Most important takeaways…
- Missouri’s collaborative agreement requirement cost one NP business $26,000 in 2025 alone.
- About 7% of Missouri APRNs relocate to full-practice authority states such as New Mexico.
- The APRN Compact enables multi-state licensure but does not override state scope-of-practice laws.
With roughly 450,000 advanced practice registered nurses practicing across the U.S., the rules governing their work vary dramatically from one state to the next. These regulatory divides, from full practice authority to mandated collaborative agreements, directly influence where nurse practitioners can build careers and serve patients.
For some, the financial burden is concrete: Brandon Forester, an NP in Missouri, spent $26,000 on collaborative agreement fees in 2025 alone, a cost that chips away at the viability of his practice.1 That reality reflects a broader pattern. Restrictive regulations are pushing APRNs to relocate to states with the most need for nurse practitioners, reshaping both career paths and healthcare access where it is already scarce.
Why Restrictive NP Regulations Are Pushing APRNs to Move
For one Missouri nurse practitioner, the annual price of practicing in his home state hit $26,000 in 2025, not in tuition or supplies, but in collaborative agreement fees.
The Cost of Collaboration: A Missouri Example
In nearly half of U.S. states, advanced practice registered nurses must maintain a formal business arrangement with a physician to diagnose, treat, and prescribe. Missouri's rules are among the strictest: the supervising physician must be within 75 miles, regularly review charts and prescriptions, and often carries legal and financial leverage over the NP's practice. Brandon Forester, an NP since 2011, founded Midwest Medcon, a disability evaluation service for veterans, in southwest Missouri in 2020.1 His clinic now spans five states and serves roughly 4,300 veterans each year. Yet in his home state, the collaborative arrangement alone cost him $26,000 last year, a direct overhead that does nothing to improve patient care.
Building a Multi-State Practice Under Restrictions
Forester's experience highlights the operational friction restrictive regulations impose on entrepreneurial NPs. The same year he opened his Missouri practice, Kansas granted full practice authority states to APRNs, allowing him to launch a clinic there without a mandatory physician tie.1 That contrast shapes hiring, expansion, and the ability to serve rural populations efficiently. When a single state adds tens of thousands of dollars in compliance costs, it's no surprise NPs consider relocation or bypass restrictive states entirely when scaling their practices.
Legislative Setbacks and Physician Oversight
A 2026 Missouri bill that would have transitioned APRNs to full practice authority was struck down.1 Jacob Scott of the Missouri State Medical Association defended the current model, stating, "We believe in a collaborative model where physicians are the one quarterbacking the care." While such oversight is framed as a safety measure, NPs and their advocates see it as an economic and geographic tether. Valerie Fuller, president of the American Association of Nurse Practitioners, underscores the real-world fallout: "We know that there are many underserved communities across Missouri, and when you tether people like that, it prevents expansion into those underserved communities."1 A 2022 state workforce report found about 7% of Missouri's APRNs already leave to practice elsewhere, a brain drain that restrictive bills risk accelerating.
Rural Barriers for Adult-Gerontology NPs
For new graduates, particularly adult-gerontology nurse practitioners who often target careers in rural and aging communities, restrictive states present the steepest barriers. Missouri has roughly 16,000 APRNs, but about half work in hospitals or urban areas. A new NP hoping to open a rural clinic or join a community health center faces not only a tight job market but also the burden of finding and paying a collaborating physician. That reality directly affects nurse practitioners in rural healthcare, where primary care shortages are already acute. These costs alone can derail a promising career path or push new graduates toward full-practice states where they can start sooner, with fewer ongoing expenses, and directly address the communities that need them most.
Full Practice Authority vs. Restricted and Reduced Practice States
The difference between having full autonomy over your patient care and needing a physician's signature for every prescription often comes down to the state you call home. For nurse practitioners, the legal landscape is split into three tiers, each with its own impact on your day-to-day work, earning potential, and ability to serve patients where they need you most. Understanding these categories isn't just academic; it's essential for mapping out a career that aligns with your clinical goals and personal flexibility.
The Three Tiers of NP Practice Authority
The American Association of Nurse Practitioners (AANP) classifies nurse practitioner practice authority by state into three levels:1
- Full Practice Authority: In these states, NPs can evaluate, diagnose, order and interpret tests, initiate and manage treatments, and prescribe medications without a formal collaborative agreement with a physician. You practice under the sole authority of your state board of nursing. As of 2025-2026, 28 states and the District of Columbia have adopted full practice, including recent additions like New York.1
- Reduced Practice: These states require a collaborative agreement with a physician for at least one element of practice, such as prescriptive authority. Twelve states currently operate under reduced practice.1 Even if you can independently run a clinic, you might need a physician to co-sign certain orders or oversee a set number of charts.
