Most important takeaways…
- No U.S. state requires a DNP for nurse practitioner licensure in 2026, and MSN programs continue enrolling more NP students than DNP programs.
- CRNAs are the sole APRN specialty with a binding doctoral mandate, effective January 1, 2025, for new program entrants.
- AGACNP certification remains available through MSN preparation, with no doctoral degree required by any credentialing body.
- If any state ever mandates the DNP, regulatory precedent strongly supports grandfathering existing MSN-prepared nurse practitioners.
The 2025 deadline set by the American Association of Colleges of Nursing and the National Organization of Nurse Practitioner Faculties has passed, and nurse practitioners holding a Master of Science in Nursing remain fully licensed and certified to practice in every U.S. state. No state legislature enacted a law requiring a Doctor of Nursing Practice for nurse practitioner licensure. No certification body added a DNP as a prerequisite for examination or renewal.
Yet confusion persists. Working MSN-prepared NPs wonder whether their credentials will lose standing. Prospective students fear they are entering online MSN NP programs that may soon be obsolete. Many assume that the 2025 target was binding and that grandfathering protections have already gone into effect.
The reality is simpler and less dramatic. Professional organizations issued a recommendation. States did not follow through with legislation. The MSN remains the legal standard. Certified Registered Nurse Anesthetists face a mandatory DNP requirement, and that exception feeds the mistaken belief that all advanced practice nursing specialties are headed in the same direction.
What Was the 2025 DNP Deadline, and What Actually Happened?
Professional recommendation versus state law: these are fundamentally different mechanisms for changing the educational requirements for nurse practitioners, yet the two are often conflated when discussing the 2025 DNP deadline. Understanding this distinction is essential to making sense of where the profession stands today.
The Origin: A Vision from 2004
The story begins in 2004, when the American Association of Colleges of Nursing (AACN) issued a position statement recommending that the Doctor of Nursing Practice (DNP) become the entry-level degree for all advanced practice registered nurses (APRNs) by 2015.1 This was an aspirational goal set by a professional organization, not a piece of legislation or a regulatory mandate from state boards of nursing. The AACN believed that the increasing complexity of healthcare demanded more rigorous preparation at the doctoral level.
When 2015 arrived without widespread adoption, the National Organization of Nurse Practitioner Faculties (NONPF) took up the torch. In 2018, NONPF formally committed to the goal of DNP entry-to-practice for nurse practitioner practice by 2025.1 The organization reaffirmed this commitment in 2023 with a statement titled "DNP: Entry to Nurse Practitioner Practice by 2025."2 NONPF continued to invest in faculty development, launching initiatives such as the 2026 Competency-Based Education Workshop to support programs transitioning to the DNP model.3
What Actually Happened by 2025
As of early 2026, no state has enacted a DNP mandate for nurse practitioner licensure. The MSN remains the accepted entry-level degree for NPs nationwide. MSN-to-NP programs continue to enroll students, graduate cohorts, and prepare nurses for national certification exams. The professional organizations' timeline was always a recommendation to academic programs and accrediting bodies, not a directive to state legislatures or boards of nursing.
The one notable exception is certified registered nurse anesthetists (CRNAs). The Council on Accreditation of Nurse Anesthesia Educational Programs did successfully transition all entry-level CRNA programs to the doctoral level, and that requirement is now in effect. For nurse practitioners, however, the landscape remains unchanged from a regulatory standpoint.
Where the Professional Organizations Stand Now
Neither NONPF nor AACN has issued new timeline statements or revisions since January 2025. AACN's most recent DNP fact sheet, published in June 2025, continues to reference NONPF's 2025 goal and expresses support for the transition.1 NONPF has not publicly revised or abandoned its 2025 target, but it has also not announced a new deadline.2 The organizations appear to be taking a quieter, longer-term approach, focusing on competency-based education and program development rather than pressing for a new mandatory cutoff date. If you're weighing your options, you can explore best online DNP nurse practitioner programs to see what's available right now.
