Most important takeaways…
- NPs earn a median of $129,210 per year, roughly $43,000 more than the typical RN salary of $86,000.
- MSN programs generally take two to three years and cost between $25,000 and $75,000 depending on institution type.
- The BLS projects NP employment to grow 40 percent through 2032, far outpacing most healthcare occupations.
- Full practice authority in 27 states lets NPs prescribe, diagnose, and run clinics without physician oversight.
More than 355,000 nurse practitioners work in the United States today, and many of them started exactly where you are: as a bedside RN wondering whether the cost, time, and uncertainty of NP school are worth the trade. The average MSN program demands two years and $30,000 to $60,000 in tuition, while median NP salaries sit around $129,000 compared to $86,000 for RNs. That $43,000 gap sounds promising until you factor in clinical hour requirements, malpractice liability, state-by-state scope restrictions, and the reality that some specialties face genuine market saturation.
This is not a cheerleading piece. You will find honest numbers on return on investment, autonomy gaps by state, burnout patterns reported by newly practicing NPs, and the daily role differences that textbooks do not prepare you for. The sections ahead walk through tuition breakdowns by degree type, how to become a nurse practitioner step by step, job outlook by specialty, scope-of-practice constraints, and the transition shock many graduates face in their first independent year. The goal is to help you decide with your eyes wide open, not to sell you on a credential you may or may not need.
NP vs RN: How the Roles Actually Differ Day to Day
Twelve-hour bedside shifts versus eight-hour clinic days represent just the surface difference between RN and NP roles. The deeper distinction lies in what you own, what you decide, and how you spend your mental energy throughout each workday.
Shift Structure and Daily Workflow
As an RN, your day revolves around executing physician-driven care plans. You assess patients, administer medications, coordinate with the care team, and document within the framework of existing orders. A typical hospital RN might manage four to six patients during a 12-hour shift, with clear handoff protocols and team support at every turn.
NPs operate differently. In primary care, you might see 18 to 24 patients across an 8-hour clinic day, independently diagnosing conditions, ordering labs, prescribing medications, and building long-term treatment plans. In acute care settings, hospitalist NPs round on patient panels, admit new patients, and manage complex cases alongside physicians. The pace is relentless in both settings, but the cognitive load shifts from task execution to clinical reasoning and decision-making.
Documentation Ownership
RNs chart nursing assessments and interventions within parameters set by providers. Your documentation supports the medical record, but you are not the author of the diagnostic story.
NPs own the entire chart note. You write the history of present illness, document your physical exam findings, articulate your nurse practitioner differential diagnosis, and justify your treatment plan. Every note you sign carries your name and your reasoning. This documentation burden adds 30 to 60 minutes daily for many NPs, often completed after patients leave.
Autonomy and Liability
The weight of decision-making changes fundamentally. As an RN, you advocate for patients and catch potential errors, but the diagnostic liability rests with the ordering provider. As an NP, that liability shifts to you. If you miss a diagnosis or prescribe inappropriately, you carry professional and legal responsibility for that outcome.
This autonomy can feel empowering when you catch something early and guide a patient toward recovery. It can feel isolating when you are uncertain and lack immediate colleagues to consult.
On-Call Expectations
Primary care NPs rarely carry on-call responsibilities. You see your panel during clinic hours, and after-hours coverage typically routes to urgent care or answering services.
Acute care and hospitalist NPs face different realities. Night shifts, weekend rotations, and on-call coverage are common. Emergency department NPs work traditional shift schedules similar to RNs but with provider-level responsibilities throughout.
The Emotional Transition
Perhaps the least discussed shift involves the social dynamics of your workday. Bedside nursing involves constant interaction with patients, families, and a care team that shares physical space and immediate challenges. You celebrate small victories together and debrief difficult moments in real time.
NP practice, especially in outpatient settings, can feel surprisingly isolated. You move from room to room making independent decisions, often without another provider nearby to process a tough case. Many new NPs describe this transition as unexpectedly lonely, even when patient interactions remain meaningful. If that isolation catches you off guard, it helps to read up on preventing nurse practitioner burnout before it takes hold.
Understanding these daily realities helps you evaluate whether the NP role aligns with how you want to spend your working hours, not just what credentials you want to hold.
