Most important takeaways…
- Palliative care NPs lead symptom management strategy for seriously ill patients at any stage, not only end of life.
- No standalone palliative care NP degree exists; you earn a primary NP certification then add the ACHPN credential.
- NP employment is projected to grow 35% from 2024 to 2034, with palliative care demand rising even faster.
- The path from RN to practicing PCNP typically spans 7 to 10 years, including a master's or doctoral degree.
A palliative care nurse practitioner is an advanced-practice provider who manages symptoms, coordinates goals-of-care conversations, and supports quality of life for patients living with serious illness. With roughly 10,000 Americans turning 65 every day through the next decade, demand for these specialists is accelerating well beyond oncology into cardiology, pulmonology, nephrology, and neurology programs nationwide.
The pathway is not direct. You must first earn a primary NP certification in a population-focus track (such as family nurse practitioner or adult-gerontology), then layer on subspecialty credentialing through the Hospice and Palliative Credentialing Center. Most clinicians spend seven to ten years moving from RN licensure through graduate school and into certified practice, a timeline that shapes everything from salary expectations to work-life balance. If you are mapping out those steps from the beginning, our overview of how to become a nurse practitioner covers the full sequence.
What Does a Palliative Care Nurse Practitioner Do?
In palliative care, the difference between RN-driven comfort and NP-led decision-making is profound. While bedside nurses manage symptoms hour by hour, the NP builds the clinical strategy that keeps suffering at bay across days, weeks, and months. That shift in scope transforms the patient experience.
Core Responsibilities: Symptom Management and Beyond
Palliative care nurse practitioners (PCNPs) own the patient's symptom plan from end to end. Their daily work includes: - Pain: titrating opioids, co-analgesics, and non-pharmacologic approaches to match the patient's goals. - Dyspnea: managing oxygen, opioids for air hunger, and non-invasive support. - Nausea, fatigue, and delirium: often with rotating protocols that demand frequent reassessment. - Advance care planning: helping families articulate what matters most, then translating those wishes into medical orders (POLST, DNR, healthcare proxy documentation). - Family meetings: acting as the translator between complex medical realities and a family's emotional readiness.
PCNPs also hold prescriptive authority. They independently initiate, adjust, and deprescribe comfort medications under collaborative agreements or full practice authority, depending on the state.
How the NP Role Differs from Bedside Palliative Nursing
RNs are the hands-on presence; NPs are the diagnostician and decision-maker. The NP can: - Order labs, imaging, and consults when symptoms change unexpectedly. - Diagnose a new source of pain or delirium that is driving distress. - Bill for services under Medicare Part B for advance care planning conversations. - Serve as the attending provider in home-based and hospice settings.
These responsibilities require a graduate-level understanding of pharmacology, pathophysiology, and family systems, skills far beyond the RN scope, even with palliative certification.
The Holistic Team and Your Place in It
PCNPs do not work alone. The care model weaves together physical, emotional, spiritual, and social support. A typical interdisciplinary team includes chaplains, social workers, music or art therapists, and hospice volunteers. The NP often coordinates this group, ensuring that a patient's uncontrolled pain is not managed in isolation from their panic or existential distress. This is a specialty that demands humility: your prescription pad is only one tool among many.
Which NP Specialties Lead to Palliative Care?
Palliative care is not a standalone NP certification track. It is a subspecialty layered on top of a primary population-focus certification. Most PCNPs start as: - Family Nurse Practitioners (FNP) - Adult-Gerontology Primary Care NPs (AGPCNP) - Adult-Gerontology Acute Care NPs (AGACNP)
The common thread is a broad clinical foundation, because the palliative population spans adolescents to centenarians. After obtaining national certification in one of these roles, NPs complete clinical hours in palliative care and then sit for the Advanced Certified Hospice and Palliative Nurse (ACHPN) exam. So when people ask "What specialty does palliative care fall under?" the answer is hospice and palliative medicine, but your entry point is always a primary NP certification first. That dual credential signals both the breadth and the depth of training required.
Palliative Care NP vs. Hospice NP: Key Differences
Palliative care NPs and hospice NPs do related work, but they serve different patient populations under different rules.1 Understanding the distinction matters for your scope of practice, your daily caseload, and how your services get billed.