- Restricted Practice: In the 11 remaining states, you must have a supervising physician actively involved in your care decisions.1 This typically means a collaborative agreement that dictates regular chart reviews, co-signatures, and sometimes physician presence on-site or within a defined geographical radius. In many cases, you cannot practice to the full extent of your education and training without this tethered relationship.
How Your State's Tier Shapes Your Daily Work
The tier determines not just paperwork, but your clinical autonomy and income. In a restricted state like Missouri, a collaborative agreement can cost a practice tens of thousands of dollars annually. Brandon Forester, an NP who runs a veterans' disability evaluation service, paid about $26,000 in 2025 for such an arrangement. That money could otherwise fund staff, equipment, or expansion. In full practice states, NPs can open their own clinics, bill directly under their own NPI, and hire other providers without physician involvement. Reduced practice falls somewhere in between, often allowing independent practice but limiting prescription powers or specific procedures.
Why Kansas Moved to Full Practice Authority
Kansas granted APRNs full practice authority in 2020. That same year, Forester opened a second clinic site there, free from the financial and administrative burden of maintaining a physician collaborator. His story illustrates a common pattern: NPs gravitate toward states with the most need for nurse practitioners, especially when they aim to serve rural or underserved communities that lack physician coverage. For many, the choice is not just about money; it's about reducing barriers to care in areas that desperately need it.
What to Look for in Your Own State
If you're evaluating where to build your career, or whether to stay where you are, start by checking your state's practice tier on the AANP's interactive map.1 Key questions:
- Does the law require a collaborative agreement, and what exactly must it cover?
- Is prescriptive authority independent or tied to a physician's oversight?
- Can you operate an independent practice without paying for chart reviews or cosigning fees?
- How do these rules affect your ability to work in specialty areas like adult-gerontology, where rural populations often need you most?
States like Florida, Texas, and California remain restricted,2 while many in the West and Northeast have moved to full practice. The movement is fluid: New York achieved full practice authority only recently.2 Keeping an eye on legislative changes could open doors you didn't know existed, or solidify your decision to relocate to a state that trusts nursing expertise at its fullest.
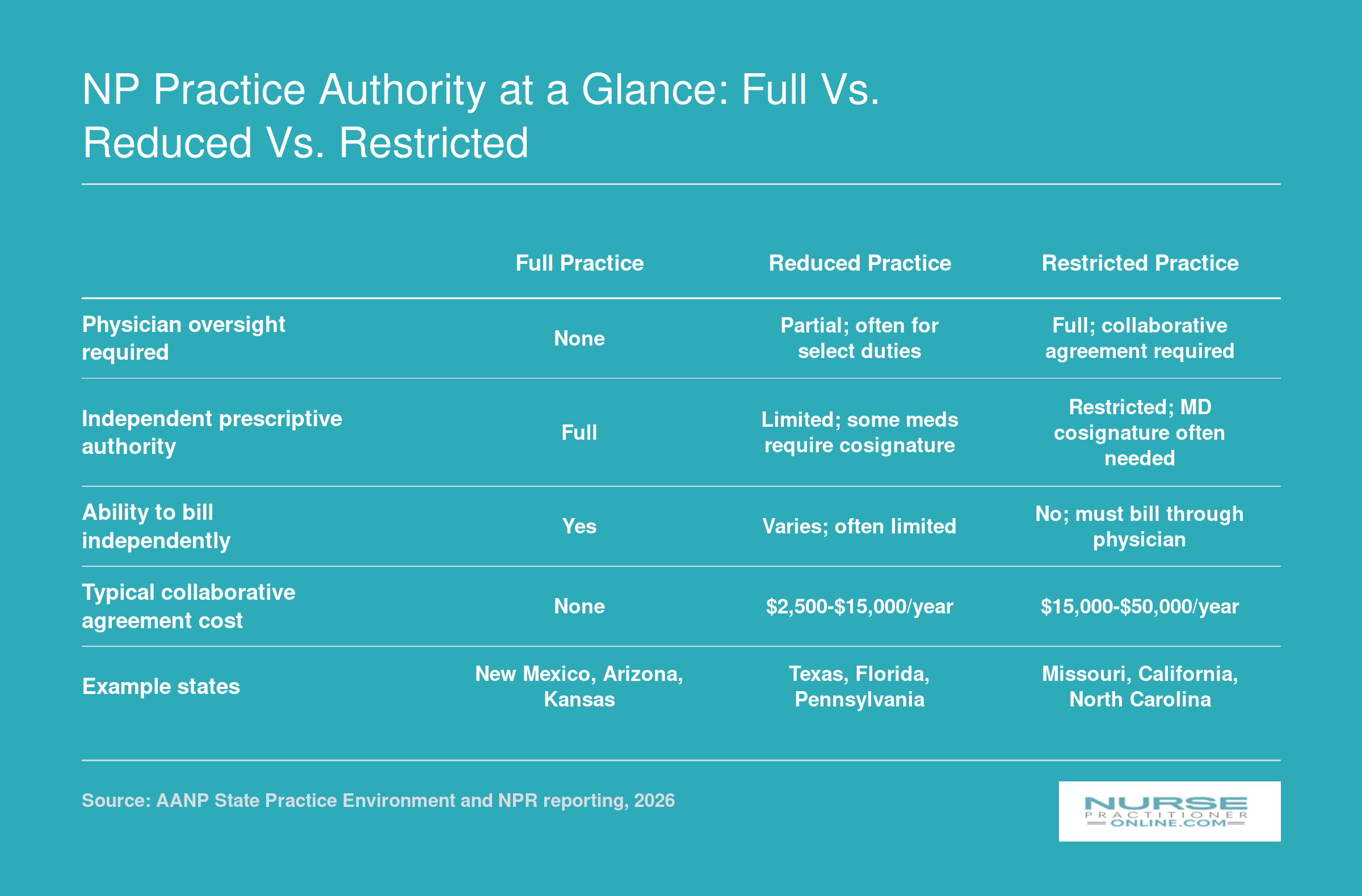
NP Practice Authority at a Glance: Full vs. Reduced vs. Restricted
Nurse practitioner practice authority varies significantly across the U.S., affecting everything from physician oversight to prescription rights. Below is a quick comparison of the three main practice tiers to help you understand the landscape.