What NP School Really Costs, and How Long It Takes
The price tag of NP school varies dramatically depending on the degree level, institution type, and delivery format you choose, so getting clear on the numbers before you commit is one of the smartest moves you can make.
Tuition Ranges: MSN vs DNP
For MSN-NP programs, total costs generally fall between $25,000 and $80,000.1 Online MSN programs tend to land in a similar range (roughly $25,000 to $77,000), with public in-state options clustering toward the lower end. Is a DNP worth it for your situation? That question starts with the numbers. Public in-state DNP students may pay around $561 per credit hour, while private institutions can charge $1,024 per credit or more.1 High-cost private DNP programs can run $100,000 to $150,000 in total.2 If you already hold an MSN, an MSN-to-DNP bridge typically costs between $21,000 and $40,000, making it a more budget-friendly path to a doctoral degree.1 BSN-to-DNP programs, which combine both degree levels, range from about $41,000 at public in-state schools to $75,000 at private universities.1 On-campus DNP programs often carry a total cost of attendance between $80,000 and $120,000 once you factor in fees, books, and living expenses.3
Hidden Costs Most Students Miss
Tuition is only part of the equation. Budget for these commonly overlooked expenses:
- Clinical placement fees: Some programs charge $500 to $2,000 per semester to coordinate your clinical sites.
- Preceptor-finding services: If your school does not guarantee placements, third-party matching services can run $500 to $5,000.
- Certification exam fees: National board certification through the AANP or ANCC costs roughly $400.
- Background checks and compliance: Drug screenings, immunization records, and state background checks add up to several hundred dollars over the course of a program.
- Lost income: This is the biggest hidden cost. Reducing your RN hours during clinical rotations can mean thousands of dollars in foregone earnings each semester.
Realistic Timelines
How long NP school takes depends on your starting point and pace:
- Full-time MSN: 2 to 3 years
- Part-time MSN: 3 to 4 years
- BSN-to-DNP (full-time): 3 to 4 years
- Post-master's certificate: 1 to 2 years
Most working nurses choose a part-time track, which stretches the timeline but keeps a paycheck coming. For a deeper look at how these timelines break down by pathway, DNP program length varies more than most students expect.
Can You Work Full-Time While in NP School?
The honest answer: it depends on where you are in the program. During online didactic semesters, many RNs successfully maintain full-time or near-full-time schedules. The coursework is demanding, but the flexibility of asynchronous classes lets you study around shifts. Clinical rotations change the math entirely. NP programs require between 500 and over 1,000 hours of supervised clinical practice, often during business hours at outpatient sites. Most students find they need to drop to part-time or per diem nursing work during those semesters. Planning for this income dip ahead of time prevents a lot of stress.
Ways to Offset the Cost
You do not have to shoulder the entire bill alone. Many hospitals and health systems offer tuition reimbursement programs for nurses pursuing advanced degrees, sometimes covering $3,000 to $10,000 per year. Federal programs can also help. The NURSE Corps Scholarship and Loan Repayment Program covers tuition or repays a significant portion of educational debt in exchange for service at a critical-shortage facility. The National Health Service Corps (NHSC) offers similar loan repayment for NPs who practice in underserved communities. Exploring nurse practitioner loan forgiveness programs before you borrow can meaningfully change your post-graduation financial picture. Federal Direct Unsubsidized and Grad PLUS loans remain available as well, though borrowing strategically (rather than maximizing loans) keeps things healthier long term.
The bottom line: NP school is a real financial commitment, but the range of program costs means there are options at nearly every budget. The key is mapping out not just tuition but the full picture, including lost wages and ancillary fees, before you enroll.