Patient Eligibility and Care Goals
A palliative care NP can see patients at any stage of serious illness, including those still pursuing curative or disease-modifying treatment.1 You might manage symptoms for a patient newly diagnosed with metastatic cancer who is starting chemotherapy, or for someone living with advanced heart failure who continues to see a cardiology nurse practitioner. The goal is symptom relief and quality of life alongside ongoing treatment.
Hospice NPs work with patients who have a prognosis of six months or less if the illness runs its expected course, and who have elected to forgo curative treatment.1 The focus shifts entirely to comfort, dignity, and end-of-life care for the patient and family.
Practice Settings and Team Structure
Palliative care NPs practice across hospitals, outpatient clinics, and home-based programs, often consulting alongside oncology, cardiology, or critical care teams.2 Hospice NPs more commonly work in patients' homes, nursing facilities, and inpatient hospice units. Both roles are embedded in interdisciplinary teams that include social workers, chaplains, and bedside nurses, but hospice teams are structured around the federal hospice benefit and meet regularly to review every patient on service. For a closer look at how hospice interdisciplinary teams function, see our guide on collaboration between hospice professionals and families.
Medicare Billing Rules
This is where the distinction gets technical. Palliative care NP visits are typically billed to Medicare Part B as fee-for-service encounters, similar to other outpatient or consultative visits.3 Hospice care, by contrast, is reimbursed through a bundled per diem paid to the hospice agency, which covers nursing, aide services, medications related to the terminal diagnosis, and equipment.3
NPs working under the hospice benefit also face specific rules about serving as the attending provider versus the hospice medical director, and what they can bill separately.3 If you are weighing these two paths, the billing structure shapes not just your paycheck but the rhythm of your week.
Questions to Ask Yourself
How to Become a Palliative Care Nurse Practitioner
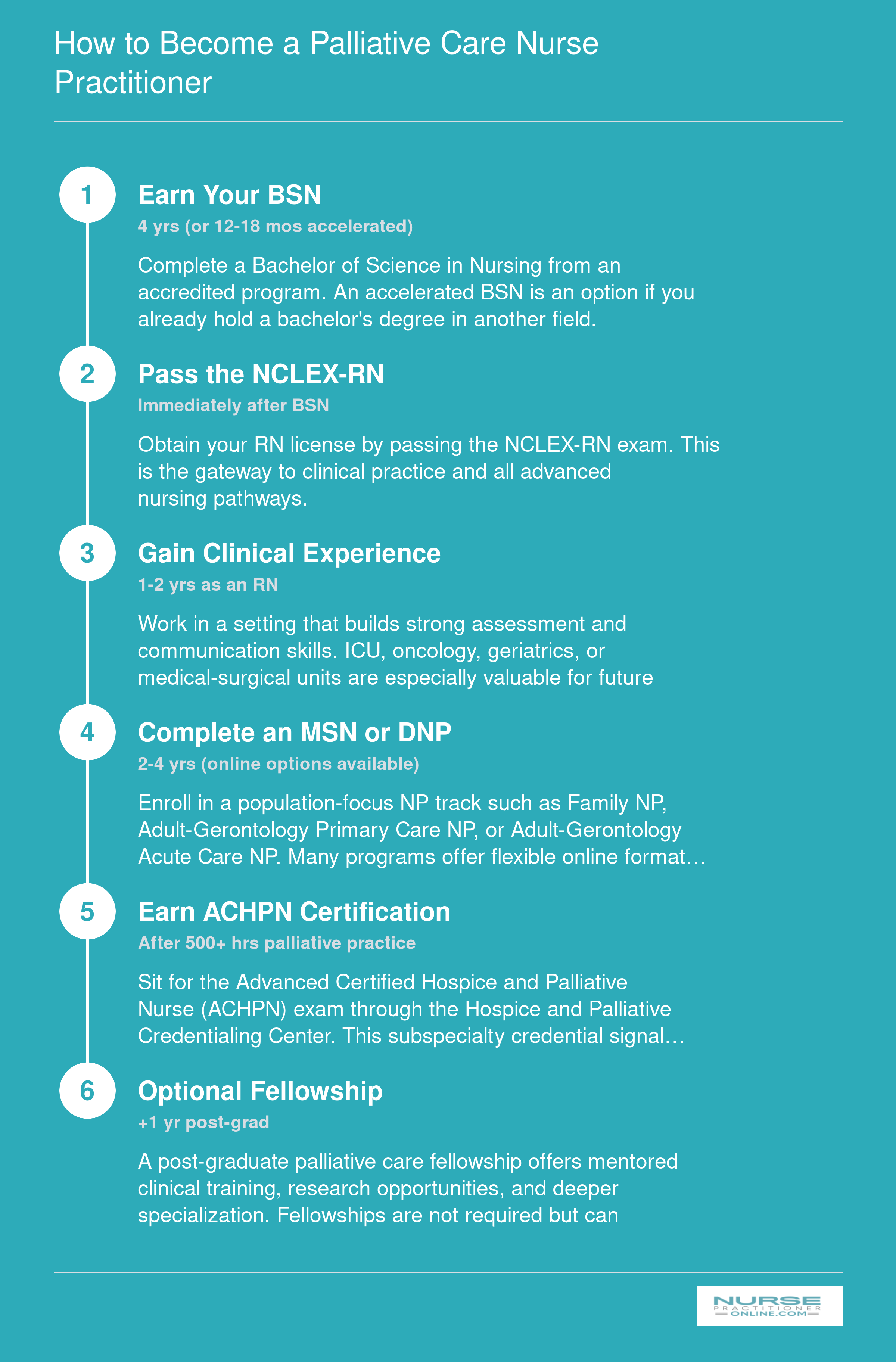
There is no standalone palliative care NP degree. Instead, you earn a primary NP certification in a population-focus track (such as FNP, AGPCNP, or AGACNP) and then add a subspecialty credential in hospice and palliative care. From your first day of a BSN program to full board certification, expect the journey to take roughly 7 to 10 years.
ACHPN Certification: Requirements, Exam, and Preparation