Which States Are APRNs Moving To, and Why?
Two types of advanced practice nurses find themselves asking the same question: stay in a state that limits their authority, or move to one that trusts their training. For thousands of nurse practitioners, the answer increasingly points toward relocation.
The Pull of Full-Practice Authority
Missouri's 2022 Nursing Workforce Report highlighted a quiet migration: roughly 7 percent of the state's APRNs leave to practice elsewhere.1 With about 16,000 APRNs in the state, and roughly half working in hospitals or urban areas, that outflow represents a significant loss of primary care capacity, especially in rural and underserved communities. Valerie Fuller, president of the American Association of Nurse Practitioners, observed that this pattern repeats nationwide: APRNs commonly leave restrictive states for full-practice authority states like New Mexico, Arizona, and Nevada.
These destinations share a legislative landscape that removes the requirement for physician collaboration agreements. NPs in full-practice states evaluate patients, diagnose, order tests, and prescribe medications without a costly, sometimes intrusive partnership with a physician. For many, this equates to professional respect that matches their years of training and clinical judgment.
Compensation and Career Freedom
The financial calculus is compelling. Brandon Forester, an NP who runs a multi-state disability evaluation service, reported that collaborative agreements cost his Missouri-based business roughly $26,000 in 2025.1 In full-practice states, that overhead disappears. Meanwhile, nurse practitioner salary by state data consistently shows that NPs in these settings earn at or above the national median while enjoying greater practice autonomy. The savings from eliminated collaboration fees, combined with the ability to open independent practices or expand service lines, can accelerate career growth significantly.
Beyond the dollars, the psychological load of mandated chart reviews and prescriptive-authority tethers can weigh heavily. Moving to a full-practice state often restores a sense of professional maturity, and that intangible benefit resonates deeply with experienced NPs.
Telehealth and Border-Crossing Complexities
Relocation does not always sever ties with a former state. NPs who maintain a patient panel in their previous home state may discover that telehealth rules require them to hold a license there, and that delivering care across state lines may still demand compliance with the restrictive state's collaborative agreement rules. The APRN Compact, which facilitates multi-state practice, remains in early adoption phases (discussed in a later section). For now, NPs who move must carefully weigh whether telemedicine revenue is worth the administrative burden of dual licensure and the potential need to maintain a collaborative relationship with a supervising physician in a state they left behind.