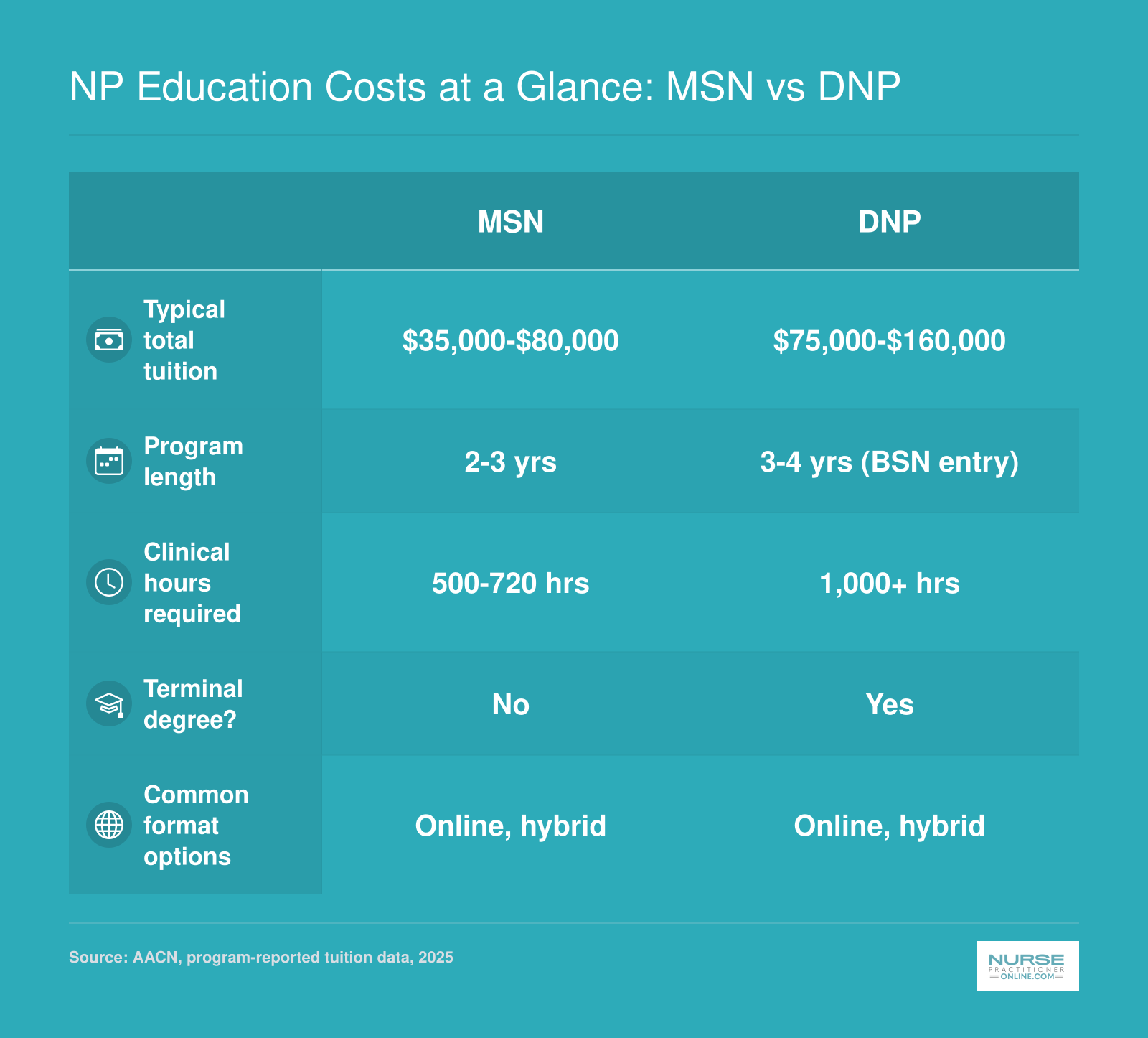
NP Education Costs at a Glance: MSN vs DNP
Deciding between an MSN and a DNP shapes your timeline, budget, and long-term credentials. Here is a side-by-side look at the key differences so you can weigh both paths before committing.
Is the Salary Bump Worth the Investment? An ROI Breakdown
Nurse practitioners nationally earn a median salary of $129,210 per year, while registered nurses typically bring in around $86,000. That gap of roughly $43,000 sets up an encouraging return on the investment in NP education.
Crunching the Numbers: The Financial ROI
NP school costs vary widely, from about $40,000 for a public in-state MSN to more than $80,000 for a private DNP. If you complete a program in three years while continuing to work part-time, the total outlay lands in that range. With a $43,000 annual salary bump, you break even in one to two years after graduation. Over a 20-year career, even a conservative estimate adds $800,000 in extra earnings above the RN baseline. That calculation assumes steady employment and no major interruptions, but it demonstrates the power of the advanced practice credential.
