Most important takeaways…
- Loretta Ford and Henry Silver launched the first nurse practitioner program at the University of Colorado in 1965.
- A 1960s physician shortage, especially in rural and underserved areas, drove creation of the NP role.
- The NP workforce has grown from fewer than 100 clinicians in 1965 to over 461,000 licensed practitioners today.
- NP education evolved from four-month certificate programs to master's and doctoral degrees required for practice.
More than 400,000 nurse practitioners now practice in the United States, delivering over one billion patient visits every year and serving as primary care providers for millions of Americans. That workforce did not emerge from policy committees or medical school expansions. It was built, from the ground up, by women who saw a gap in care and designed a new kind of clinician to fill it.
The nurse practitioner role began in 1965 when Loretta Ford, a public health nurse with a doctorate in education, partnered with pediatrician Henry Silver to launch the first formal NP program at the University of Colorado. What started as a four-month pilot has since grown into a profession with graduate-level education, state-by-state scope-of-practice battles, and a transition from certificate programs to doctoral degrees.
This article traces that arc: the 1965 origin, the nurse practitioner visionaries whose scholarship and advocacy expanded the role, the legislative fights that secured independent practice authority in some states but not others, and the educational evolution that turned a clinical experiment into a cornerstone of American primary care.
When Did Nurse Practitioners Start? The Origin Story
Nurse practitioners began in 1965 at the University of Colorado, where pediatric nurse Loretta Ford and physician Henry Silver launched the first formal nurse practitioner program.1 That pilot program marked the birth of a profession that now, more than 60 years later, has grown from a handful of public health nurses into the largest group of primary care providers in the United States.
A Pediatric Demonstration Project in Rural Colorado
The original 1965 program was not a degree track or even a lengthy certificate. Ford and Silver designed a compact, intensive training program lasting three to four months, specifically for experienced public health nurses.2 The curriculum focused squarely on preventive child health and well-child care, addressing a critical shortage of pediatric primary care in rural Colorado communities.3 With just $7,000 in initial funding, the project was a lean, pragmatic experiment aimed at demonstrating that registered nurses with advanced training could safely and effectively expand access to pediatric health services.2
The first cohort completed the program within the same academic year it began, and the model proved so successful that by 1972, 64 nurses had graduated from the University of Colorado pediatric nurse practitioner certificate program.2 The concept was controversial at the outset, challenging traditional boundaries between medicine and nursing, yet the outcomes spoke for themselves: nurses were delivering high-quality preventive care, freeing physicians to focus on more complex cases, and improving health outcomes in underserved areas.
Why 1965 Is the Accepted Origin Date
Earlier advanced-practice nursing experiments existed, most notably Thelma Ingles's clinical nurse specialist work at Duke in the 1950s. However, 1965 marks the first structured, formalized nurse practitioner role with a defined curriculum, clinical competencies, and a clear scope of practice centered on independent assessment, diagnosis, and management of common health conditions. Ford and Silver's program created a replicable template that other universities quickly adopted. By 1967, Boston College had launched its own nurse practitioner program, and the movement gained unstoppable momentum.4
Today, with more than 400,000 licensed nurse practitioners nationwide, the profession has matured far beyond its rural Colorado roots. If you're curious about the nurse practitioner visionaries who carried that momentum forward, their stories build directly on the foundation Ford and Silver laid in 1965: extend the reach of quality primary care by empowering nurses with advanced training and clinical autonomy.
Why Were Nurse Practitioners Created?
Treat the physician shortage of the 1960s as a policy failure and you get one response: train more doctors. Treat it as an opportunity to rethink who delivers care and you get the nurse practitioner. The people who built the NP profession chose the second path, and that choice changed American healthcare permanently.
A Nation Short on Doctors
By the mid-1960s, large stretches of rural America and most low-income urban neighborhoods had no reliable access to a primary care physician. Families went without well-child visits, chronic conditions went unmanaged, and preventable illnesses became emergencies. The problem was especially acute for children and for communities with little economic or political power. Training new physicians was not a realistic short-term answer: the pipeline from undergraduate preparation through residency ran well beyond a decade, and new graduates rarely chose to practice in the communities that needed them most.
Medicare, Medicaid, and a Widening Gap
The 1965 passage of Medicare and Medicaid made the access crisis visible in numbers. Suddenly, millions of Americans who had previously gone without care held coverage cards and needed somewhere to use them. Demand surged. The supply of primary care providers did not. Policymakers and clinicians alike began asking whether the healthcare system's traditional division of labor still made sense when the math so clearly did not work.
