Most important takeaways…
- Pediatric ER nurses manage two patients per bed, caring for the child while de-escalating anxious caregivers.
- CPEN certification is the gold-standard credential, and most competitive children's hospitals expect candidates to hold it.
- RN jobs are projected to grow 5% from 2024 to 2034, yet pediatric ER nurse supply is not keeping pace.
- Advancing to a nurse practitioner role can increase earnings by 40 to 60 percent over bedside RN pay.
Children account for roughly 20% of all emergency department visits in the United States each year, yet only a fraction of ER nurses specialize in caring for this population. A pediatric ER nurse is an RN who stabilizes and treats patients from newborns through adolescents in emergency department settings, managing everything from febrile seizures and fractures to respiratory distress and trauma.
This role is distinct from general ER nursing, which centers on adults, and from PICU nursing, which focuses on post-stabilization intensive care. Pediatric ER nurses work at the front end of the crisis, where rapid triage, weight-based medication dosing, and the ability to assess a nonverbal toddler can determine outcomes. Demand for these nurses continues to outpace supply at many children's hospitals, making the specialty both competitive to enter and hard to leave once you're in.
Pediatric ER Nurse Job Description: Core Duties and Responsibilities
What do pediatric ER nurses actually do on a shift, and how does their work differ from caring for adults? The answer lies in a skill set that combines specialized clinical expertise with the ability to connect with children and their families under intense pressure.
Rapid Triage with Age-Specific Tools
Pediatric triage is not simply a scaled-down version of adult triage. A child's condition can deteriorate quickly, so pediatric ER nurses rely on age-appropriate assessment frameworks such as the Pediatric Assessment Triangle (PAT). This rapid visual and auditory tool evaluates appearance, work of breathing, and circulation to the skin, all within seconds of the patient's arrival. The Broselow tape, a color-coded length-based measuring tape, is another essential resource that instantly estimates weight, equipment sizes, and medication dosages. Every vital sign, from heart rate to respiratory rate to blood pressure, must be interpreted against narrow age-based norms. A heart rate of 120 might be normal for a 2-year-old but alarming for a 10-year-old. Similarly, medication dosing is almost always weight-based, leaving zero room for guesswork. The pediatric ER nurse must also recognize that children often present differently: a serious infection might manifest as lethargy and poor feeding rather than a fever and productive cough. Triaging kids demands both clinical precision and a parent's intuition. You learn to trust that "something is off" feeling even when the numbers look stable.
Hands-On Clinical Skills for Small Patients
Once past triage, the hands-on work of a pediatric ER nurse highlights why this role is so distinct. Gaining intravenous access on tiny, moving veins is a daily challenge, often requiring the use of vein-finders, warm compresses, or even intraosseous access in critical moments. Calculating and administering medications is a high-stakes task: a misplaced decimal in a weight-based dose can be catastrophic, so independent double-checks are standard practice. Pediatric ER nurses frequently assist with procedural sedation for fracture reductions, laceration repairs, or imaging studies, which means they must be proficient in airway monitoring and emergency resuscitation for every age from neonate to adolescent. Splinting a toddler's arm or cleaning a playground wound requires not only technical skill but also a knack for distraction, positioning, and using child-friendly language. You might tell a 4-year-old that the pulse oximeter is a "glowing sticker" while you carefully mold a splint. Coordinating diagnostic imaging adds another layer, as children often cannot hold still without coaching or, in some cases, sedation. The procedural skill on small, frightened patients is the core differentiator that defines pediatric emergency nursing. If this specialty excites you and you're considering advanced practice, explore what a pediatric nurse practitioner role involves.
Family Communication and De-escalation
In the pediatric ER, the patient room often holds more family members than clinical staff. Parents and caregivers arrive terrified, sometimes hysterical, and they look to the nurse for reassurance and clear information. The pediatric ER nurse functions as the primary translator between the medical team and the family, breaking down complex diagnoses and treatment plans into plain, empathetic language. You explain why a CT scan is necessary, why the baby needs an IV, or why the team is moving quickly. De-escalation is a constant duty: you soothe a screaming toddler with bubbles or a tablet while calming a parent who is angry from long wait times. Strong strategies for dealing with difficult family members in healthcare are just as important here as clinical competence. Communication often includes phone calls to worried grandparents or coordination with school nurses. The best pediatric ER nurses balance honesty with hope, acknowledging fear while projecting steady competence. This emotional labor is exhausting but non-negotiable; it directly impacts patient cooperation and clinical outcomes.