Is a DNP Legally Required for NP Licensure in Any State in 2026?
As of 2026, no U.S. state has enacted a law requiring a Doctor of Nursing Practice degree for nurse practitioner licensure.1 The Master of Science in Nursing remains sufficient for NP licensure in all fifty states, the District of Columbia, and U.S. territories. If you hold or are pursuing an MSN in a nurse practitioner specialty, you can obtain and maintain your license to practice anywhere in the country.
Current State-by-State Licensure Status
Several states have been the subject of recurring questions about potential DNP mandates, particularly New York, North Dakota, Montana, and Hawaii. Here's where they stand:
| State | DNP Required for NP Licensure (2026) | Current Status |
|---|---|---|
| New York | No | MSN remains acceptable; no announced licensure changes |
| North Dakota | No | MSN remains acceptable; no announced licensure changes |
| Montana | No | MSN remains acceptable; no announced licensure changes |
| Hawaii | No | MSN remains acceptable; no announced licensure changes |
| Indiana | No | Graduate degree in NP role and national certification required; no doctoral requirement |
| California | No | Graduate-level education required; no doctoral requirement |
| District of Columbia | No | MSN remains acceptable; no announced licensure changes |
No state board of nursing has implemented a doctoral degree requirement for initial licensure or license renewal.1 While some states have seen legislative proposals or task force discussions over the past several years, none have resulted in binding law.
Licensure Authority vs. Professional Recommendations
It's important to understand the distinction between who sets licensure requirements and who issues educational recommendations. State boards of nursing hold the legal authority to establish the minimum degree required for nurse practitioner licensure. These are government agencies, and their rules carry the force of law. If you're considering programs across state lines, it's worth reviewing how online NP programs for out-of-state students handle licensure variations.
Professional organizations, accrediting bodies, and nursing advocacy groups may recommend the DNP as the preferred terminal degree for advanced practice nurses, but their statements do not create legal requirements. When the American Association of Colleges of Nursing called for DNP preparation by 2015 and later extended that recommendation to 2025, those were aspirational goals, not mandates. Only state legislatures and nursing boards can change licensure law.
Bills Introduced and Task Forces Formed
Several states have seen DNP-related bills introduced in their legislatures or nursing workforce task forces convened to study the issue. To date, none of these efforts have resulted in a DNP mandate reaching the statute books. States that have publicly discussed the topic include New York, where bills have been introduced but not passed, and North Dakota, where legislative interest has surfaced periodically.
If you want to stay ahead of potential changes, consider using our NP health policy toolkit for practical steps on engaging with your state legislature. For any actual change to licensure requirements, your state board of nursing would announce it well in advance, typically with a multi-year implementation timeline and grandfathering provisions for currently licensed NPs.
Will MSN-Prepared Nurse Practitioners Be Grandfathered In?
Since no state currently mandates the DNP for nurse practitioner licensure, the question of grandfathering remains hypothetical, but the anxiety it generates among working NPs is very real. The good news: every meaningful precedent in nursing regulatory history points toward protection for nurses already in practice.
What the Hypothetical Actually Looks Like
Grandfathering is the legal mechanism that lets professionals who hold a credential before a new requirement takes effect continue practicing under the older standard. In nursing, this principle has been honored consistently. When the BSN-in-10 movement gained traction in New York, existing ADN and diploma nurses were protected. When advanced practice consensus models reshaped scope of practice across states, currently certified NPs were not asked to re-credential from scratch.
The pattern matters because it reflects a basic regulatory reality: states cannot easily strip licensure from tens of thousands of currently practicing clinicians without triggering workforce collapse and significant legal challenge.
The CRNA Transition as a Template
The most instructive precedent comes from nurse anesthesia. When the Council on Accreditation set the 2025 doctoral entry requirement for new CRNAs, it applied only to students entering programs after a specific date. CRNAs already certified through master's level education retained their credentials, kept their jobs, and continued recertifying through the National Board of Certification and Recertification for Nurse Anesthetists under existing pathways.