Where ROI Varies: Specialty, Setting, and Geography
Not all NP roles pay equally. highest paid nurse practitioner specialties include psychiatric-mental health nurse practitioners (PMHNPs), who often earn more than family nurse practitioners (FNPs), especially in underserved areas or private practice. Acute care NPs in hospital systems may command higher salaries, while primary care NPs in rural clinics might see lower figures. Geography plays a huge role: NPs in California, New York, or Massachusetts typically earn well above the national median, while those in the South or Midwest may fall below it. Practice setting matters too: hospital-employed NPs usually have higher base pay than those in private physician offices, though bonuses and profit-sharing can narrow the gap. The BLS data confirms these variations, with the top 25% of NPs earning over $149,570 and the bottom 25% at $109,940.
The Hidden Cost: Lost Overtime and Differential Pay
Many RNs boost their income through overtime, shift differentials, and weekend or holiday pay. An experienced ER or travel nurse can out-earn a primary care NP, especially in the first few years after graduation. When you transition to NP school and then into a salaried role, you often trade hourly wages and premium shifts for a fixed salary. Some new NPs report a temporary pay cut if they move away from high-overtime RN positions. Factor this in: calculate your true RN earnings including differentials, not just base pay, before assuming the NP bump will be immediate and large.
The Non-Financial Return: Career Growth and Autonomy
ROI is not only about dollars. NPs gain intellectual challenge, diagnostic authority, and the ability to manage complex cases independently. The role offers greater control over schedule, NP vs CRNA return on investment considerations aside, scope expansion into specialties, and career longevity less dependent on physical stamina. Many NPs pivot across settings, from primary care to urgent care to telehealth, which brings variety and professional resilience. These factors often tip the scales for nurses who value growth and autonomy as much as a bigger paycheck.
Questions to Ask Yourself
NP Salary by State: Where Nurse Practitioners Earn the Most
Where you practice can significantly affect your earning potential as a nurse practitioner. According to the Occupational Employment and Wage Statistics from the U.S. Bureau of Labor Statistics (2024 data), the highest paying states for NPs tend to be those with full practice authority, higher costs of living, or both. States like California, New York, and Texas also rank among the largest employers of NPs, which signals strong demand alongside competitive pay.
| State | Total Employment | Median Annual Salary | 25th Percentile | 75th Percentile |
|---|---|---|---|---|
| California | 20,980 | $166,610 | $140,260 | $205,400 |
| New Jersey | 9,590 | $149,620 | $126,030 | $162,250 |
| Alaska | 570 | $145,450 | $104,000 | $165,510 |
| New York | 20,430 | $145,390 | $128,190 | $164,670 |
| Oregon | 2,430 | $144,600 | $129,840 | $163,240 |
| Washington | 4,790 | $140,220 | $125,890 | $161,730 |
| Connecticut | 3,680 | $138,960 | $125,910 | $159,680 |
| Massachusetts | 8,920 | $138,890 | $125,590 | $160,310 |
| New Mexico | 1,870 | $138,440 | $113,240 | $156,000 |
| Arizona | 7,540 | $133,790 | $115,290 | $151,650 |
| Montana | 1,050 | $133,640 | $112,180 | $141,050 |
| New Hampshire | 1,790 | $132,440 | $120,270 | $143,010 |
| District of Columbia | 790 | $131,380 | $119,240 | $143,960 |
| Hawaii | 470 | $130,940 | $121,410 | $158,100 |
| Rhode Island | 1,200 | $130,710 | $126,200 | $160,030 |
| Texas | 21,690 | $129,880 | $110,570 | $143,860 |
| Colorado | 4,130 | $129,750 | $110,300 | $139,440 |
| Vermont | 680 | $129,740 | $115,650 | $139,930 |
| Iowa | 2,810 | $129,420 | $115,950 | $137,900 |
| Florida | 24,690 | $129,010 | $109,670 | $143,670 |
| Idaho | 1,570 | $128,940 | $119,290 | $140,920 |
| Illinois | 9,560 | $128,620 | $111,450 | $138,420 |
| Wisconsin | 4,950 | $128,580 | $117,630 | $137,150 |
| Minnesota | 8,690 | $128,570 | $103,250 | $139,590 |
| Indiana | 7,470 | $128,280 | $111,210 | $134,840 |
NP Job Outlook, Demand, and Market Saturation by Specialty
The national demand for nurse practitioners is soaring, but the real story is in the details: your specialty choice and location will heavily influence your job prospects and earning potential.