Earning the Advanced Certified Hospice and Palliative Nurse Practitioner (ACHPN) credential from the Hospice and Palliative Credentialing Center (HPCC) validates your expertise and signals a deep commitment to serious illness care.1 Employers, colleagues, and patients recognize it as the gold standard for nurse practitioners specializing in palliative and hospice settings. While the process requires dedication, understanding each step removes the guesswork and lets you focus on what truly matters: becoming the skilled, compassionate provider your patients deserve.
Eligibility at a Glance
Before you schedule an exam date, you will need to meet a few clear prerequisites. First, you must hold an active, unrestricted nurse practitioner license. Your advanced practice degree must be from an accredited master's or doctoral NP program; those with a Clinical Nurse Specialist (CNS) background who are certified as NPs are also eligible if their graduate program was NP-focused.1
The clinical hour requirement is where many candidates pause to plan. HPCC currently requires a minimum of 500 supervised hours in hospice and palliative care nursing practice, completed within the last two years.1 These hours must reflect the full scope of advanced practice: physical assessment, symptom management, goals-of-care conversations, and interdisciplinary team leadership. If your graduate program did not include a dedicated clinical component in palliative care, you may qualify under an alternative pathway of 1,000 hours, but most candidates find it more straightforward to accumulate the 500 hours post-degree. Tracking your hours early is smart; keep a detailed log with dates, settings, and preceptor signatures to simplify the application.
Exam Structure and Cost
Once you receive your eligibility notice, the exam itself is a computer-based test offered during four testing windows each year. You will face 175 multiple-choice questions, but only 150 count toward your score; the remaining 25 are unscored pretest items the HPCC uses to validate future questions.1 The total sitting time is 3.5 hours, so pacing yourself matters, but there is plenty of time for most candidates to work through the material thoughtfully.
Fees depend on your HPCC membership status. For members, the exam cost is $355; non-members pay $515.1 Since HPNA membership provides a discount on both the exam and renewal fees, joining is worth considering if you plan to stay engaged with the organization. All fees are subject to change, so always verify the current amount on the HPCC website right before you apply.
