will be among the most recruited clinicians across all settings.
Where the Shortages Hit Hardest: Texas, California, and Florida
Among the states with the greatest unmet need for nurse practitioners overall, the psychiatric gap is especially severe in Texas, California, and Florida. Texas alone has 393 mental health HPSA designations, covering 13.4 million residents, and would need 606 additional mental health providers just to remove the shortage designation.1 California has 11.5 million people inside mental health HPSAs and requires 598 practitioners to close the gap, while Florida reports 9.8 million residents in mental health shortage areas and a needed increase of 545 clinicians.1 Washington and Illinois also carry significant mental health shortages, but the raw population numbers in Texas, Florida, and California make their psychiatric NP deficits the most urgent. In rural parts of these states, the situation is even more dire: travel times to the nearest prescriber often exceed an hour, and many counties have zero behavioral health providers.
The Career Signal: PMHNP Salary Premiums
For working nurses considering the PMHNP path, the shortage means strong negotiating power and above-average compensation. Nationally, psychiatric mental health nurse practitioners earn a median annual wage of around $155,000, a premium of $20,000 to $40,000 over general NP salaries.3 In high-need regions, employers frequently offer signing bonuses, loan repayment, and relocation assistance. Exploring PMHNP specialties and subspecialties can help you identify the niche that best matches your clinical interests. This salary advantage, combined with the ability to work across telehealth platforms and fill gaps in underserved communities, answers the common question directly: PMHNP is the single most in-demand NP specialty in the nation right now. You can compare nurse practitioner salary by specialty to see how the psychiatric track stacks up, and the career outlook for psychiatric NPs remains exceptionally strong through 2035 and beyond.3
Related Articles
How Scope of Practice Laws Shape NP Demand
As of mid-2026, 30 states and the District of Columbia grant nurse practitioners full practice authority, while 15 operate under reduced-practice regulations and 11 still restrict NP practice.1 These three categories create vastly different professional landscapes and directly influence where NPs can fill gaps in care.
Three tiers of practice authority
- Full practice authority: NPs can evaluate, diagnose, treat, and prescribe medications without physician oversight.
- Reduced practice: NPs need a collaborative agreement with a physician for at least one element of practice, often prescribing.
- Restricted practice: State law requires physician supervision, delegation, or team management for at least one element of NP practice.
These labels come from the American Association of Nurse Practitioners' state policy tracking, updated regularly to reflect legislative changes.
Why restrictive laws create artificial bottlenecks
In restricted-practice states, NPs cannot open independent clinics or prescribe autonomously. That means a rural health center that cannot afford or attract a collaborating physician may sit unstaffed, even if a qualified NP wants to serve the community. Among the states facing the deepest NP shortages, several still enforce restrictive regulations. South Carolina, for example, has a pending bill (3580) that would move it toward full practice authority; as of early 2026, it remains a restricted state.3 Similarly, New York adopted full practice authority in 2022 but with a 3,600-hour supervised transition, and that authority is set to sunset in July 2026 unless lawmakers make it permanent.4 This kind of uncertainty chills recruitment and makes long-term hiring difficult.
Evidence that full practice authority improves access
Workforce studies consistently link full practice authority to better primary care access, especially in underserved areas. A National Academy of Medicine report highlighted that states with fuller NP authority saw greater NP employment in rural and primary care settings. More recent data from the Health Resources and Services Administration shows that counties with full practice authority have higher NP-to-population ratios in designated shortage areas. By removing the requirement for a formal physician tie, these states let NPs quickly respond to local needs: running school-based clinics, staffing retail health sites, and opening private practices in towns that otherwise rely on emergency rooms for routine care.
The legislative push: momentum and stalemates
Since 2022, Kansas and New York joined the full practice authority states, though New York's sunset clause keeps advocates pushing for a clean, permanent fix (S2360).4 South Carolina's 2025-2026 bill reflects growing frustration among provider groups and patient advocates who point to the state's rural health deserts.3 Meanwhile, California's two-category system (103 and 104 certificates) allows independent practice after a transition, but many NPs still face administrative hurdles.5 Overall, the 2024-2026 period has seen more bills introduced to expand scope than in any preceding two-year cycle, though passage often hinges on political compromises that trade full independence for supervision-hour buffers.
Check your state's status before you commit
If you're considering NP school or relocating after graduation, scope of practice laws should be a key filter. In a restricted state, you cannot practice to the full extent of your training, and you may be unable to help the communities that need you most. The good news: every year, more states dismantle these barriers. Staying informed on your target state's legislative session can help you time your licensure or even get involved in politics as a nurse practitioner advocate.