National Growth That's Hard to Ignore
The Bureau of Labor Statistics projects a 40% increase in NP jobs from 2024 to 2034, making it the third-fastest-growing occupation in the country.1 Over 128,000 new positions are expected. But here's what the headline doesn't tell you: supply is growing even faster, by 66% over the same period.3 If demand doesn't shift, that could leave a national surplus of NPs approaching 78% by 2034.3 In other words, strong overall growth masks uneven opportunity.
Where the Jobs Are (and Aren't)
Specialty matters enormously. Family nurse practitioners (FNPs) make up the bulk of the workforce, and many urban markets are already saturated. About 88% of NP students are educated in primary care, yet only 70% actually practice there, forcing a significant share into competitive non-primary-care roles.4 Meanwhile, psychiatric mental health (PMHNP), adult-gerontology acute care (AGACNP), and neonatal NP specialties consistently show stronger demand with fewer qualified applicants. Nurse practitioners in rural healthcare still face genuine shortages across the board, with many communities offering signing bonuses and loan repayment to attract providers.
The FNP Oversupply Problem
The rapid expansion of online NP programs, especially those producing large numbers of FNPs, has flooded some states with entry-level graduates. In major metros like Chicago, Dallas, or Miami, new FNPs can face months of job searching and lower starting salaries than projected. This doesn't mean FNP is a dead end , it means you must be strategic. Texas and Florida, for example, still project NP job growth near 60% and 58.5% respectively,5 but much of that demand is outside city centers.
Be Your Own Labor Market Analyst
Before committing to a program, spend a few hours browsing job boards for your preferred specialty and geography. Look at real postings: how many require experience? What's the posted salary range? Are there more openings for PMHNP or FNP in your target city? This boots-on-the-ground research often tells a very different story from national statistics. Pair it with a look at which states need nurse practitioners the most and a hard look at the schools you're considering , are they respected regionally, or will you be competing against dozens of grads from identical online programs? The NP role is still a smart investment, but only if you step in with your eyes wide open.
Choosing the Right NP Pathway: MSN, DNP, or Post-Grad Certificate
MSN programs graduate most working nurse practitioners, while DNP enrollment is growing fast and post-graduate certificates serve a niche audience of NPs switching specialties. Each pathway leads to the same national certification exam and clinical practice privileges, but they differ sharply in time, cost, and career positioning.
MSN: The Practical Default
A Master of Science in Nursing remains the standard entry credential for nurse practitioners in 2026. Most programs require 18 to 24 months of full-time study or 2 to 3 years part-time, with tuition ranging from $30,000 to $70,000 depending on the institution. MSN graduates earn the same median salary as DNP-prepared NPs, around $129,000 annually,1 and employers widely accept the degree for clinical roles. MSN enrollment has declined slightly as some universities phase out master's-only tracks in favor of direct-entry DNP programs, but the credential remains the practical choice for working RNs who want to begin practicing as soon as possible without the added time and expense of a doctoral degree.
DNP: Future-Proofing and Leadership
The Doctor of Nursing Practice takes 3 to 4 years for RNs entering from a BSN, or 1 to 2 additional years post-MSN. Total cost typically ranges from $50,000 to $100,000. DNP enrollment has grown steadily over the past three years, driven partly by speculation that the degree will become the entry requirement by 2030 or later, though no national mandate exists as of mid-2026.1 Employers increasingly prefer DNP candidates for leadership, faculty, and system-level roles; in clinical practice, however, the wage premium is negligible. For a closer look at how the numbers stack up, comparing MSN vs DNP vs PhD in nursing by salary, cost, and career trajectory can help clarify which investment makes sense for your goals. If you plan to teach, lead quality-improvement initiatives, or position yourself for administrative advancement, the DNP offers clear value. If your goal is bedside-adjacent practice in a clinic or hospital, the MSN remains sufficient.
Post-Graduate Certificate: Specialty Switchers Only
Post-graduate certificates allow already-licensed NPs to add a second specialty without repeating a full degree. Completion takes 9 to 15 months and costs $15,000 to $35,000. Employers view certificate-holders as equivalent to degree-prepared NPs once they pass the relevant certification exam.1 Enrollment in certificate programs has remained stable, serving a steady stream of family NPs moving into psych-mental health, acute care NPs pivoting to primary care, and similar transitions.