Recognizing Trauma and Abuse Detection
All nurses are trained in abuse recognition, but in pediatric emergency care, the stakes are uniquely high. Pediatric ER nurses are mandated reporters, legally required to report any suspicion of child abuse or neglect. This role involves recognizing patterns of non-accidental trauma, such as fractures in non-mobile infants, bruises in unusual locations like the ears, neck, or torso, burns with clear demarcations, or stories inconsistent with the injury. The pediatric ER nurse carefully documents findings, often using forensic photography protocols, and collaborates with social workers and child protective services. These situations demand clinical objectivity, meticulous charting, and emotional resilience. You may be the first person to identify that a child is in danger, and your detailed assessment can be pivotal in a legal case. Even when the truth is unclear, the nurse's role is to advocate for the child's safety, following strict protocols while offering the child a calm, protective presence during a chaotic time.
Pediatric ER Nurse Vs. General ER Nurse Vs. PICU Nurse
While the foundation of emergency and critical care nursing is similar, the day-to-day realities for pediatric ER, general ER, and PICU nurses differ significantly. Knowing these differences can help you choose the path that best fits your strengths and goals.
Who You'll Care For and Where
- Pediatric ER Nurse: Works with patients from newborn up to 18 years old, typically in a children's hospital emergency department, an academic center's pediatric ED, or a dedicated pediatric zone inside a community hospital.1
- General ER Nurse: Cares for patients of all ages, from infants through older adults, in community hospital EDs, trauma centers, and urgent care departments.2
- PICU Nurse: Focuses on critically ill children from birth to 17 years in a pediatric intensive care unit, usually inside a children's hospital or large academic medical center.3
Daily Scope of Care
- Pediatric ER Nurse: Provides rapid stabilization and short-term management of acute illnesses and injuries, then transfers patients to an appropriate unit or discharges them.4
- General ER Nurse: Stabilizes patients across the entire age spectrum with a wide variety of emergencies, from minor issues to life-threatening conditions.2
- PICU Nurse: Delivers ongoing, intensive care for critically ill children over hours, days, or longer, managing complex life-support equipment and continuous monitoring.3
Certifications That Set You Apart
Each of these roles has a standout credential that signals specialized competence to employers and families alike. If you are exploring certifications for nurse practitioners beyond bedside roles, you will find the credentialing landscape equally nuanced at the advanced-practice level.
- Pediatric ER Nurse: The flagship credential is the Certified Pediatric Emergency Nurse (CPEN).5
- General ER Nurse: The standard is the Certified Emergency Nurse (CEN), which covers all age groups.2
- PICU Nurse: The gold standard is the CCRN (Pediatric) for acute/critical care nursing.3
Nurse-to-Patient Ratios
- Pediatric ER Nurse: For stable patients, ratios typically range from 1:2 to 1:4; the most acute cases receive 1:1 care.2
- General ER Nurse: Stable assignments are often 1:3 to 1:5, with 1:1 or 1:2 for the highest-acuity patients.2
- PICU Nurse: Ratios are consistently tighter, usually 1:1 or 1:2 at all times, reflecting the intensity of critical care.3
Common Career Crossover Paths
Pediatric ER experience opens the door to several rewarding next steps. Many nurses transition to PICU roles to deepen critical care expertise, while others move to general ER settings for broader experience.1 If you are drawn to autonomous practice with younger patients, pursuing an online pediatric NP program can formalize that trajectory.