Pass Rates and Preparation Resources
With a latest published pass rate of 65.4%, the ACHPN exam is challenging but entirely achievable with the right study plan.2 That statistic underscores the need for structured preparation rather than last-minute cramming. The good news: high-quality review materials are readily available.
- Core curriculum textbooks: The HPNA core curriculum for advanced practice hospice and palliative care nursing is the foundational text. It aligns tightly with exam content and provides comprehensive content review.
- ELNEC training modules: The End-of-Life Nursing Education Consortium offers robust online modules covering pain and symptom management, communication, ethics, and cultural considerations, all heavily tested topics.
- Practice question banks: Multiple publishers offer test banks mirroring the exam format. Using these daily builds your familiarity with the question style and identifies weak areas.
- HPNA review course: The HPNA ACHPN Virtual Live Certification Review Course is endorsed by HPCC and delivers expert-led sessions with up-to-date strategies and content.4
Aim for a mix of self-study and interactive learning. Many successful candidates spend three to six months preparing, gradually layering comprehension with application.
Recertification Cycle and Requirements
ACHPN certification is valid for four years. To renew, you must accumulate 100 recertification points through continuing education, professional development, clinical practice, or other approved activities.3 At least 10 of those points must come from scholarly activities, such as publishing an article, presenting at a conference, or completing a research project. This ensures you stay current not only in practice but also in the evolving evidence base.
Renewal fees also vary: early-bird rates are $320 for members and $480 for non-members, while standard rates rise to $430 and $590, respectively.3 Planning your points over the four-year period rather than rushing at the end reduces stress and deepens your learning. Many NPs find that the recertification process itself becomes a rewarding journey of professional growth, connecting them with mentors, new clinical approaches, and a community of peers dedicated to transformative end-of-life care.
Palliative Care NP Salary and Job Outlook
The Bureau of Labor Statistics (BLS) reports salary data for nurse practitioners as a single occupational group, covering all NP specialties. Palliative care NPs typically earn within this national range, with variation depending on years of experience, geographic location, and practice setting. As of the latest BLS data, more than 307,000 nurse practitioners are employed across the United States, reflecting strong and growing demand for advanced practice providers in virtually every care area, including palliative and hospice medicine.
| Salary Benchmark | Annual Amount |
|---|---|
| National Median Salary | $129,210 |
| National Mean Salary | $132,000 |
| 25th Percentile | $109,940 |
| 75th Percentile | $149,570 |
| Total National NP Employment | 307,390 |
NP Salary by State: Highest-Paying Markets
Geography plays a significant role in nurse practitioner compensation. The table below highlights the top-paying states for NPs along with total employment figures. Keep in mind that many of the highest-paying states, such as California, New York, and Massachusetts, also carry a higher cost of living, which can offset the salary advantage. Several of these states also grant full practice authority, which can expand your scope and earning potential. Meanwhile, states with large and rapidly aging populations, like Florida, Texas, and Pennsylvania, may offer more palliative care specific openings even if median pay runs slightly lower. When evaluating your options, weigh salary against cost of living, practice authority laws, and the local demand for palliative and hospice services.
| State | Total NP Employment | Median Annual Salary | 25th Percentile | 75th Percentile |
|---|---|---|---|---|
| California | 20,980 | $166,610 | $140,260 | $205,400 |
| New Jersey | 9,590 | $149,620 | $126,030 | $162,250 |
| Alaska | 570 | $145,450 | $104,000 | $165,510 |
| New York | 20,430 | $145,390 | $128,190 | $164,670 |
| Oregon | 2,430 | $144,600 | $129,840 | $163,240 |
| Washington | 4,790 | $140,220 | $125,890 | $161,730 |
| Connecticut | 3,680 | $138,960 | $125,910 | $159,680 |
| Massachusetts | 8,920 | $138,890 | $125,590 | $160,310 |
| New Mexico | 1,870 | $138,440 | $113,240 | $156,000 |
| Arizona | 7,540 | $133,790 | $115,290 | $151,650 |
| Montana | 1,050 | $133,640 | $112,180 | $141,050 |
| New Hampshire | 1,790 | $132,440 | $120,270 | $143,010 |
| District of Columbia | 790 | $131,380 | $119,240 | $143,960 |
| Hawaii | 470 | $130,940 | $121,410 | $158,100 |
| Rhode Island | 1,200 | $130,710 | $126,200 | $160,030 |
| Texas | 21,690 | $129,880 | $110,570 | $143,860 |
| Colorado | 4,130 | $129,750 | $110,300 | $139,440 |
| Iowa | 2,810 | $129,420 | $115,950 | $137,900 |
| Florida | 24,690 | $129,010 | $109,670 | $143,670 |
| Indiana | 7,470 | $128,280 | $111,210 | $134,840 |
Employment of nurse practitioners is projected to grow 35% from 2024 to 2034, according to the Bureau of Labor Statistics. That is much faster than average, and as the population ages, demand for palliative care NPs is expected to be especially strong.