Looking Ahead
While full-practice states continue to attract talent, the loss of providers from restrictive states like Missouri has real consequences for health equity. As Fuller noted, tethering APRNs to physician oversight prevents expansion into underserved communities.1 NP graduates, especially nurse practitioners leaving primary care for other settings, and adult-gerontology clinicians prepared for rural practice, are increasingly factoring state regulations into their job searches. The choice between staying and going is no longer just about geography; it is about the ability to practice at the top of one's license.
Questions to Ask Yourself
How to Transfer Your NP License to Another State
What exactly do you need to move your NP license to a new state, and how long will it take? The answer depends on where you're headed, but most transfers follow a predictable path. Here is a step-by-step breakdown of the process, typical costs, and practical tips to keep your career move on track.
Step 1: Verify the destination state's requirements
Before you start any paperwork, visit the website of the state board of nursing where you plan to practice. Each state sets its own rules for NP licensure by endorsement. Look for details on: whether the state is part of the APRN Compact (which allows a multistate privilege to practice), its specific continuing education (CE) requirements, any additional coursework (e.g., for prescriptive authority), and whether you'll need to provide proof of an active collaborative agreement if transitioning from a restricted practice state. States with full practice authority may have fewer documentation hurdles than those requiring supervision. For a full rundown of what licensure and certification entail, the nurse practitioner licensing and certification guide is a solid starting point.
Step 2: Gather your documents and certifications
You will generally need to assemble:
- National certification verification: Request that the ANCC or AANP send official proof of your certification directly to the new state board. Keep your certification current since lapsed credentials can delay or invalidate your application.
- Transcripts: Some states require original graduate transcripts. Contact your university early; processing can take days to weeks.
- RN license verification: Most boards use the Nursys system for interstate verification. The fee for Nurse License Verification through Nursys is typically $30 to $50.1
- Collaborative agreement records: If you worked under a physician collaboration in your previous state, retain copies of agreements, chart review documentation, and prescriptive authority delegations. Some destination states ask for this, particularly if you're seeking prescriptive authority before full practice authority is granted.
Step 3: Submit the application and pay fees
Plan for multiple fees that together range from $150 to $400.2 The core application fee for NP endorsement typically runs from $100 to $250.1 If you also need RN licensure by endorsement (which many states require before issuing an APRN license), expect an additional $75 to $200.3 A separate prescriptive authority application may cost $25 to $150.1 Budget for the total, not just the APRN application, to avoid surprises. Most boards accept online payment, and you can often track processing status through an online portal.
Step 4: Complete the background check and await processing
Every state requires a criminal background check and fingerprints are standard.3 The fee is usually between $35 and $75, not including any local fingerprinting service charges.1 Processing timelines vary: RN license endorsement can take as little as 1 to 4 weeks, while full NP licensure may take 2 to 8 weeks.3 If you have a job start date, begin the process at least 3 to 6 months in advance to allow for delays. Some states process faster if you have a clean Nursys record and no disciplinary history.
APRN Compact vs. full new application: what's the difference?
As of 2026, several states have adopted the APRN Compact, which allows an NP to practice in another compact state without a new license, similar to the RN Compact. If your destination is a compact state and your home state also participates, you may only need to maintain a single multistate license. However, not all states are members, and even within compact states, you might need to meet extra conditions for prescriptive authority. Always check the latest compact map on the NCSBN website. If the state is not in the compact, you must complete the full endorsement process described above.
Practical tips for a smooth transfer
- Start early: Give yourself 3 to 6 months before your planned move date. Delays in transcript requests, fingerprinting, or board review are common.
- Keep your national certification active: This is the fastest part to verify if it's current and unconditioned. If your CE requirements are coming due, review nurse practitioner continuing education requirements for your specialty before you apply.
- Document your collaborative practice: If you're moving from a restricted state, maintain summaries of chart reviews, supervisory meeting logs, and any notations of delegated prescriptive authority. Some boards want to see this history, especially for initial prescriptive authority approval.
- Use Nursys whenever possible: For RN verification, Nursys is the quickest and cheapest. Many state boards now accept it as primary source verification.
- Prescriptive authority is often a separate step: Even after your APRN license is issued, you may need to apply separately for controlled substance prescribing privileges. Fees and requirements vary widely, so research this alongside your main application.