Loretta Ford's Practical Insight
Nurse Loretta Ford recognized something that the physician-training pipeline could not offer: nurses were already doing much of the clinical groundwork. They performed assessments, educated patients, monitored chronic conditions, and coordinated care. Formalizing an expanded scope of practice would not require inventing a new professional from scratch. It would mean building on preparation that experienced nurses already had, and it could reach underserved populations within years rather than decades. Working alongside pediatrician Henry Silver at the University of Colorado, Ford translated that insight into a structured educational program. Today, the question of whether a nurse practitioner can be a primary care provider has a clear answer rooted in that original vision.
A Social Moment That Demanded New Models
The creation of the NP role did not happen in a vacuum. The civil rights movement was dismantling the idea that unequal access to basic services was acceptable. The War on Poverty was funding community health centers designed to bring care directly into underserved neighborhoods. Those centers needed clinicians willing to work in communities that traditional medicine had overlooked. The NP was, in a real sense, a product of that social pressure: a practical answer to a moral question about who deserved quality healthcare and who was qualified to provide it. That same spirit of advocacy continues to shape nurses in politics and health policy today.
Loretta Ford and Henry Silver: Founders of the First NP Program
The first nurse practitioner program was the product of an unusual partnership: a public health nurse with a doctorate in education and a pediatrician who believed nurses could safely manage much of the well-child care his colleagues were too stretched to deliver. Together at the University of Colorado Medical Center in 1965, Loretta Ford and Dr. Henry Silver designed a clinical training model that would reshape primary care for the next sixty years.1
Loretta Ford: A Nurse's Vision of Expanded Practice
Ford came to the project through years of public health nursing in rural Colorado, where she watched families go without basic pediatric care because no physician was available. She held a PhD in education, and she was clear-eyed about what she was building. The nurse practitioner, in her view, was an autonomous nursing role grounded in nursing science, not a junior physician or a stand-in for one. Her now-famous framing was that NPs are "maxi nurses, not mini doctors," and she repeated throughout her career that the role was never meant to substitute for physicians.2 It was meant to extend nurse practitioner scope of practice into assessment, diagnosis, and management of common conditions.
Her influence did not end in Colorado. In 1972, Ford became the founding Dean of the University of Rochester School of Nursing and concurrently served as Director of Nursing at Strong Memorial Hospital.3 There she developed the unification model, which integrated education, research, and clinical practice under a single academic structure. She published well over a hundred papers, served as a visiting professor at institutions including St. Luke's College of Nursing in Japan, the University of Washington, and the University of Florida, and was named a Living Legend by the American Academy of Nursing.4 She retired in 1986 but continued advocating for DNP entry-to-practice decades before the DNP became the field's preferred terminal degree.
Henry Silver: The Physician Partner
Silver was a pediatrician at the University of Colorado who saw collaborative, team-based care as the practical answer to a primary care shortage. His partnership with Ford modeled what nurse-physician collaboration could look like in training and in practice, and he later founded the country's first physician assistant program in 1968, drawing on what he and Ford had learned together.2
From Pediatric Roots to Family Practice
The original Colorado program was explicitly pediatric, focused on well-child care, developmental screening, and management of common childhood illness. But Ford's longer vision was always family-centered primary care across the lifespan. That vision took shape through the 1970s as family nurse practitioner tracks emerged at programs around the country, building directly on the pediatric foundation Ford and Silver had laid.
Other Women Who Shaped the NP Profession
What other women contributed to the nurse practitioner profession beyond the well-known Dr. Loretta Ford? The NP movement was never a solo effort. A network of nurse scholars, researchers, and policy advocates built the foundation for advanced practice nursing as we know it today. Each added a critical piece to the puzzle.
Harriet Kitzman: Building the Research Base
Harriet Kitzman, a distinguished professor and senior associate dean for research at the University of Rochester School of Nursing, co-led one of the earliest pediatric nurse practitioner programs alongside Dr. Ford.1 Together, they designed a curriculum that proved NPs could deliver safe, effective primary care, and Kitzman ensured it was backed by rigorous evidence. Over her career, she published more than 100 peer-reviewed articles, 17 book chapters, and 14 proceedings, with her most recent study appearing in 2019, just a year before her death in March 2020 at age 82.2 Her leadership extended to directing the Center for Research Implementation and Translation, and she was instrumental in securing federal funding in 1996 for the Nurse-Family Partnership, a home-visiting program that now serves 38,000 families annually across 41 states.3 Kitzman's ability to translate research into real-world health improvements validated the NP role in pediatric and community settings.