Where Palliative Care NPs Work: Practice Settings Compared
Palliative care nurse practitioners practice across a diverse range of settings, each offering distinct patient populations, work structures, and lifestyle trade-offs. Understanding the nuances of each environment helps you choose a practice model that aligns with your clinical interests, autonomy preferences, and personal schedule.
Hospital-Based Inpatient Consult Teams
Most PCNPs begin their careers on hospital-based consult teams, typically seeing 8 to 12 patients per day alongside attending physicians, social workers, and chaplains. You round on inpatients referred for symptom management, goals-of-care discussions, or transition planning. Autonomy varies by institution: academic medical centers often have attending-led rounds, while community hospitals may grant PCNPs more independent decision-making. Many PCNPs in these roles hold an acute care nurse practitioner credential, which prepares them for the complexity of inpatient populations. Schedules usually follow weekday daytime hours, though many teams rotate evening, weekend, or on-call coverage. Hospital consult roles tend to offer the highest base salaries in palliative care, often $115,000 to $135,000 annually, reflecting the intensity and complexity of acute-care work.
Outpatient Palliative Care Clinics
Outpatient clinics serve patients earlier in serious illness trajectories, providing symptom control, advance-care planning, and caregiver support outside the hospital. Patient volume typically ranges from 10 to 15 visits per day, with scheduled appointments and minimal on-call responsibility. Autonomy is high; you often manage your own panel with periodic physician oversight. Clinic hours are predictable, making this setting attractive for work-life balance, though compensation may be 10 to 15 percent lower than hospital roles.
Home-Based Palliative Programs
Home-based PCNPs conduct house calls, managing 4 to 8 patients daily. Travel time is built into your schedule, and you work closely with home-health agencies and family caregivers. Autonomy is substantial, as you function as the primary provider in the home. Schedules are flexible but may include occasional after-hours phone triage. This setting offers deep continuity of care and strong patient relationships.
Long-Term Care and Skilled Nursing Facilities
In nursing homes and post-acute rehabilitation centers, PCNPs provide palliative consultation for residents with advanced dementia, frailty, or chronic illness. If you are drawn to this population, an adult gerontology nurse practitioner background can be especially valuable. Patient loads vary widely, from 10 to 20 residents per day. On-call demands are typically lighter than in hospitals. Compensation tends to fall in the middle range.
Tele-Palliative Care Models
Tele-palliative care has grown rapidly since the pandemic, enabling PCNPs to conduct virtual symptom assessments, family meetings, and advance-care planning visits. You may see 12 to 16 patients per day from home or a clinic hub. Autonomy depends on state scope-of-practice laws; full practice authority states support independent telehealth NP practice, while restricted states require physician collaboration agreements even for virtual visits. Tele-PCNP roles offer exceptional schedule flexibility and often allow part-time or contract arrangements, though pay may be slightly lower than in-person hospital work. This model is especially appealing if you live in a rural area or seek geographic independence.
Daily Life, Workload, and Emotional Wellness
Palliative care is one of the most emotionally demanding yet deeply fulfilling specialties a nurse practitioner can pursue. The day-to-day reality blends clinical complexity with profound human connection, and understanding both the logistics and the emotional landscape is essential for anyone considering this path.