NP Supply Pipeline: Are Schools Keeping Up?
Nursing schools are graduating more nurse practitioners than ever, yet the pipeline still falls short of projected demand, and the gap is widest in the states that need NPs the most.
National Graduates vs. Projected Openings
DNP program enrollment reached roughly 42,800 students nationally in 2024, capping more than 20 consecutive years of growth.1 That expansion is encouraging, but it tells only part of the story. The Bureau of Labor Statistics projects thousands of NP openings each year through the next decade, driven by retirements, population growth, and the ongoing shift toward primary care delivered by advanced practice providers. While a precise side-by-side comparison depends on how many enrolled students actually graduate and enter clinical practice each year, multiple workforce analyses suggest the annual output of new NPs has not kept pace with cumulative demand. The mismatch is not dramatic at the national level in any single year, but it compounds over time, particularly in states already running deficits.
Pipeline Gaps in the Five Highest-Need States
The states identified earlier in this article tend to share a common trait: they do not produce enough NPs domestically to cover their own projected openings. States with smaller populations or fewer graduate nursing programs rely heavily on interstate migration, recruiting NPs who trained elsewhere. That strategy works only when other states have a surplus to share, and in a tightening national market, the math gets harder every year. Rural states face an additional challenge because new graduates tend to gravitate toward metropolitan job markets, leaving rural counties underserved even when the statewide numbers look manageable.
Bottlenecks That Limit Growth
Even schools that want to expand are running into structural barriers.
- Clinical placement shortages: Finding quality preceptor sites remains the single largest constraint on NP program capacity. In 2024, roughly 13,000 qualified applicants were turned away from graduate nursing programs nationally, and clinical site availability was cited as a leading reason schools could not accept more students.1
- Faculty shortages: PhD nursing program enrollment has declined for 11 consecutive years, thinning the pool of doctorally prepared faculty who can teach and supervise NP students.1 Programs cannot add seats without adding instructors.
- Funding and infrastructure: Even where clinical sites and faculty exist, program budgets and simulation lab capacity can limit cohort sizes.
These bottlenecks mean that waitlists are long but graduation numbers grow only modestly from year to year.
The Role of Online NP Programs
Online and hybrid NP programs have become a critical release valve for the supply pipeline, especially in shortage states. Working nurses who cannot relocate or attend classes on a traditional campus can now earn their MSN or DNP through best online MSN nurse practitioner programs, often arranging local clinical placements with preceptors in their own communities. This model keeps students rooted in the regions that need them most, rather than funneling everyone through a handful of brick-and-mortar universities in major cities. For nurses in high-need states weighing their next career move, nursepractitioneronline.com is a practical starting point for comparing accredited programs that fit around a full-time schedule.
The bottom line: schools are trying to keep up, but systemic constraints on clinical sites, faculty, and infrastructure mean the supply pipeline will likely trail demand well into the next decade. States that invest in removing those bottlenecks, and in retaining the NPs they do produce, will be best positioned to close the gap.
NP Salary Snapshot: What High-Need States Pay
Compensation is a key factor when deciding where to practice, especially if you are considering relocating to a state with high NP demand. The table below shows how nurse practitioner salaries compare across states that face some of the greatest workforce shortages. Figures reflect the most recent federal wage data available for nurse practitioners.
| State | Total NPs Employed | 25th Percentile Salary | Median Salary | 75th Percentile Salary | Mean Salary |
|---|---|---|---|---|---|
| California | 20,980 | $140,260 | $166,610 | $205,400 | $173,190 |
| New Mexico | 1,870 | $113,240 | $138,440 | $156,000 | $136,620 |
| Montana | 1,050 | $112,180 | $133,640 | $141,050 | $131,560 |
| Alaska | 570 | $104,000 | $145,450 | $165,510 | $142,340 |
| Texas | 21,690 | $110,570 | $129,880 | $143,860 | $130,930 |
The Bureau of Labor Statistics projects nurse practitioner employment will grow 40.1% between 2024 and 2034, making it one of the fastest-growing occupations in the country. For context, that pace is roughly ten times the average growth rate across all U.S. occupations.
Future Outlook: Where NP Demand Is Headed Through 2035
The tension between today's NP shortage and tomorrow's even greater need creates both urgency and opportunity for nurses considering advanced practice careers. Understanding where demand is headed helps you make strategic decisions about specialization, location, and timing.