Online, Hybrid, or In-Person?
Most accredited NP programs in 2026 are hybrid: didactic coursework online, clinical rotations in person. Fully online programs still require students to arrange local preceptors and complete hundreds of face-to-face clinical hours in their home region. A handful of campus-based cohorts remain, but they are the exception. The learning modality matters less than accreditation, clinical placement support, and whether the schedule fits your work commitments.
Choose MSN if you want to practice soon and cost matters. Choose DNP if you are targeting academia, system leadership, or want to hedge against a possible future entry-standard shift. Choose a post-graduate certificate only if you already hold NP licensure and need to add a specialty.
Scope of Practice and State-By-State Autonomy
Scope of practice determines whether you can open your own clinic, sign your own prescriptions, and work without a physician looking over your shoulder. For nurse practitioners, this legal framework varies dramatically by state, and it directly shapes your day-to-day autonomy, income potential, and career flexibility.
Three Practice Authority Categories
The American Association of Nurse Practitioners tracks three distinct levels of practice authority. Full practice states allow NPs to evaluate patients, diagnose conditions, order tests, and prescribe medications independently, without any physician oversight or collaborative agreement. As of 2026, 30 jurisdictions (including U.S. territories) grant full practice authority, up from 27 in 2024.1
Reduced practice states require a written collaborative agreement with a physician. NPs can still diagnose and prescribe, but they need a formal relationship on paper with a supervising doctor. Fifteen jurisdictions currently operate under reduced practice rules.
Restricted practice states impose the tightest controls: NPs must work under direct physician supervision, and a physician may need to sign off on charts, prescriptions, or treatment plans. Eleven jurisdictions maintain restricted practice, including populous states like California and Florida.
How Practice Authority Affects Your Daily Work
In restricted states, finding a collaborating physician can delay your job start, limit where you can practice (rural areas often lack willing physicians), and cap your earning potential. Some employers deduct the cost of the collaborative agreement from NP salaries. In full practice states, you can hang your own shingle, negotiate higher compensation, and practice in underserved areas without hunting for a supervising doctor.
The Trend Toward Autonomy
More states are expanding nurse practitioner practice authority by state. California's AB 890 allows NPs to practice independently after completing 4,600 supervised hours.3 Florida's HB 607 introduced a similar pathway.3 Federal facilities have recognized full practice authority since December 2016, meaning NPs at Veterans Affairs hospitals operate independently nationwide.4
Check Your Target State Before Enrolling
If you plan to practice in a restricted state, factor in the added administrative burden and potential income ceiling. If you hope to relocate or open your own practice, prioritize full practice authority states for NPs. The AANP's State Practice Environment Map, last updated in May 2026, offers the most current breakdown.5 Where you choose to work matters as much as the credential itself.
The Realities No One Talks About: Burnout, Liability, and Transition Shock
The higher salary and expanded scope of an NP role come with trade-offs that are rarely discussed during recruitment events or program orientations. Before you commit, it is worth understanding the less glamorous side of the career so you can plan around it rather than be blindsided by it.
Burnout Is Real, and It Does Not Disappear With a New Title
If you are hoping the move from RN to NP will cure your burnout, the data suggests otherwise. A 2022 national survey found that more than 60 percent of nurse practitioners reported burnout, with roughly 62 percent saying it had lasted at least a year.1 About 20 percent reported burnout persisting for more than two years.1 Those numbers are comparable to the burnout rates seen among acute care RNs, which hovered around 60 percent in the same period.2
The sources of NP burnout look a little different from bedside nursing, though. Nearly half of NPs pointed to bureaucratic tasks (charting, prior authorizations, inbox management) as the top contributor.1 Insufficient compensation and a perceived lack of respect from physician colleagues each ranked as major factors for about 43 percent of respondents.1 Around 25 percent of NPs reported changing jobs specifically to reduce burnout, and roughly 31 percent said they had considered leaving healthcare altogether.1
None of this means the NP path is a mistake. It does mean you should go in with realistic expectations rather than assuming a role change will solve systemic workplace problems.