No CRNA was forced back to school. No employer was required to replace existing staff. The transition affected program structure, not practicing clinicians.
What Every Proposed DNP Bill Has Included
In the nearly two decades since the AACN first recommended the DNP as entry to advanced practice, no state legislature or board of nursing has proposed decertifying existing MSN-prepared NPs. Every draft policy, position statement, and stakeholder proposal has included grandfathering language. The political and practical cost of doing otherwise is simply too high.
Your Best Protection Right Now
If you want to insulate yourself from any future regulatory shift, the answer is straightforward:
- Keep your national certification active and in good standing through your certifying body (AANP, ANCC, or specialty board).
- Maintain continuous active clinical practice, including the required practice hours for recertification.
- Document your continuing education consistently.
Nurses who stay certified and clinically active have historically been the first protected when standards evolve. For a deeper look at what those credentials involve, review our nurse practitioner licensing guide. That is the lever you control today, regardless of what any state board decides tomorrow.
Questions to Ask Yourself
The Exception: CRNA DNP Requirements Explained
While nurse practitioners continue operating under a voluntary framework for doctoral education, one advanced practice nursing specialty has successfully implemented a binding DNP mandate. Certified Registered Nurse Anesthetists now face a clear requirement: as of January 1, 2025, anyone entering nurse anesthesia practice must hold a doctoral degree.1
What the CRNA Mandate Actually Requires
The Council on Accreditation of Nurse Anesthesia Educational Programs made this change enforceable by setting firm deadlines. All nurse anesthesia programs were required to transition to doctoral-level curricula by January 1, 2022, and the COA stopped accrediting new master's-level programs back in 2015.2 Students matriculating after January 2022 must enroll in a doctoral program, with either a Doctor of Nursing Practice or a Doctor of Nurse Anesthesia Practice satisfying the requirement.2
This is not a recommendation or a professional aspiration. It is an accreditation standard with teeth.
How Existing CRNAs Are Protected
If you earned your CRNA credential through a master's program before these deadlines, you can continue practicing without obtaining a doctorate.3 The profession explicitly grandfathered existing practitioners, recognizing that forcing tens of thousands of working clinicians back to school would be neither practical nor fair. Optional MSN-to-doctoral completion programs exist for those who want to upgrade their credentials, but participation remains voluntary for master's-prepared CRNAs.2
Why CRNAs Succeeded Where NPs Have Not
The nurse anesthesia profession achieved what has eluded nurse practitioners for over a decade. Three structural factors made the difference:
- Single accrediting body: The COA is the sole accreditor for all nurse anesthesia programs nationwide, giving it unified authority to set and enforce standards.
- One professional organization: The American Association of Nurse Anesthesiology has represented CRNAs since 1931 and formally endorsed doctoral entry back in 2007, creating consistent messaging and political will.3
- Smaller practitioner pool: With approximately 60,000 CRNAs compared to over 350,000 nurse practitioners, the profession could coordinate change more efficiently.
The Lesson for Nurse Practitioners
The NP landscape looks nothing like this. Nurse practitioners span dozens of specialties, from family practice to psychiatric care to acute care vs primary care subspecialties. Multiple certification bodies govern different populations. Fifty state boards of nursing maintain independent licensing authority. No single organization can mandate anything for the entire profession.
This fragmentation explains why the 2025 deadline came and went without enforcement. It also suggests that any future NP doctoral requirement would likely emerge state by state or specialty by specialty rather than through a single national mandate. For nurses weighing a DNP or MSN pathway, CRNAs provide a successful model of how a mandate can work, but replicating their approach across the NP profession would require unprecedented coordination among competing stakeholders.
DNP Vs. MSN for Adult-Gerontology Acute Care NPs (AGACNP)
Adult-gerontology acute care nurse practitioners work in some of the most demanding clinical environments in healthcare, and many practicing RNs wonder whether a doctoral degree is now mandatory to enter the specialty.