- General ER Nurse: With additional pediatric training, you may shift into a dedicated pediatric ER or even advanced critical care roles like the PICU.1
- PICU Nurse: The pediatric intensive care background often leads naturally into the pediatric ER, where rapid decision-making and critical assessment skills are highly valued.3
Questions to Ask Yourself
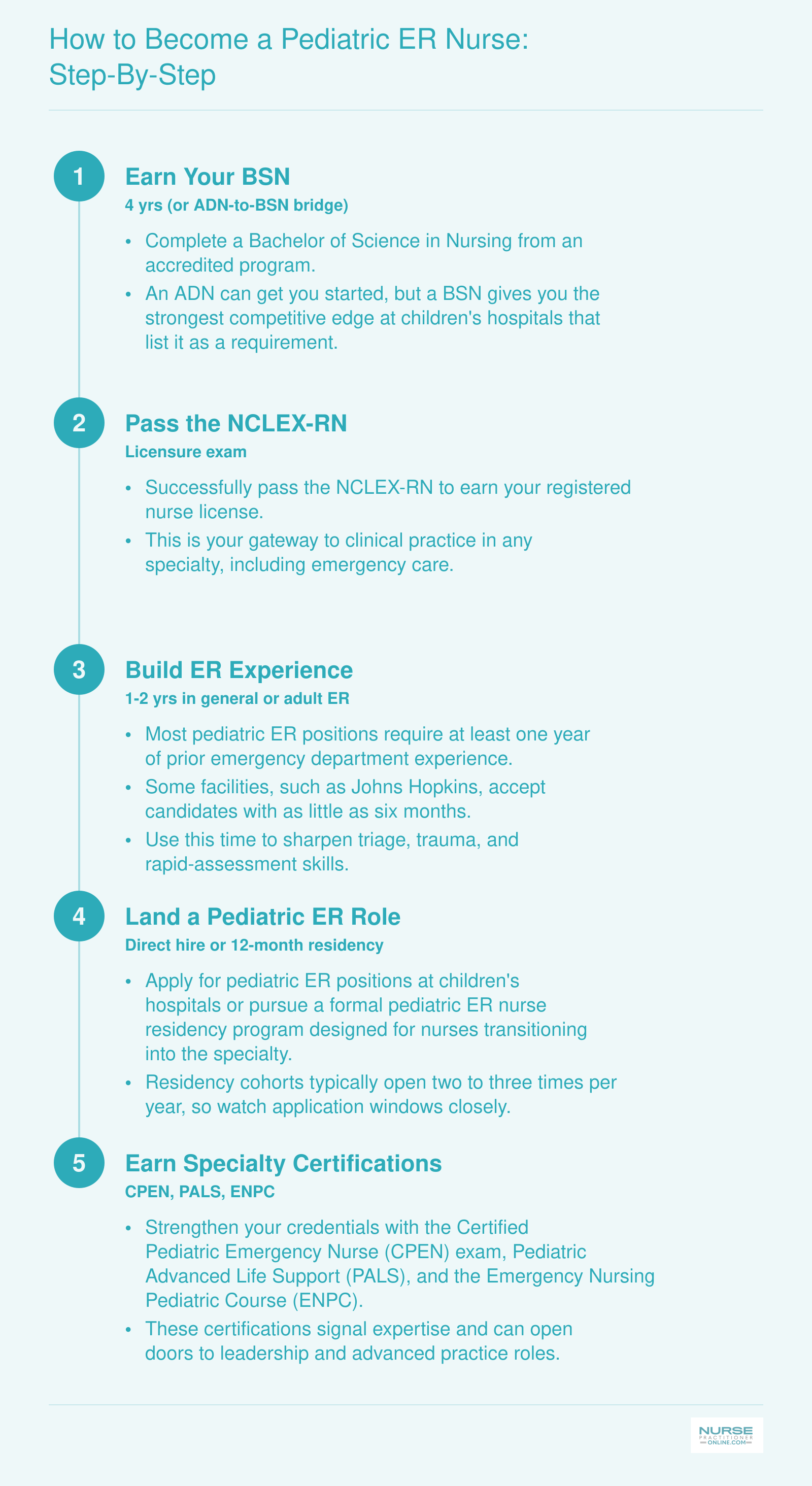
How to Become a Pediatric ER Nurse: Step-By-Step
Breaking into pediatric emergency nursing takes deliberate planning, but the pathway is straightforward. Most major children's hospitals prefer or require a BSN and at least one year of emergency department experience. While ADN-prepared nurses can get hired, the landscape is increasingly competitive, making a BSN your safest bet. New graduates who lack ER experience can sometimes enter through dedicated pediatric ER nurse residency programs offered at large children's hospitals, typically running about 12 months with two to three application cycles per year.
CPEN Certification and Other Key Credentials
The Certified Pediatric Emergency Nurse (CPEN) credential is the gold-standard specialty certification for nurses who practice in pediatric emergency settings, and most competitive children's hospitals treat it as a marker of clinical maturity even when they don't formally require it.