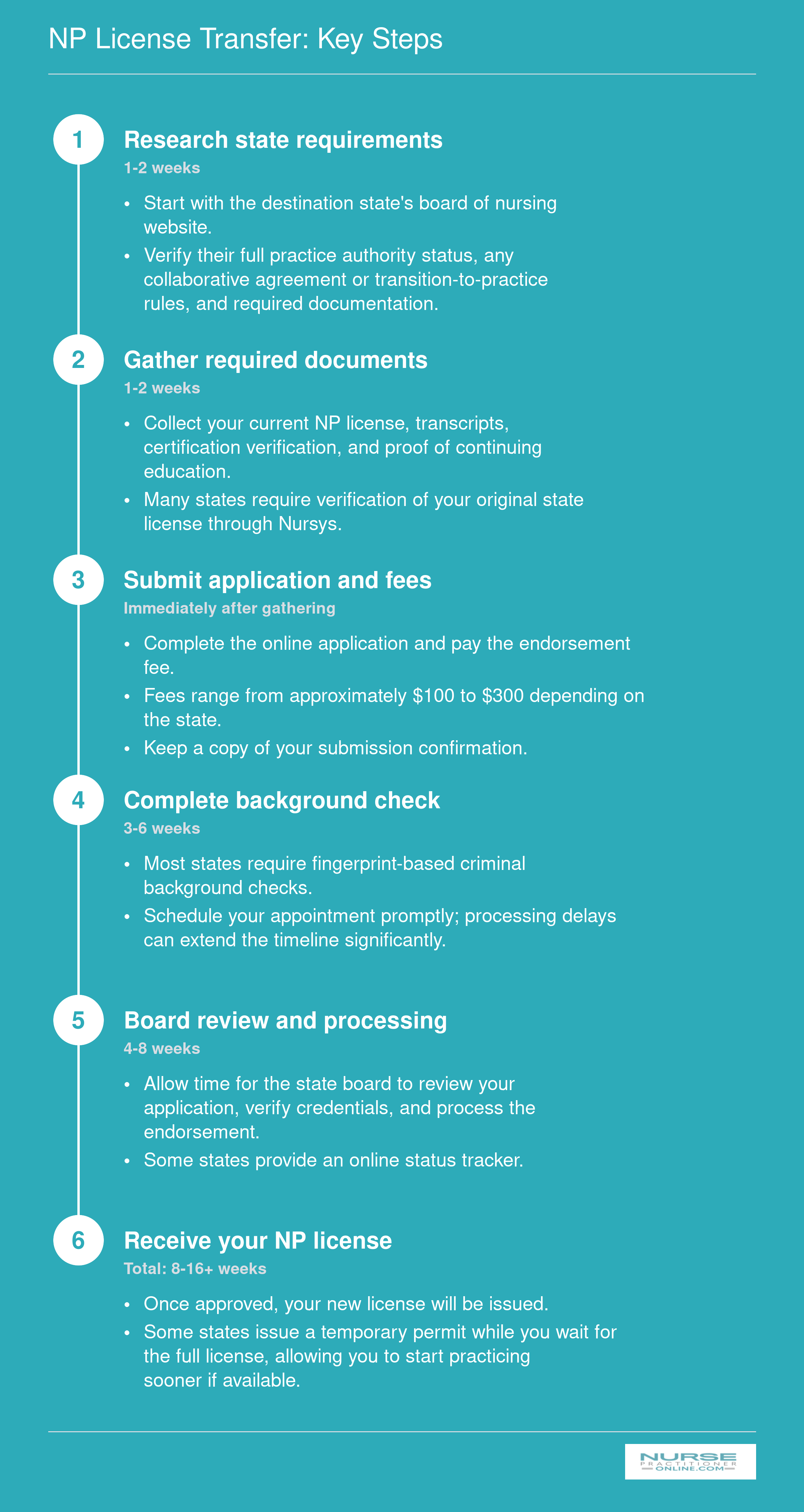
NP License Transfer: Key Steps
Moving your NP license to a new state doesn't have to be overwhelming. The process follows a predictable sequence, and with a little preparation you can keep your career on track. Here's a step-by-step overview of what to expect and how long it typically takes.
APRN Compact States in 2026: What You Need to Know
The APRN Compact is not yet active, but its promise of multistate licensure is already reshaping conversations about nurse practitioner mobility.
What Is the APRN Compact?