Is a DNP Required for AGACNP Certification?
No. The American Nurses Credentialing Center (ANCC), which administers the AGACNP-BC certification exam, continues to accept both master's-prepared and doctoral-prepared candidates in 2026.1 ANCC has not announced any plan to require the DNP for AGACNP certification, meaning you can sit for the exam with either an MSN or DNP from an accredited program. This stands in contrast to the CRNA specialty, where doctoral preparation became mandatory in 2025.
Comparing the MSN and DNP Pathways
Both pathways prepare you for the same national certification exam and the same clinical role, but they differ in scope and time commitment:
- Program length: MSN programs typically require 18 to 24 months of full-time study, while entry-level DNP programs (BSN to DNP) span three to four years. Post-master's DNP programs for practicing NPs generally take two years part-time.
- Clinical hours: ANCC requires a minimum of 500 supervised clinical hours for AGACNP certification, a standard both MSN and DNP programs meet.1 Many DNP programs exceed this minimum, often reaching 1,000 hours or more by graduation.
- Curriculum: Both degrees cover advanced physiology, pathophysiology, health assessment, and pharmacology. DNP programs add courses in evidence-based practice, healthcare policy, systems leadership, and a scholarly practice project.
- Certification eligibility: Identical. Graduates of either degree sit for the same ANCC AGACNP-BC exam.
Employer Preferences in Acute Care Settings
Most hospitals and health systems accept MSN-prepared AGACNPs for bedside and unit-based positions.2 However, academic medical centers, Magnet-designated hospitals, and institutions with teaching missions increasingly prefer or explicitly seek DNP-prepared candidates for clinical leadership roles, residency preceptor positions, and quality-improvement initiatives. A 2024 survey of acute care NP hiring managers found that 68 percent of large academic hospitals expressed a preference for DNP credentials when choosing between otherwise equal candidates, though only 12 percent required it outright.
If your career goals center on direct patient care in ICUs, step-down units, or emergency departments, an MSN remains a fully viable and more affordable entry point. You can explore acute care nurse practitioner programs online to compare options side by side. If you envision leading clinical teams, shaping hospital protocols, or transitioning into administrative or academic roles, DNP AGACNP programs may offer a competitive advantage and align better with long-term goals. Nurses already holding an MSN who want to add the AGACNP focus can also look into an AGACNP post-master's certificate online.
Related Articles
How Certification Bodies and Accreditors Are Handling the Transition
Both the American Association of Colleges of Nursing and the National Organization of Nurse Practitioner Faculties hold prominent roles in shaping NP education, yet neither entity can legally mandate degree requirements for licensure. Understanding who does what helps you separate headline anxiety from actual career impact.
Accreditors vs. Professional Organizations vs. Certification Bodies
The nursing landscape involves several distinct entities, each with different authority:
- AACN (American Association of Colleges of Nursing): Accredits nursing programs at colleges and universities. AACN's 2021 Essentials framework guides how schools design curricula, but it does not set licensure rules.
- NONPF (National Organization of Nurse Practitioner Faculties): A professional organization that establishes recommended competencies for NP education. NONPF endorsed the 2025 DNP goal, but endorsements carry no regulatory weight.
- ANCC and AANP: These are the two primary certification bodies for nurse practitioners. They administer the exams that allow NPs to become certified in their specialty populations.
- State Boards of Nursing: The only entities with legal authority to determine what degree is required for NP licensure in a given state.
What the 2021 AACN Essentials Actually Changed
AANC's updated Essentials framework focuses on competency-based education rather than prescribing a specific terminal degree. Schools accredited under this framework must demonstrate that graduates meet defined competencies, whether the program confers an MSN or DNP. For a deeper look at how accrediting bodies like ACEN and CCNE evaluate programs, see our nursing accreditation guide. Importantly, this framework applies to newly developed or revised curricula going forward. It does not retroactively alter the credentials of nurses who graduated under previous standards, nor does it touch licensure requirements.