Barbara Safriet: Tearing Down Legal Barriers
While clinicians built programs, legal scholar Barbara Safriet removed the obstacles that kept NPs from practicing. As associate dean and lecturer at Yale Law School, she published a 1992 article titled "Health Care Dollars and Regulatory Sense: The Role of Advanced Practice Nursing" in the Yale Journal on Regulation.4 The article dismantled arguments for restrictive scope-of-practice laws and made an economic and patient-safety case for full practice authority. Safriet's work became a cornerstone of the Institute of Medicine's Future of Nursing reports, influencing policy changes that eventually expanded NP autonomy in dozens of states. Her writing gave state legislators and advocacy groups the intellectual ammunition to overturn outdated regulations, proving that legal scholarship could be as powerful as a stethoscope.
Thelma Ingles: A Precursor at Duke
Before the first NP program launched, Thelma Ingles was already experimenting with advanced clinical training for nurses at Duke University School of Nursing. In the late 1950s, she created a program intended to prepare nurses for expanded patient-care responsibilities, a direct forerunner to the NP role. Though the program was denied accreditation and didn't survive, it influenced Ford's thinking and demonstrated the viability of nurses managing chronic conditions. Ingles collaborated with physician E. Harvey Estes, showing the interdisciplinary teamwork that would later define NP practice. Her work reminds us that innovation often precedes formal recognition.
Hildegard Peplau: Theory for Psychiatric NPs
Hildegard Peplau's contribution was more theoretical but equally essential. Her interpersonal relations theory, developed in the 1950s, provided the clinical framework for psychiatric-mental health nursing. When the psychiatric NP specialty later emerged, it was built on Peplau's concepts of nurse-patient interaction as a therapeutic process.
These women, alongside many others, formed a chain of mentorship and mutual influence. From Ingles' early experiments to Kitzman's research, Safriet's policy victories, and Peplau's theoretical grounding, the NP profession evolved through their collective effort, not a single flash of insight but a sustained, collaborative campaign.
Related Articles
NP Timeline: Key Milestones From 1965 to Today
Some professions trace their history through dramatic single moments; the nurse practitioner role grew through steady, decade-by-decade legal and educational wins. Mapping those wins side by side reveals how a small Colorado pilot grew into a 400,000-strong workforce reshaping primary care.
The Founding and Early Growth Era (1965 to 1979)
The NP story begins in 1965, when Dr. Loretta Ford and Dr. Henry Silver launched the first nurse practitioner educational program at the University of Colorado.1 The pediatric focus reflected an urgent shortage of primary care for children, particularly in rural communities. Within a few years, family-focused training emerged at other universities, planting the seeds of the FNP specialty that would later become the largest NP track. In 1971, Idaho became the first state to formally recognize the NP role and title in statute, giving the profession its first foothold in law.2 The rest of the decade was spent building curricula, certifying early graduates, and convincing skeptical physicians and regulators that NPs could safely deliver primary care.
Legitimization and Prescriptive Authority Battles (1980 to 1999)
The 1980s and 1990s were defined by state-by-state fights over prescribing rights and reimbursement. The Omnibus Budget Reconciliation Act of 1989 cracked open the federal door, granting limited Medicare reimbursement for NP services in specific settings such as rural and nursing-home care.1 In 1994, Alaska, Iowa, Montana, New Mexico, and Oregon became the first cluster of states to grant full practice authority, letting NPs evaluate, diagnose, and treat without physician supervision.2 The defining federal milestone arrived with the Balanced Budget Act of 1997, which authorized direct Medicare reimbursement for NPs regardless of geographic setting.1 That single change transformed the economic viability of the role and accelerated FNP hiring across primary care practices nationwide.