The CPEN Exam: What to Expect
The CPEN is administered by the Board of Certification for Emergency Nursing. To sit for it, you need a current unrestricted RN license; BCEN recommends two years of pediatric emergency experience before testing, but there are no prerequisite courses, and nurses licensed in the US, US territories, Canada, and Australia are eligible.1
The exam itself is 175 questions over 180 minutes, delivered either at a Pearson VUE testing center or through remote proctoring.2 Content is organized across six clinical domains, with 15 integrated concepts woven through them, covering triage, resuscitation, medical emergencies, trauma, mental health and abuse, and procedural support. A scaled passing score works out to roughly 75% correct, and BCEN reported a 2024 first-time pass rate of about 63.6%, so this is not a credential you walk into cold.4
The initial exam fee is $380, retakes are $200 (with a 90-day waiting period and no cap on attempts), and certification renews every four years through either 100 continuing education hours or by retesting.5 Recertification runs $280.6
PALS and ENPC: The Non-Negotiables
Before CPEN even enters the conversation, nearly every emergency department will require Pediatric Advanced Life Support (PALS) and strongly prefer the Emergency Nursing Pediatric Course (ENPC). These are foundational courses, not specialty certifications, and most EDs expect both regardless of whether you ever pursue CPEN. Treat them as the price of admission.
Salary Impact and the TCRN Add-On
Honest answer on pay: there is no robustly published salary differential specifically tied to CPEN.7 Anecdotally, certified nurses report stronger positioning for charge roles, clinical ladder advancement, and pediatric transport teams, but a guaranteed dollar figure tied to the credential isn't something the data supports.
If you work at a Level I pediatric trauma center, also consider the Trauma Certified Registered Nurse (TCRN) credential, also from BCEN. It pairs naturally with CPEN for nurses who manage major mechanism pediatric trauma alongside general emergency volume. Nurses interested in advancing further into acute-care leadership may also want to explore emergency nurse practitioner programs online or learn more about the trauma nurse practitioner role.
Related Articles
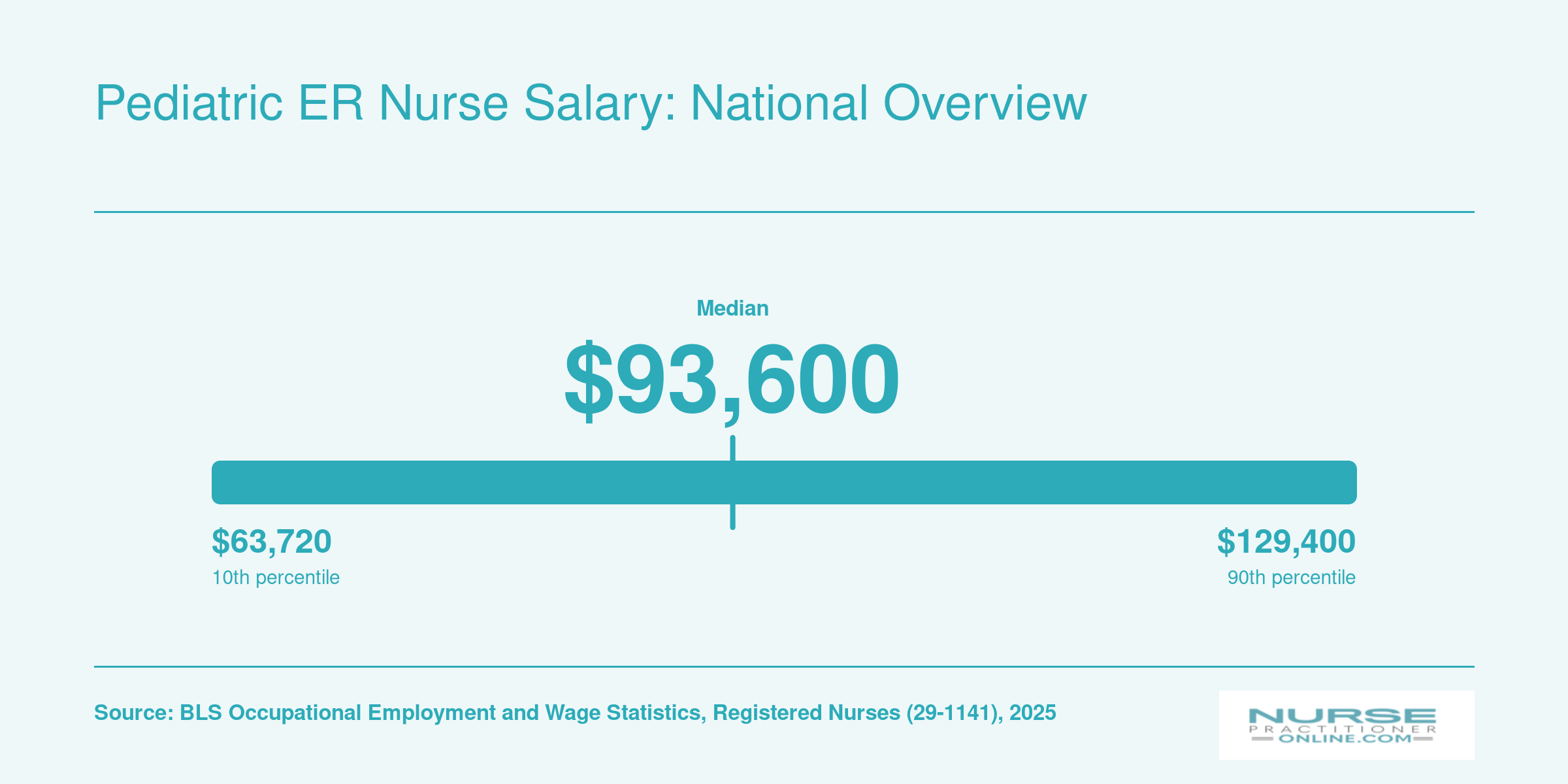
Pediatric ER Nurse Salary: National Overview
The Bureau of Labor Statistics does not break out pediatric ER nursing as a separate subspecialty, so the registered nurse salary distribution serves as the closest federal baseline. In practice, pediatric ER nurses typically earn at or slightly above these figures thanks to emergency department setting premiums, night and weekend shift differentials, and specialty credentials such as the CPEN. Industry salary aggregators place the national mean for pediatric ER nurses near $105,000 per year, reinforcing the expectation of a modest premium over the general RN median.
Pediatric ER Nurse Salary by State