The APRN Compact is a multistate licensing agreement designed to let advanced practice registered nurses hold one license in a compact state and practice in any other compact state without obtaining additional licenses. It is entirely separate from the Nurse Licensure Compact (NLC), which covers registered nurses and licensed practical/vocational nurses , the NLC does not extend to advanced practice roles. Developed and endorsed by the NCSBN compacts program, the compact aims to reduce regulatory barriers, improve access to care, and support telehealth and cross-state practice.
Where Does the Compact Stand in 2026?
As of 2026, the APRN Compact is not yet active.1 Activation requires at least seven states to enact it through legislation. Only four states have fully enacted the compact so far:2
- Delaware
- North Dakota
- South Dakota
- Utah
An additional seven states have introduced legislation and are in various stages of consideration: Arizona, Idaho, Kansas, Kentucky, Montana, Nebraska, and New York.2 For example, New York's bill (S3916) remains in committee.4 Until the compact reaches the seven-state threshold, no multistate APRN licenses are being issued. NPs in every state must continue to hold individual state licenses wherever they practice.3
What the Compact Does , and Does Not , Do
Once active, the compact will allow an NP who resides in a member state and holds a compact APRN license to practice in any other member state, both in person and via telehealth. This is a meaningful advantage for NPs who live near state lines or work for multistate health systems. If you want a deeper look at how telehealth for nurse practitioners intersects with cross-state practice rules, that context is worth reviewing alongside compact developments. However, the compact does not override individual states' scope-of-practice laws. If you hold a compact license and move to a restrictive state, you must still follow that state's collaborative agreement, prescribing limits, and any other practice restrictions. The compact only addresses licensure portability, not the day-to-day authority to practice independently.
Common Misconceptions
- Misconception: The APRN Compact is already active. Reality: It is not. You still need separate state licenses even if your state has enacted the compact.5
- Misconception: The compact covers all RNs and APRNs. Reality: The NLC covers RNs and LPN/VNs, but APRNs are excluded from that compact. Only the dedicated APRN Compact addresses advanced practice licensure.
- Misconception: Joining the compact forces a state to grant full practice authority. Reality: Compact participation has no bearing on state scope-of-practice laws; you must still comply with the destination state's practice tier.
What This Means for Your Career
Until the compact reaches activation, which may still be years away, your license mobility remains tied to individual state applications. If relocation is on your mind, check whether your target state has enacted the compact and whether its practice environment matches your career goals. Staying informed through NCSBN updates and your state nursing association can help you time a move strategically. For now, the compact is a beacon of future flexibility, not a present-day shortcut.
What to Expect From an NP Relocation Package
Nurse practitioners who relocate across state lines, especially those moving to states with full practice authority, often receive financial incentives to help offset the costs of moving and settling into a new community. While packages vary by employer, facility type, and regional demand, most share a common structure aimed at making the transition financially feasible and professionally attractive.
Common Components of an NP Relocation Offer
A typical relocation package for an NP might include several elements designed to reduce the financial burden of moving. Employers frequently offer a lump-sum payment to cover moving expenses such as transporting household goods, temporary storage, or travel costs for house-hunting trips. Some organizations also provide a housing stipend or temporary lodging for the first few months. Additionally, many contracts feature a signing bonus, which can be paid as a one-time amount or spread over the first year of employment. This bonus serves as both a recruitment incentive and a way to bridge cash flow during the transition.
Understanding Signing Bonuses and Repayment Clauses
Signing bonuses are common in high-demand specialties and underserved areas, but they often come with strings attached. It is important to review the repayment clause carefully. Many employers require the NP to remain with the organization for a specified period, typically one to three years, or pay back a prorated portion of the bonus if they leave early. Repayment terms can vary widely, so understanding the time commitment and any conditions that trigger repayment is essential before signing. Ask the employer to clarify whether the bonus is contingent on meeting performance benchmarks or simply on continued employment. A solid understanding of nurse practitioner contract negotiation can help you ask the right questions before you put pen to paper.
How to Evaluate an Offer Against Cost of Living
When considering a relocation package, compare the total compensation and benefits to the local cost of living. Pay also varies considerably depending on where you land, so reviewing highest paying states for nurse practitioners can help you calibrate whether an offer is competitive for that region. Use reliable cost-of-living calculators and review local housing markets to estimate your actual purchasing power. Also consider non-salary benefits such as continuing education allowances, licensure fee reimbursement, or professional development funds, which can add significant value over the term of the contract.