Federal Projections Signal Sustained Growth
The Bureau of Labor Statistics projects nurse practitioner employment to grow 45 percent between 2024 and 2034, far outpacing most healthcare occupations and the national average across all fields. This translates to roughly 135,000 new NP positions over the decade, not counting replacements for practitioners who retire or leave the profession.
State-level projections from Projections Central reveal that high-need states face even steeper climbs. States already struggling with shortages will need to fill thousands of additional positions annually just to keep pace with population growth and aging demographics.
The 65-Plus Population Surge
Census Bureau projections show the 65-and-older population will reach approximately 77 million by 2035, up from around 58 million in 2022. This 33 percent increase in older adults drives demand for primary care, chronic disease management, and mental health services, all areas where NPs play expanding roles.
Older adults average four to five times more healthcare visits than younger patients. As this demographic grows, the gap between available providers and patient needs widens, particularly in states with already thin provider networks.
Physician Shortages Amplify NP Demand
AAMC projections estimate the United States will face a shortage of between 37,800 and 124,000 physicians by 2034, with primary care and rural medicine hit hardest. HRSA reports reinforce these findings, noting that many underserved communities will rely almost entirely on NPs and physician assistants for primary care access.
This physician shortage directly increases NP demand. Healthcare systems, rural clinics, and federally qualified health centers are already restructuring care delivery models around NP-led teams. That trend will accelerate through 2035.
What This Means for Your Career Planning
If you are weighing when to pursue NP education, these projections suggest demand will remain strong for at least the next decade. Specialties addressing aging populations, psychiatric care, and primary care nurse practitioner roles in underserved areas will likely see the most consistent need.
For nurses ready to take the next step, learning how to enroll in NP school online can help you start planning around your current schedule. Professional associations like AANP and regional NP school career services offices can provide localized demand insights. Many publish annual workforce reports that break down hiring trends by specialty and geography, helping you match your interests to areas of greatest opportunity.
Common Questions About NP Shortages and Demand
Below are answers to some of the most common questions nurses ask when evaluating where nurse practitioner demand is strongest and what that means for career planning. Each response draws on the data and analysis discussed throughout this article.
- Which state has the highest demand for nurse practitioners?
- Based on the per capita analysis in this article, states with large rural populations, aging demographics, and limited primary care infrastructure consistently rank at the top. The specific leader can shift depending on whether you measure open job postings, provider shortage area designations, or NP to population ratios. However, states in the South and Mountain West regions appear most frequently among the highest need areas in 2026.
- Is there a shortage of nurse practitioners in the US?
- Yes. Federal workforce projections indicate that the gap between NP supply and patient demand continues to widen, driven by an aging population, physician retirements, and expanded insurance coverage. While NP program enrollments have grown, graduation rates have not kept pace with projected need, particularly in primary care and behavioral health specialties. Several national organizations classify the current situation as a genuine workforce shortage.
- What is the nurse practitioner to patient ratio by state?
- NP to patient ratios vary widely. States with robust NP pipelines and full practice authority tend to have more favorable ratios, sometimes one NP for every 800 to 1,200 residents. By contrast, the five high need states profiled in this article often exceed one NP for every 2,000 or more residents. Rural counties within those states can see ratios that are even more stretched.
- Which states have full practice authority for nurse practitioners?
- As of 2026, roughly half of U.S. states and Washington, D.C. grant full practice authority, allowing NPs to evaluate, diagnose, and prescribe independently. States that restrict NP scope of practice often experience sharper shortages because regulatory barriers limit NPs from filling gaps left by physician vacancies, particularly in underserved and rural communities. Full practice authority is one factor that shapes where NP demand is greatest.
- What type of nurse practitioner is most in demand?
- Psychiatric mental health nurse practitioners (PMHNPs) are currently the most sought after specialty, followed closely by family nurse practitioners and adult gerontology primary care NPs. The psychiatric NP shortage is especially severe because mental health provider gaps affect nearly every state. Family NPs also remain in high demand due to their versatility in primary care settings, which are the backbone of rural and underserved healthcare delivery.
- Where is the biggest shortage of psychiatric nurse practitioners?
- The psychiatric NP shortage is most acute in rural areas of the South and Mountain West, where mental health provider deserts overlap with high rates of substance use disorders and limited access to telepsychiatry. Several of the five states highlighted in this article have counties with zero practicing psychiatric NPs. Urban areas face their own challenges, but rural communities consistently report the deepest gaps in behavioral health coverage.