The table below shows registered nurse salary data by state. Because federal labor statistics do not break out pediatric ER nurses as a separate category, these figures reflect general RN wages. Pediatric ER nurses working in high-cost states or at standalone children's hospitals, particularly those with Level I pediatric trauma center designations, may earn above the median shown here. Notably, the top five highest-paying states (Rhode Island, Arizona, New Hampshire, Maryland, and Colorado) all have at least one major standalone pediatric trauma center, suggesting a correlation between pediatric emergency infrastructure and higher RN compensation.
| State | Total RN Employment | Median Annual Salary | 25th Percentile | 75th Percentile | Mean Annual Salary |
|---|---|---|---|---|---|
| Rhode Island | 10,760 | $99,960 | $83,870 | $112,540 | $99,770 |
| Arizona | 64,430 | $96,890 | $81,390 | $105,450 | $95,230 |
| New Hampshire | 16,580 | $96,830 | $79,720 | $105,500 | $94,620 |
| Maryland | 48,980 | $96,830 | $81,470 | $104,840 | $96,650 |
| Colorado | 54,510 | $96,520 | $81,790 | $104,370 | $95,470 |
| Delaware | 13,260 | $92,610 | $82,600 | $108,360 | $95,450 |
| Texas | 261,050 | $90,010 | $77,450 | $102,200 | $91,690 |
| Virginia | 77,420 | $88,820 | $77,650 | $100,920 | $90,930 |
| New Mexico | 17,510 | $88,260 | $82,630 | $104,720 | $94,360 |
| Pennsylvania | 146,840 | $87,610 | $78,570 | $102,030 | $90,830 |
| Georgia | 97,410 | $86,560 | $76,600 | $104,790 | $91,960 |
| Illinois | 139,900 | $86,410 | $79,150 | $103,660 | $91,130 |
| Idaho | 14,540 | $86,100 | $78,020 | $100,220 | $89,770 |
| Wisconsin | 64,960 | $86,070 | $79,570 | $100,680 | $90,450 |
| Michigan | 104,210 | $85,670 | $80,030 | $101,210 | $90,580 |
| Vermont | 7,240 | $85,150 | $79,980 | $104,110 | $92,710 |
| Maine | 16,280 | $82,860 | $76,890 | $98,000 | $87,440 |
| Florida | 218,100 | $82,850 | $77,070 | $99,260 | $88,200 |
| Utah | 25,780 | $82,270 | $77,030 | $101,530 | $88,240 |
| North Carolina | 108,510 | $81,860 | $74,710 | $98,720 | $86,270 |
| Wyoming | 5,180 | $81,790 | $75,540 | $100,910 | $88,020 |
| Montana | 10,540 | $81,560 | $77,800 | $100,510 | $88,480 |
| Ohio | 138,360 | $81,250 | $77,420 | $97,440 | $86,110 |
| Oklahoma | 32,870 | $81,160 | $75,320 | $96,460 | $85,800 |
| Nebraska | 24,180 | $81,020 | $76,430 | $93,140 | $82,890 |
Work Environment, Shift Realities, and Staffing Ratios
Pediatric emergency departments operate 24/7, creating a shift-based work environment that demands flexibility and stamina. Most pediatric ER nurses work 12-hour shifts, typically three or four days per week, with rotating schedules that include nights, weekends, and holidays. Some facilities, particularly smaller community hospitals with pediatric-capable EDs, still use 8-hour shifts or hybrid models that mix both structures. Rotating schedules mean you may work a stretch of day shifts followed by nights, and many departments require nurses to share weekend and holiday coverage equitably. The intensity of this schedule is one reason nurse practitioner burnout remains a serious concern across emergency specialties.
Understanding Nurse-to-Patient Ratios
Staffing ratios in pediatric emergency departments vary significantly by state, hospital type, and acuity level. California mandates a 1:4 nurse-to-patient ratio for emergency departments, which applies to pediatric EDs as well. This legislative standard creates a baseline that many other states lack. In states without mandated ratios, pediatric ER staffing often depends on hospital policy, emergency severity index (ESI) levels, and whether the facility is a dedicated children's hospital or a general ED with pediatric capabilities.