A Typical Day
Most palliative care NPs start with morning chart reviews and prep, often joining a brief interdisciplinary team huddle with physicians, social workers, chaplains, and nurses. Inpatient roles involve rounding on 8 to 10 patients, while community-based NPs may see 5 to 8 patients through a mix of home visits and telehealth. Each encounter focuses on symptom management, goals-of-care discussions, and family support. A midday family meeting to align care with a patient's values is common, followed by detailed documentation that captures medical decision-making and emotional nuances. The afternoon often includes new consults, follow-up calls, and collaboration with referring providers.
Call and Weekend Coverage
Call expectations vary widely. In many hospital programs, NPs share overnight and weekend call with a physician, often on a rotating schedule. Some hospices require 24/7 on-call availability a few days per month. Outpatient and community-based roles are less likely to involve overnight call, but weekend coverage is still typical. Ask directly during interviews how call is structured, what backup is available, and whether you are compensated for after-hours work.
The Emotional Weight
This is not a specialty you can leave at the hospital door. Cumulative grief, moral distress, and compassion fatigue are real occupational hazards, not signs of weakness. You will witness suffering, navigate family conflict, and occasionally question whether you did enough. Recognize that these responses are normal reactions to extraordinary circumstances. Physical symptoms like sleep disruption or irritability can appear when emotional burdens accumulate.
Protecting Your Well-Being
Research and experienced clinicians point to several evidence-based strategies for preventing nurse practitioner burnout:
- Reflective practice: Engaging in Schwartz Center Rounds or clinical supervision provides structured time to process difficult cases with colleagues in a psychologically safe space.
- Peer support: Informal debriefs with trusted palliative peers or a formal peer support group can normalize experiences and reduce isolation.
- Boundaries with technology: Set clear limits on after-hours email and messaging. Unless on call, mute work notifications at a designated time to protect personal recovery.
- Mindfulness and self-compassion: Brief daily mindfulness exercises, journaling, or simply taking a quiet moment between patients helps reset emotional reserves.
Why NPs Stay
Despite the intensity, job satisfaction among palliative care NPs remains remarkably high. The meaningful-work factor, being present for patients and families during life's most vulnerable moments, consistently outweighs the emotional demands. Many describe it as a calling that deepens their own perspective on life. This sense of purpose, combined with strong interdisciplinary teams, is a powerful retention driver.
Related Articles
Career Advancement and Subspecialties in Palliative Care
Career advancement in palliative care nursing means moving beyond generalist practice into specialized fellowship training, leadership roles, or focused subspecialties that deepen your clinical expertise. For nurse practitioners who want to provide the highest level of palliative care, post-graduate training programs offer structured pathways to advanced competency.
Post-Graduate Fellowships and Residencies
NP fellowship programs in palliative care typically run 12 months and provide intensive clinical training under expert mentorship. Most programs offered by major academic medical centers are paid positions, meaning you earn a salary while completing your training rather than paying tuition. These fellowships follow structured curricula that combine direct patient care with didactic education, research opportunities, and quality improvement projects. If you are exploring this route, our guide to nurse practitioner residency programs offers a broader look at what to expect from post-graduate training.
Institutions such as Mayo Clinic, Cleveland Clinic, and UCSF offer palliative care NP fellowships with comprehensive training in symptom management, goals-of-care conversations, and interdisciplinary team leadership. Fellowship graduates often move into senior clinical roles, program development positions, or academic appointments.
Finding the Right Program
Start your search with these professional resources:
- Hospice and Palliative Nurses Association (HPNA): Maintains directories of fellowship and residency programs specifically designed for palliative care NPs.
- Center to Advance Palliative Care (CAPC): Offers program listings and professional development resources for clinicians entering or advancing in the field.
- Academic medical center websites: Individual institutions post fellowship openings directly, so check career pages at hospitals known for strong palliative programs.
- American Nurses Association and state nursing boards: Provide links to accredited programs and continuing education opportunities.
Online professional communities can supplement your research. LinkedIn groups focused on palliative care and the HPNA community forum let you gather peer reviews and firsthand accounts from NPs who have completed specific programs.
Subspecialty Directions
Palliative care NPs can develop expertise in several focused areas:
- Pediatric palliative care: Working with children and families facing serious illness.
- Geriatric palliative care: Specializing in the complex needs of older adults with multiple chronic conditions.