Certification Remains Open to MSN Graduates
As of 2026, both ANCC and AANP continue to certify graduates of accredited MSN programs. Neither organization has announced a sunset date for MSN certification eligibility. If you complete an accredited MSN NP program and pass the appropriate certification exam, you earn the same credential as a DNP graduate sitting for that same exam.
Only State Legislatures Can Mandate Degree Requirements
Professional organizations can publish position statements, and accreditors can update educational standards, but only state legislatures and boards of nursing hold the legal authority to require a specific degree for licensure. As of mid-2026, no state has enacted legislation mandating a DNP for initial NP licensure. The gap between professional recommendations and legal mandates is where much of the confusion originates. If you are still mapping out the steps to enter practice, our overview of how to become a nurse practitioner walks through each milestone. When you hear that a DNP is "required," always verify whether the source is a professional organization expressing a goal or a state board enacting a binding rule.
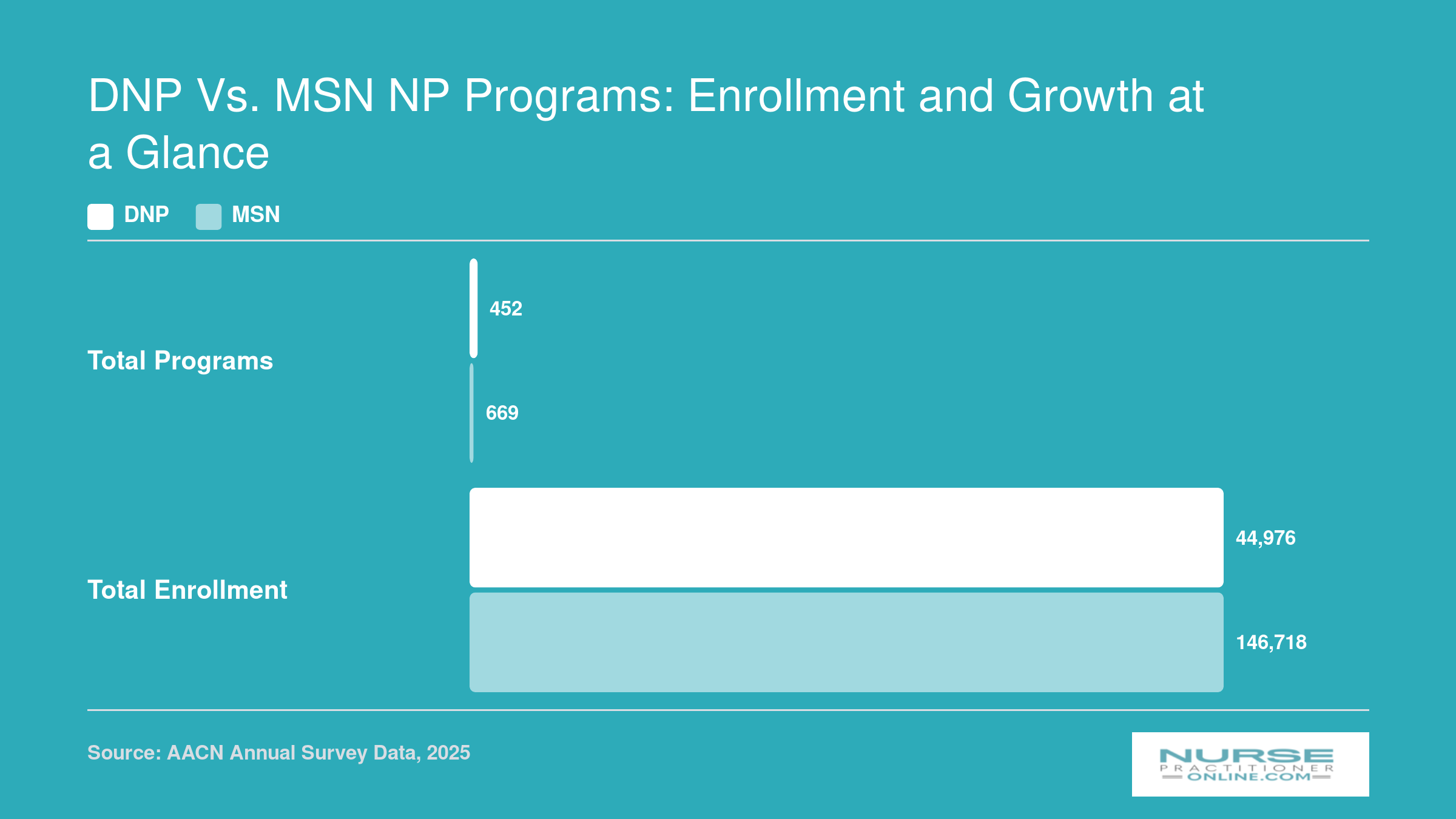
DNP Vs. MSN NP Programs: Enrollment and Growth at a Glance
Despite years of debate over a potential DNP mandate, MSN programs continue to enroll far more nurse practitioner students than DNP programs. Both program types are growing, and the data makes one thing clear: MSN education is not being phased out.
MSN-To-DNP Pathway: What It Takes in 2026
An MSN-to-DNP bridge in 2026 is a 30- to 45-credit, two-to-three-year part-time commitment built around your existing NP practice, not a return to full-time student life. It exists to layer doctoral-level systems, leadership, and translational science onto the clinical foundation you already have. Whether you pursue it is a career investment decision, not a licensure mandate.
Credits, Clinical Hours, and the Scholarly Project
Most MSN-to-DNP programs require somewhere between 30 and 45 additional credits on top of your master's degree. Texas Woman's University, for example, structures its bridge at 40 credits, while UAB sits at 43.23 The clinical hour requirement depends on what you completed during your MSN: AACN expects DNP graduates to finish a total of 1,000 post-baccalaureate supervised hours, so bridge programs typically add 500 to 540 hours to close that gap.2 Texas Woman's adds 540; UAB adds 500.