Major children's hospitals frequently maintain lower ratios, commonly 1:3 or 1:4 for stable patients and 1:1 or 1:2 for critical or trauma cases. Community hospitals treating pediatric patients in general EDs may stretch to 1:5 or 1:6 ratios during busy periods, depending on state regulations and institutional staffing models. The Emergency Nurses Association and American Nurses Association advocate for safe staffing levels and publish position statements on recommended ratios, though these are advisory rather than binding outside states with legislation.
The Physical and Operational Setting
Pediatric ERs are designed with families in mind, featuring child-friendly decor, separate waiting areas, and treatment spaces sized for small bodies. You will work in a fast-paced environment where patient volumes fluctuate unpredictably, from quiet early morning hours to chaotic evenings when respiratory illnesses spike. The layout typically includes triage areas, treatment bays, trauma rooms, and procedure rooms equipped with pediatric-specific supplies. Nurses interested in advancing within this setting often explore becoming an emergency nurse practitioner.
Shift Handoffs and Float Requirements
Handoff communication is critical when shifts change, especially in 12-hour rotations where patient conditions can evolve dramatically. Many hospitals require pediatric ER nurses to float to inpatient pediatric units or general EDs during low-census periods, adding variability to your work environment. Understanding your facility's float policies and staffing elasticity before accepting a position helps you anticipate the full scope of scheduling demands beyond your home department.
Emotional Challenges and Building Resilience in Pediatric Emergency Nursing
Pediatric emergency nursing has become a focal point in broader conversations about healthcare worker mental health, with hospitals increasingly recognizing that emotional sustainability is as critical as clinical competency. Caring for critically ill or injured children while supporting frightened families creates a unique psychological burden that requires intentional resilience strategies.
Understanding the Emotional Landscape
Working with pediatric emergencies exposes nurses to situations that many find uniquely difficult: trauma cases involving children, parents in acute distress, and outcomes that sometimes defy the best clinical efforts. A 2023 American Academy of Pediatrics report indicates that burnout drives turnover decisions for 64% of emergency nurses, with stressful work environments cited by 52% as a contributing factor.1 While these figures reflect emergency nursing broadly rather than pediatric specialty specifically, they highlight the high-stakes emotional context you would be entering. Separately, research published in PubMed found that 25% of pediatric emergency medicine physicians reported high levels of burnout, underscoring how pervasive this challenge is across roles in the pediatric ED.2
Compassion fatigue, sometimes called secondary traumatic stress, develops when repeated exposure to others' suffering begins to erode your own emotional reserves. Pediatric cases often intensify this effect because children represent vulnerability in ways that can bypass professional detachment.