Full Practice Authority Expansion (2000 to Present)
The 2000s shifted the focus from billing to scope of practice. State after state revisited supervision requirements, and FNPs (the largest specialty) often led the policy conversations because they practice in the settings most affected: primary care, retail clinics, and rural health. You can track the current landscape in our guide to full practice authority states. Utah granted full practice authority in March 2023, bringing the total to 27 states.2
Milestone Table
- 1965: First NP program launched at the University of Colorado by Ford and Silver.1
- 1971: Idaho becomes the first state to formally recognize the NP role.2
- 1989: OBRA grants limited Medicare reimbursement for NP services.1
- 1994: Alaska, Iowa, Montana, New Mexico, and Oregon adopt full practice authority.2
- 1997: Balanced Budget Act authorizes direct Medicare reimbursement for NPs.1
- 2023: Utah becomes the 27th full practice authority state.2
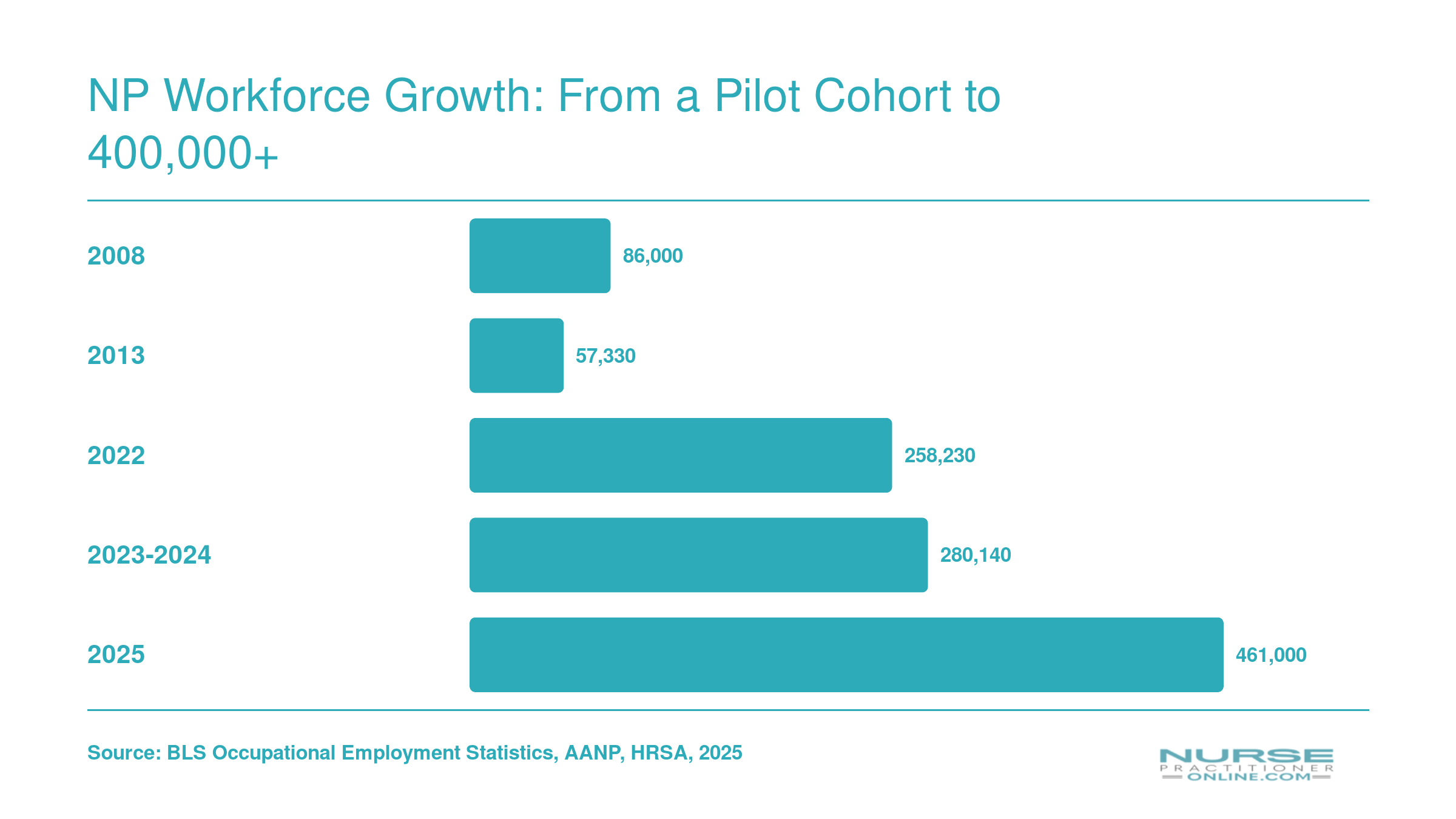
The nurse practitioner workforce has grown from fewer than 100 clinicians in 1965 to more than 461,000 licensed NPs today, according to the American Association of Nurse Practitioners. That's a more than 4,600-fold increase in just six decades, making NPs one of the fastest-growing healthcare professions in American history.
NP Workforce Growth: From a Pilot Cohort to 400,000+
What began as a single pilot cohort in 1965 has grown into one of the fastest-expanding healthcare professions in the country. The chart below highlights key workforce milestones using employment and licensure figures reported by the Bureau of Labor Statistics and the American Association of Nurse Practitioners.