Every program culminates in a DNP scholarly project, a practice-focused initiative addressing a real problem in your clinical setting: quality improvement, policy analysis, or implementation of evidence-based change.
Timeline and Format
Plan on 24 to 36 months part-time. Purdue Global runs a 24-month track; UAB ranges from 24 to 36 depending on pace.43 The format is overwhelmingly online or hybrid, with Texas Woman's, UAB, and Purdue Global all delivering coursework at a distance and allowing clinical hours and project work to happen in your own community. That accessibility is the whole point: these programs are designed for nurse practitioners who are already employed and want to advance without relocating or stepping away from practice. If you are weighing different DNP concentrations, our comparison of best online DNP FNP programs can help narrow the search.
Admission generally requires a 3.0 GPA, an active RN and APRN license, and a current MSN from an accredited program.5 GRE waivers have become standard, including at the University of Florida.5
Cost and Funding
Per-credit tuition varies widely. Purdue Global runs around $420 per credit; UAB sits near $723.43 Total program cost nationally lands roughly between $25,000 and $80,000. Three funding levers are worth pursuing: employer tuition assistance (common at hospital systems wanting doctorally prepared clinicians), HRSA's Nurse Faculty Loan Program and Advanced Nursing Education awards for those interested in academic or underserved-population roles, and federal Grad PLUS loans for the balance.
In 2026, the DNP is a voluntary credential. Choose it because it opens doors, not because a deadline forced you.
Making Your Decision: MSN or DNP in 2026?
Choosing between an MSN and a DNP is one of the biggest decisions you will face as a working nurse exploring the NP path. Rather than letting anxiety about a future mandate drive your choice, use this practical breakdown to weigh what each degree offers right now and where each one could leave you in the years ahead.