Malpractice Liability: A New Kind of Weight
As an RN, your employer's liability coverage typically shields you. As an NP, you carry your own clinical decision-making responsibility, and most NPs purchase individual malpractice insurance. Occurrence-based policies generally run between $1,000 and $3,000 per year, depending on your specialty and state. The dollar amount is manageable, but the psychological shift is significant. Knowing that a missed diagnosis or prescribing error could result in a malpractice claim is a very different feeling from the shared accountability of bedside nursing.
Transition Shock: The Hardest Year You Did Not Expect
Many new NPs describe the first one to two years of practice as the most difficult stretch of their careers. The phenomenon is often called "transition shock," and it shows up as imposter syndrome, decision fatigue, and a nagging sense that your training left gaps. New nurse practitioner confidence is something most new grads have to actively build rather than something programs hand you at graduation.
Part of the reason is structural. NP programs typically require 500 to 1,000 clinical hours, a fraction of what you accumulated as an RN. That clinical time was enough to learn assessment and differential diagnosis frameworks, but it rarely prepares you for the speed and volume of a full patient panel on day one. Many new NPs also report that mentorship during the transition is inconsistent or absent entirely, leaving them to figure things out through trial and error.
How to Protect Yourself Early On
The good news is that transition shock is temporary, and there are concrete steps you can take to shorten it.
- Negotiate onboarding terms: Ask for a structured orientation period before you sign a contract. Three to six months of a reduced patient load gives you breathing room to build clinical confidence without compromising patient safety.
- Find a mentor: Seek out an experienced NP or collaborating physician who is willing to answer questions and review complex cases with you. Formal mentorship programs exist through some employers and professional organizations, but informal relationships can be just as valuable.
- Budget for malpractice insurance: Factor annual premiums into your financial planning before you graduate. Getting your policy in place on day one protects you and reduces one source of anxiety.
- Expect the learning curve: Giving yourself permission to feel uncertain in the first year is not weakness. Nearly every NP who has practiced for five or more years will tell you the same thing: the first year was rough, and it got better.
Reviewing what experienced NPs wish they had known as new NPs before you start your first position can help you anticipate specific pitfalls rather than stumbling into them unprepared. Knowing about these realities in advance does not make them disappear, but it does let you build a plan that accounts for them. The NPs who navigate the transition most successfully are the ones who sought support early and refused to suffer through it in silence.
Nurse Practitioner Pros and Cons
Weighing the decision to pursue NP practice means looking honestly at both the rewards and the trade-offs. The points below synthesize the salary data, cost figures, job outlook trends, and lifestyle realities covered throughout this guide. Use them as a quick reference when you sit down to make your decision.
Pros
- Higher salary ceiling, with median NP earnings well above the registered nurse average across most states and specialties.
- Diagnostic autonomy and prescriptive authority let you drive patient care decisions from assessment through treatment.
- Diverse practice settings, from primary care clinics and hospitals to telehealth, urgent care, and specialty offices.
- Ongoing intellectual growth through differential diagnosis, evidence-based prescribing, and complex clinical reasoning.
- Clear leadership pathway into roles such as clinical director, policy advocate, or academic faculty.
- Greater career flexibility, since NP credentials are portable across a wide range of healthcare environments.
Cons
- Significant education cost and time commitment, whether you choose the MSN or DNP route, often while still working.
- Personal malpractice liability increases substantially compared to the RN role, requiring dedicated coverage.
- Productivity pressures tied to patient volume quotas can contribute to burnout, especially in primary care.
- Loss of bedside camaraderie and the team nursing culture that many RNs find professionally fulfilling.
- The FNP market is increasingly saturated in some metro areas, which can limit job options and suppress starting salaries.
- Reduced access to overtime, shift differentials, and weekend premiums that can make experienced RN take-home pay competitive with NP salaries.
Decision Checklist: Signs NP School Is (Or Isn't) Right for You
More than 355,000 nurse practitioners currently practice in the United States, each having navigated the same crossroads you face today. Before you submit a single application, work through this values-based checklist to determine whether NP school aligns with your financial situation, career goals, and personal circumstances.
Green Light Signals: You're Likely Ready
You should feel confident moving forward if several of these apply to your situation:
- Consistent clinical interest: You routinely catch yourself wanting to adjust the care plan, question diagnoses, or manage patients longitudinally rather than shift by shift.