- Oncology palliative care: Partnering with cancer care teams to manage symptoms and support treatment decisions.
- Heart failure or pulmonary palliative care: Addressing the unique symptom burdens of advanced cardiopulmonary disease.
Before committing to a subspecialty, confirm that the program you choose holds proper nursing program accreditation, as this affects both your eligibility for certification and future employer recognition.
Leadership and Teaching Roles
Experienced palliative care NPs often transition into leadership positions such as program director, palliative care team lead, or clinical educator. Academic roles include precepting NP students, teaching in graduate programs, or conducting research that shapes clinical practice. These paths typically require several years of clinical experience combined with fellowship training or advanced certifications.
Frequently Asked Questions About Palliative Care Nurse Practitioners
Below are answers to the questions nurses most often ask when exploring a palliative care nurse practitioner career. Each response draws on current certification requirements, scope of practice standards, and workforce data so you can plan your next steps with confidence.
- What type of NP is best for palliative care?
- An adult-gerontology primary care NP (AGPCNP) or family nurse practitioner (FNP) provides the strongest foundation for palliative care. Both tracks cover chronic illness management, symptom assessment, and goals-of-care communication across the lifespan. After completing your NP program, you can pursue the ACHPN credential through the Hospice and Palliative Credentialing Center to formalize your specialty expertise.
- What is the difference between a palliative care NP and a hospice NP?
- Palliative care NPs treat patients at any stage of a serious illness, often alongside curative therapies. Hospice NPs focus on comfort care for patients with a terminal prognosis, typically six months or less. In practice, many NPs work across both settings and hold the same ACHPN certification. The core distinction is timing: palliative care can begin at diagnosis, while hospice care begins when curative treatment stops.
- How long does it take to become a palliative care nurse practitioner?
- Plan for roughly six to eight years after high school. You will need a BSN (four years), at least one to two years of clinical RN experience (often in acute or critical care), and an MSN or DNP (two to four years). After earning your NP license, you can sit for the ACHPN certification exam once you accumulate 500 hours of supervised palliative care practice.
- How much do palliative care nurse practitioners make?
- Palliative care NP salaries align closely with general NP compensation. According to the Bureau of Labor Statistics, nurse practitioners earned a median annual wage of roughly $126,260 as of 2024. Palliative care NPs in high-cost metro areas or those holding specialty certification and DNP degrees often earn above that median. Compensation varies by employer type, geographic region, and years of experience.
- Do palliative care NPs prescribe medications?
- Yes. Palliative care NPs hold prescriptive authority in all 50 states, though the level of autonomy varies by state. They commonly prescribe opioids, anxiolytics, antiemetics, and other medications central to symptom management. In states with full practice authority, palliative care NPs prescribe independently. In reduced or restricted practice states, a collaborative agreement with a physician may be required.
- Can a family nurse practitioner work in palliative care?
- Absolutely. Family nurse practitioners are well suited to palliative care because their training spans all age groups and emphasizes holistic, patient-centered care. Many palliative care teams actively recruit FNPs. To strengthen your candidacy, consider earning the ACHPN certification and completing continuing education in pain management, serious illness communication, and end-of-life planning.
Explore More
- Acute Care Nurse Practitioner (ACNP)
- Adult-Gerontology Nurse Practitioner (AGNP)
- Cardiology Nurse Practitioner
- Critical Care Nurse Practitioner (CCNP)
- Dermatology Nurse Practitioner
- Emergency Nurse Practitioner (ENP)
- Family Nurse Practitioner (FNP)
- Forensic Nurse Practitioner
- Functional Medicine Nurse Practitioner
- Holistic Nurse Practitioner
- Neonatal Nurse Practitioner (NNP)
- Occupational Health Nurse Practitioner
- Oncology Nurse Practitioner
- Orthopedic Nurse Practitioner
- Pediatric ER Nurse
- Pediatric Nurse Practitioner (PNP)
- Psychiatric-Mental Health Nurse Practitioner (PMHNP) Guide
- Trauma Nurse Practitioner
- What Do Urgent Care Nurse Practitioners Do? Role Guide
- Women's Health Nurse Practitioner (WHNP)