Pros
- The MSN path is typically faster (two to three years) and significantly less expensive, making it accessible for nurses balancing work and family obligations.
- An MSN is fully sufficient for NP licensure and national certification in every U.S. state as of 2026, with no legal barriers to practice.
- The DNP positions graduates for leadership, health policy, and academic faculty roles that increasingly list a doctoral degree as preferred or required.
- A DNP may offer long term career flexibility if professional organizations or states eventually adopt doctoral entry requirements.
- DNP graduates often complete a scholarly project with direct clinical impact, building expertise that can set them apart in competitive healthcare systems.
Cons
- MSN holders face some uncertainty: if a state or certification body mandates the DNP in the future, they may need to return to school later at additional cost.
- A growing number of academic medical centers and large health systems list the DNP as preferred, which could affect hiring competitiveness for MSN prepared NPs over time.
- The DNP adds one to two extra years of study and tens of thousands of dollars in tuition, with little immediate difference in scope of practice or prescriptive authority compared to the MSN.
- DNP graduates do not consistently earn higher salaries than MSN prepared NPs in the same clinical role, so the return on investment is not guaranteed.
- Pursuing a DNP while working full time can strain finances and personal life, and the opportunity cost of delayed earning potential is real.
Frequently Asked Questions About the DNP Requirement
These are some of the most common questions working nurses ask when weighing whether to pursue a DNP. Each answer reflects where things actually stand in 2026, not where people assumed they would be a few years ago.
- When will a DNP be required for nurse practitioners?
- As of 2026, no state requires a DNP for nurse practitioner licensure. The AACN recommended the DNP as the entry level for advanced practice by 2025, but that was a professional aspiration, not a legal mandate. No federal or state legislation currently sets a firm date for a universal DNP requirement, and the timeline remains uncertain.
- Will MSN nurse practitioners be grandfathered in if a DNP becomes required?
- Most professional organizations and accrediting bodies have signaled that MSN-prepared NPs already in practice would be grandfathered under any future DNP mandate. Historically, nursing transitions (such as the shift from diploma to BSN) have protected currently licensed practitioners. However, because no binding requirement exists yet, specific grandfathering language has not been written into law.
- Is a DNP required for AGACNP certification?
- No. In 2026, both the ANCC and AACN allow MSN-prepared nurses to sit for Adult-Gerontology Acute Care NP certification. MSN-level AGACNP programs remain accredited and widely available. A DNP may offer career advantages in academic medical centers, but it is not a certification prerequisite at this time.
- Are MSN nurse practitioner programs being phased out?
- MSN NP programs are not being phased out. Some universities have shifted their NP tracks exclusively to the DNP, but hundreds of accredited MSN NP programs continue to enroll students and produce graduates. Both degree pathways lead to the same NP certification and licensure, so the MSN remains a fully viable route into practice.
- What states require a DNP for nurse practitioner licensure?
- No state requires a DNP for NP licensure in 2026. Every state board of nursing accepts MSN-prepared graduates for NP licensing. Periodic legislative proposals surface in various states, but none have passed. Always check your state board's current requirements before making enrollment decisions.
- What is the difference between a DNP and an NP?
- An NP (nurse practitioner) is a clinical role and a license. A DNP (Doctor of Nursing Practice) is a doctoral degree. You can become an NP with either an MSN or a DNP. The DNP adds coursework in systems leadership, evidence-based practice, and quality improvement, but the clinical scope of practice for NPs is determined by licensure, not degree level.
- Do I need a DNP to get a raise or promotion as an NP?
- Not necessarily. Many employers base NP compensation on experience, specialty certification, and productivity rather than degree level. That said, some health systems and academic institutions offer higher pay or leadership opportunities to DNP-prepared NPs. If your goal is a specific role, such as clinical director or faculty, research the actual requirements at organizations you are targeting before committing to a doctoral program.