Leveraging Networks and Professional Resources
To get a realistic sense of what to expect, tap into NP-specific professional networks. The American Association of Nurse Practitioners (AANP) and state-level NP organizations often share insights on compensation trends and can connect you with colleagues who have navigated similar moves. Additionally, specialty recruiters and staffing agencies that focus on placing advanced practice providers can provide anonymized compensation data and help you benchmark offers. Reviewing multiple job postings for comparable positions across different states can also reveal patterns in relocation support and help you negotiate from a position of knowledge.
How Regulation-Driven Relocation Affects Underserved Communities
What happens to rural communities when nurse practitioners pack up and move to states with fewer practice restrictions? The answer is a widening gap in healthcare access for the people who need it most. Missouri offers a stark case study. With roughly 16,000 advanced practice registered nurses (APRNs) in the state, nearly half work in hospitals or urban areas, leaving rural counties chronically underserved.1 When restrictive collaborative practice requirements drive even a small percentage of these providers to relocate, the consequences ripple through communities that already struggle to recruit and retain clinicians.
The Provider Exodus from Restrictive States
Missouri's requirement that APRNs maintain a collaborative agreement with a physician, including regular chart and prescription reviews, creates financial and logistical burdens that push some clinicians out. Valerie Fuller, president of the American Association of Nurse Practitioners, captured the core problem: "We know that there are many underserved communities across Missouri, and when you tether people like that, it prevents expansion into those underserved communities."1 When a nurse practitioner leaves for a full practice authority state like New Mexico or Arizona, the rural clinic they staffed may close or cut hours, leaving patients with nowhere else to go.
The numbers bear this out. A 2022 Missouri Nursing Workforce Report found that about 7% of APRNs leave the state to practice elsewhere.1 That might sound modest, but in rural areas where a single NP can serve hundreds of patients, each departure has an outsized impact. The $26,000 annual cost of collaborative agreements for a small practice, as reported by one Missouri NP business owner in 2025, makes it harder to sustain care in low-margin rural settings.1 Those costs often get passed along in higher patient fees or reduced service hours, further discouraging patients from seeking care.
Adult-Gerontology NPs and Aging Rural Populations
This regulatory squeeze hits especially hard for adult-gerontology nurse practitioners, who are trained to manage the complex, chronic conditions common in older adults. Rural America is aging faster than urban areas, and many small communities rely on nurse practitioners as primary care providers to manage diabetes, heart disease, and mobility issues for an older population. When those NPs relocate, elderly patients face longer travel times, delayed diagnoses, and worsening health outcomes. The same restrictive laws that are meant to ensure physician oversight instead create access deserts for the very patients who need consistent, nearby care.
Health Equity and the Bigger Picture
The tension between practice restrictions and underserved communities highlights a stark health equity problem. States like Missouri that limit NP practice authority may inadvertently widen disparities between well-served urban centers and forgotten rural pockets. While physician groups argue for collaborative models, the reality is that many rural counties have no practicing physician at all. Nurse practitioners often represent the sole source of primary care. When regulations drive them away, the most vulnerable populations, including elderly, low-income, and chronically ill patients, pay the price.
This is not just a Missouri issue. In many restricted practice states, the pattern repeats: well-intentioned oversight rules can end up straining the safety net that keeps rural America healthy. For nurse practitioners deciding where to build their careers, understanding this dynamic is a critical part of making an informed choice, and an invitation to get involved in nurse practitioner health policy to protect both clinicians and the communities they serve.
Advocacy, Policy Literacy, and Your Career Path Forward
You can wait for your state to change its regulations , or you can help write the next chapter. For nurse practitioners who want to practice at the top of their license, policy literacy is not an optional soft skill; it's a career accelerator. Understanding how nurse practitioner scope of practice laws are made, amended, and enforced gives you the power to choose environments that fit your goals and to influence the systems that shape patient care.
Building Your Policy Literacy
Start by tracking the legislative process in your state. Identify the key committees that hear healthcare bills, note the annual session calendar, and subscribe to alerts from your state board of nursing. The American Association of Nurse Practitioners (AANP) maintains a state-by-state policy tracker that highlights active full-practice-authority bills, pending collaborative agreement reforms, and APRN compact legislation. Pair that with regular updates from your state NP association, as these groups often have the most granular, timely intelligence on local political dynamics. When a bill like Missouri's 2026 attempt to move to full practice authority surfaces, you'll already know the players, the arguments, and the timeline, positioning you to act quickly.