Evidence-Based Resilience Strategies
Many pediatric emergency departments have implemented structured support programs to help nurses process difficult cases. Common approaches include:
- Critical Incident Stress Debriefing: Facilitated group discussions after particularly difficult cases, allowing team members to process events together rather than carrying the emotional weight alone.
- Schwartz Rounds: Regular forums where clinical staff discuss the social and emotional aspects of caregiving, fostering connection and reducing isolation.
- Peer support programs: Trained colleagues who provide confidential check-ins and emotional first aid after challenging shifts.
If you are evaluating potential employers, ask specifically what wellness resources exist. Look for departments that normalize seeking support rather than treating emotional difficulty as weakness.
Finding Reliable Information on Workplace Wellness
To research resilience programs and mental health support in nursing, consult professional organizations like the Emergency Nurses Association, which publishes position statements and resources on nurse wellness. The American Nurses Association maintains guidance on workplace mental health standards. When evaluating specific employers, review their career pages for mentions of employee assistance programs, debriefing protocols, or wellness committees. Published studies on nursing burnout and intervention effectiveness can be found through the National Library of Medicine's PubMed database, which indexes nursing journals containing the latest research on compassion fatigue and evidence-based coping strategies.
Building personal resilience also matters. Many experienced pediatric emergency nurses credit practices like peer connection outside work, clear boundaries between shifts and home life, and ongoing professional supervision or counseling with helping them sustain long careers in this demanding specialty.
According to the Bureau of Labor Statistics, registered nursing jobs will grow 5% from 2024 to 2034, with nearly 190,000 annual openings. Yet children’s hospitals and pediatric emergency departments report that the supply of pediatric ER-trained nurses isn’t keeping pace, creating a critical workforce gap.
Career Growth: From Bedside Pediatric ER Nurse to NP and Beyond
Master's-prepared nurse practitioners often earn 40-60% more than bedside RNs, while advanced practice roles rooted in direct clinical experience enjoy the highest satisfaction ratings. For pediatric ER nurses ready to expand their scope, the question is not whether to advance but which path fits best.
The Classic Ladder: From Bedside to Nurse Practitioner
Most pediatric ER nurses follow a predictable climb. After 2-3 years at the bedside, many step into charge nurse roles, coordinating unit flow and mentoring new hires. From there, clinical nurse educator positions allow experienced nurses to design orientation curricula and lead simulation labs. The apex of clinical practice, however, is the pediatric nurse practitioner role.
Two PNP tracks exist: primary care (PNP-PC) and acute care (PNP-AC). For pediatric ER nurses, the acute care nurse practitioner track is the natural fit. PNP-AC programs emphasize resuscitation, advanced pharmacology, and differential diagnosis in high-acuity settings. Graduates work in pediatric emergency departments, trauma centers, and specialized transport teams, often functioning as the first-line provider for critical patients. They order imaging, interpret labs, suture lacerations, and manage airways independently.
MSN or DNP: Weighing Speed Against Future-Proofing
The Master of Science in Nursing remains the faster route. Most MSN-PNP programs require 2-3 years of part-time study and qualify graduates for national certification and full practice authority in most states. The Doctor of Nursing Practice adds 1-2 years and a capstone quality-improvement project. While the MSN suffices for the majority of bedside and outpatient PNP roles, the DNP is increasingly preferred at academic medical centers, opens tenure-track faculty positions, and positions nurses for health system leadership. If you're weighing the trade-offs, a deeper look at whether a DNP is worth it can help clarify the decision.
For nurses balancing work and family, the timeline matters. An MSN can be completed in as few as 24 months through an accelerated online format, and many nurses map out a plan to go from RN to NP within a defined window. DNP programs typically span 3-4 years part-time. Both degrees yield strong return on investment. National data show pediatric acute care NPs earning a median of $120,000 to $135,000 annually, compared to $75,000 to $85,000 for experienced pediatric ER staff nurses.