- Financial stability: You can cover tuition (typically $30,000 to $80,000 total) while potentially reducing work hours, without jeopardizing housing or dependents.
- Real-world exposure: You have shadowed an NP in your target specialty for at least one full shift and found the workflow appealing, not just conceptually interesting.
- Geographic alignment: Your state grants full practice authority or you are willing to relocate to one that does, and you have researched the local job market for your chosen specialty.
- Timeline fit: Committing three to four years to school fits your current life stage, whether you are establishing your career or ready for a mid-career pivot.
Pause Signals: Proceed with Caution
Consider postponing your application if any of these describe your current situation:
- Salary as sole motivation: If the pay bump is your only driver, the investment may not deliver the satisfaction you expect. Many NPs report that autonomy and scope matter more than the raise.
- Unresearched market: You have not investigated whether your target specialty is saturated locally or if new graduates struggle to find positions in your region.
- Burnout as catalyst: You are already exhausted as an RN and hope that switching roles will restore your energy. Role transition typically adds stress before it alleviates it, and many NPs face comparable or greater administrative burdens.
- Unclear specialty preference: You have not identified a specific population (family, adult-gerontology, pediatric, psychiatric-mental health) that excites you beyond a vague interest in "doing more."
Your Next Concrete Step
Before applying to any program, shadow an NP in your target specialty for a full clinical day. Observe patient volume, documentation load, consultation patterns, and the rhythm of decision-making. Ask about liability insurance, prior authorization battles, and what surprised them most after graduation. This single day will reveal more than any brochure or online forum thread, and it costs you nothing but time. If you decide to move forward, reviewing how to get into NP school will help you avoid the most common application missteps.
Frequently Asked Questions About Becoming a Nurse Practitioner
These are the questions RNs ask most often when weighing the decision to pursue NP school. Each answer draws on the data and analysis covered throughout this guide.
- How long does it take to become a nurse practitioner?
- Most RNs complete an MSN in two to three years of full-time study, while a BSN-to-DNP track typically runs three to four years. Part-time and online programs can stretch the timeline to four or five years but offer the flexibility working nurses need. Clinical hour requirements (a minimum of 500 for MSN programs, often 1,000 or more for DNP programs) are usually the biggest scheduling variable.
- Can I work full-time as an RN while in NP school?
- Many online NP programs are designed for working nurses, and a large share of students do maintain full-time positions, especially during didactic coursework. The clinical practicum phase is where scheduling gets tight. Most students drop to part-time hours or use PTO during intensive clinical rotations. Planning ahead with your employer and choosing a program with flexible clinical placement support makes a significant difference.
- Is becoming a nurse practitioner worth it financially?
- In most scenarios, yes. The median NP salary exceeds the median RN salary by roughly $40,000 to $50,000 per year, according to the Bureau of Labor Statistics. Even factoring in tuition costs, lost wages during school, and loan interest, many NPs recoup their investment within three to five years of practice. The ROI breakdown earlier in this guide walks through specific numbers for MSN and DNP pathways.
- What is the difference between an MSN and a DNP for nurse practitioners?
- An MSN is the minimum degree required for NP certification and focuses on advanced clinical practice. A DNP adds coursework in leadership, health policy, evidence-based practice improvement, and systems-level thinking. Both qualify you to sit for the same NP certification exams. A DNP may open doors to academic, executive, or health system leadership roles, but it is not currently required for clinical practice in any state.
- Which NP specialty has the best job outlook right now?
- As of 2026, psychiatric-mental health NPs (PMHNPs) remain in exceptionally high demand due to a nationwide behavioral health provider shortage. Primary care family NPs (FNPs) also see strong demand, particularly in rural and underserved areas. Acute care and neonatal NP specialties tend to have fewer openings overall but face less competition per role. The specialty demand section of this guide compares outlook data across the major tracks.
- Do nurse practitioners need malpractice insurance?
- Yes. While some employers provide coverage, most experienced NPs recommend carrying your own individual policy as well. Personal malpractice insurance protects you in situations your employer's plan may not fully cover, such as claims filed after you leave a position. Annual premiums for NP malpractice coverage typically range from $500 to $2,500, depending on specialty and state. This topic is explored further in the section on liability and transition shock.