Concrete Actions That Move the Needle
Advocacy is most powerful when it's personal and persistent. Consider these high-impact steps: - Testify at state legislative hearings: A three-minute personal story about how restrictive regulations limit your ability to serve patients can shift committee votes. - Join AANP's advocacy initiatives: Their annual Capitol Hill fly-in and grassroots action alerts make it easy to contact lawmakers with pre-drafted messages you can customize. - Write to your legislators: A concise, polite letter explaining how a collaborative agreement requirement affects your practice , or your decision to leave the state , carries weight, especially if you represent a rural or underserved constituency. - Connect with state-level coalitions: Many full-practice-authority victories have been won by broad coalitions of NPs, physician assistants, patient advocates, and rural health organizations. Together, you amplify the message that healthcare access depends on modernizing licensure.
Practice Authority as a Career Planning Factor
For new graduates, the conversation often starts with salary, location, and sign-on bonuses. But practicing under a restricted framework can cap your autonomy and entrepreneurial options for years. When evaluating job offers, ask direct questions: Does the employer handle the collaborative agreement, or will you need to find and pay a collaborating physician yourself? What happens if that physician retires or moves? If you dream of opening your own clinic or serving a remote community, you'll want a state that allows it without expensive contractual tethers. Including practice authority in your early career calculus can prevent a costly relocation down the road and position you for leadership roles sooner. Reviewing AANP membership benefits can help you identify the advocacy resources and professional networks available to support that planning.
The Momentum Toward Full Practice Authority
The landscape is shifting. Kansas granted APRNs full practice authority in 2020, a move that directly enabled clinicians like Brandon Forester to open veteran disability-evaluation clinics and expand across multiple states without physician oversight. More states are weighing similar bills each session. The evidence base showing equivalent or superior outcomes in full-practice states continues to grow. NPs who combine clinical skill with policy awareness don't just react to regulatory changes; they accelerate them. Whether you stay and advocate or move to a full-practice state, your engagement helps build a profession where every advanced practice nurse can serve patients to the full extent of their training.
Frequently Asked Questions About NP Regulations and Relocation
Navigating NP regulations and relocation logistics can feel overwhelming. Below we answer common questions to help you understand your options, from licensing transfers to compact agreements, so you can make informed career decisions.
- Can nurse practitioners move to another state and keep practicing?
- Yes, but you must obtain a license in the new state. Since NP licenses are state-specific, you'll apply for licensure by endorsement if you hold an active license elsewhere. Plan ahead, as processing times vary. For a step-by-step guide, see the section 'How to Transfer Your NP License to Another State.'
- Which states have full practice authority for nurse practitioners?
- Full practice authority states allow NPs to evaluate, diagnose, treat, and prescribe without physician oversight. As of 2026, over half of U.S. states grant full practice authority, including New Mexico, Arizona, and Nevada. For a complete list and details, see the section 'Full Practice Authority vs. Restricted and Reduced Practice States.'
- How do I transfer my NP license to another state?
- The process involves verifying your eligibility, completing state-specific applications, submitting transcripts and certifications, and undergoing a background check. Each state board sets its own requirements and timelines. For a detailed walkthrough, refer to the section 'How to Transfer Your NP License to Another State' and the accompanying infographic.
- What is the APRN Compact and which states participate?
- The APRN Compact allows NPs to hold one multistate license to practice in all member states, similar to the RN compact. As of 2026, only a few states have enacted legislation to join, but more are considering it. For current participants and requirements, see 'APRN Compact States in 2026: What You Need to Know.'
- How much do NP relocation packages typically cover?
- Relocation packages can range from $5,000 to $20,000 or more, covering moving costs, temporary housing, and sometimes sign-on bonuses. The amount varies by employer, location demand, and experience. For a detailed breakdown, see the section 'What to Expect From an NP Relocation Package' and its companion infographic.
- Do restrictive NP regulations affect rural healthcare access?
- Yes. Restrictive regulations, such as mandatory collaborative agreements, often push NPs away from underserved rural areas where physicians are scarce, worsening provider shortages. This creates significant access barriers for patients. Explore the impact further in the section 'How Regulation-Driven Relocation Affects Underserved Communities.'
- Can I use telehealth to treat patients in a state where I'm not licensed?
- Typically, you need a license in the state where the patient is physically located. Some states have exceptions or participate in compacts, and temporary waivers may exist. Always verify the specific telehealth regulations of each state before providing care. For more information, see the section on the APRN Compact.