Lateral Moves: High-Acuity Roles Beyond the NP Track
Not every pediatric ER nurse envisions graduate school. Lateral moves offer variety and challenge without the classroom commitment. Pediatric transport nurses accompany critically ill children by ground or air between facilities, requiring CPEN and often Certified Flight Registered Nurse (CFRN) credentials. Pediatric trauma coordinators design injury-prevention programs, manage registry data, and lead multidisciplinary reviews. Emergency department nurse managers oversee staffing, budgets, and quality metrics, blending clinical expertise with operational leadership. Each path leverages emergency experience while shifting the daily focus.
Frequently Asked Questions About Pediatric ER Nursing
Below are answers to some of the most common questions nurses ask before stepping into pediatric emergency nursing. Each response offers a concise overview, and you can find more detail in the relevant sections above.
- What does a pediatric ER nurse do on a typical shift?
- A pediatric ER nurse triages young patients, performs rapid assessments, administers age-appropriate medications, assists with procedures such as splinting or suturing, and monitors vital signs throughout care. Communication is a huge part of the role: you explain treatments to frightened children while keeping parents informed and calm. Shifts are fast-paced and unpredictable, blending acute trauma cases with common childhood illnesses like asthma flares, febrile seizures, and broken bones.
- How much do pediatric ER nurses make compared to general ER nurses?
- Pediatric ER nurse salaries generally fall in line with general ER nurse pay, though exact figures vary by region, facility type, and experience. Children's hospitals in major metro areas often offer competitive base pay plus shift differentials for nights, weekends, and holidays. Specialty certifications and advanced degrees can push compensation higher. Overall, most pediatric ER nurses earn salaries comparable to, or slightly above, the median for all emergency nurses in their state.
- What certifications do pediatric ER nurses need?
- The gold standard credential is the Certified Pediatric Emergency Nurse (CPEN) designation, offered through the Board of Certification for Emergency Nursing. While not always required for hire, CPEN demonstrates specialized competence and can improve job prospects. Pediatric Advanced Life Support (PALS) certification is typically mandatory. Many employers also value Trauma Nursing Core Course (TNCC) completion and Basic Life Support (BLS) certification. Additional credentials like ENPC (Emergency Nursing Pediatric Course) further strengthen your profile.
- Is pediatric ER nursing more stressful than adult ER nursing?
- The stress is different rather than simply more or less. Caring for critically ill or injured children carries a unique emotional weight, especially when outcomes are poor. Parents' fear and grief add another layer of intensity. However, many nurses find that positive outcomes with pediatric patients are deeply rewarding. Building resilience through peer support, debriefing after difficult cases, and professional counseling resources helps nurses manage the emotional demands over a long career.
- Can new grads get hired as pediatric ER nurses?
- Some children's hospitals and large medical centers offer new graduate residency programs specifically for pediatric emergency departments. These programs typically last 6 to 12 months and pair new nurses with experienced preceptors. Competition can be stiff, so strong clinical rotations in pediatrics or emergency settings during nursing school help your application stand out. Other new graduates gain experience first on a general pediatric floor or adult ER before transitioning into a pediatric ER role.
- What is the difference between a pediatric ER nurse and a PICU nurse?
- Pediatric ER nurses focus on initial stabilization, rapid assessment, and triage of children with acute injuries or illnesses. Their work is characterized by high patient turnover and unpredictable acuity. PICU (Pediatric Intensive Care Unit) nurses, on the other hand, manage children who need prolonged critical care, often involving ventilators, continuous medication drips, and complex monitoring. The PICU environment involves deeper, longer term patient relationships, while the ER demands quick decision making across a broader range of conditions.
Explore More
- Acute Care Nurse Practitioner (ACNP)
- Adult-Gerontology Nurse Practitioner (AGNP)
- Cardiology Nurse Practitioner
- Critical Care Nurse Practitioner (CCNP)
- Dermatology Nurse Practitioner
- Emergency Nurse Practitioner (ENP)
- Family Nurse Practitioner (FNP)
- Forensic Nurse Practitioner
- Functional Medicine Nurse Practitioner
- Holistic Nurse Practitioner
- Neonatal Nurse Practitioner (NNP)
- Occupational Health Nurse Practitioner
- Oncology Nurse Practitioner
- Orthopedic Nurse Practitioner
- Palliative Care Nurse Practitioner
- Pediatric Nurse Practitioner (PNP)
- Psychiatric-Mental Health Nurse Practitioner (PMHNP) Guide
- Trauma Nurse Practitioner
- What Do Urgent Care Nurse Practitioners Do? Role Guide
- Women's Health Nurse Practitioner (WHNP)