How NP Education Evolved: Certificates to DNP
Nurse practitioner education has traveled a long road from the four-month certificate Loretta Ford and Henry Silver awarded in 1965 to the rigorous graduate programs and clinical doctorates common today. That evolution reflects the profession's steady climb toward legitimacy, standardization, and parity with other advanced-practice health professions.
The Certificate Era (1965, 1970s)
The first NP programs were short, hospital-based continuing-education certificates. Nurses with a bachelor's degree (or, in some cases, a diploma) could complete a concentrated curriculum in pediatric assessment and management and emerge as nurse practitioners. These early programs lacked uniform admission requirements, credit hours, or accreditation. While they proved the concept and trained the pioneers, the lack of standardization made it difficult to compare graduates' competencies or win acceptance from skeptical physicians and state boards of nursing.
The Shift to Master's Preparation (1970s, 1990s)
By the late 1970s, nursing education leaders began requiring a master's degree for entry into NP practice. The rationale was twofold: master's-level preparation aligned nurse practitioners with other advanced-practice nurses (clinical nurse specialists, nurse-midwives, nurse anesthetists) and signaled professional parity with physician assistants and other master's-prepared clinicians. Accreditation bodies emerged to enforce curriculum standards, and by the 1990s the master of science in nursing with an NP specialty track became the accepted entry credential. Today, this remains the minimum standard for NP licensure and certification. If you're considering this path, our guide on how to become a nurse practitioner walks you through each step.
The DNP Movement (2004, Present)
In 2004, the American Association of Colleges of Nursing issued a position statement calling for the doctor of nursing practice as the terminal degree for all advanced-practice roles by 2015. The goal was to bring nursing in line with pharmacy (PharmD) and physical therapy (DPT), both of which had adopted clinical doctorates. While the 2015 deadline passed without a mandate, DNP programs have proliferated. For a closer look at where the profession stands today, see our analysis of current status DNP requirement for nurse practitioners. Many schools now offer MSN-to-DNP bridge tracks for practicing NPs, and a growing number of entry-level DNP programs admit BSN graduates directly into doctoral study.
Family Nurse Practitioner: The Core of NP Education
Throughout these transitions, the family nurse practitioner specialty has remained the most popular track, enrolling roughly 65 to 70 percent of all NP students. This dominance is a direct echo of Loretta Ford's original vision: preparing nurses to deliver primary care across the lifespan, especially in underserved communities. FNP graduates can work in family practices, urgent care, school health, and rural clinics, making the specialty both versatile and in high demand.
Accreditation and Certification: The Quality Gatekeepers
Today, NP programs must earn accreditation from the Commission on Collegiate Nursing Education or the Accreditation Commission for Education in Nursing. Graduates sit for national certification exams administered by the American Academy of Nurse Practitioners Certification Board or the American Nurses Credentialing Center. These gatekeepers enforce curriculum standards, clinical-hour minimums, and competency assessments that the early certificate programs could not. The result is a profession with clear benchmarks, portability across state lines, and the credibility to advocate for full practice authority.
Questions to Ask Yourself
How Nurse Practitioners Transformed Healthcare Access
Nurse practitioners now deliver over one billion patient visits annually and serve as the primary care provider for millions of Americans, especially in rural and underserved areas where physicians are scarce.1 This staggering reach reflects how deeply NPs have reshaped healthcare delivery since the profession's inception.
A Billion Patient Visits and Counting
In 2025, NPs provided an estimated one billion patient visits across the United States, according to the American Association of Nurse Practitioners.1 Their role has become indispensable in primary care, with many patients relying on NPs for routine check-ups, chronic disease management, and acute care. In rural and underserved regions, NPs often stand as the sole consistent healthcare provider, bridging gaps that have persisted for decades.
Full Practice Authority in 2026: 27 States and Growing
As of 2026, twenty-seven states and Washington, D.C., grant NPs full practice authority, meaning they can diagnose conditions, order and interpret tests, and prescribe medications without a supervising physician.2 Another twelve states maintain reduced practice, requiring collaborative agreements, while eleven states still impose restricted practice, mandating direct physician oversight.3 The trend toward full authority has accelerated, driven by overwhelming evidence of NP competency and the pressing need to expand healthcare access.
Connecting Today's Expansion to the 1965 Vision
The same access gaps that motivated Loretta Ford in rural Colorado in 1965 are propelling today's regulatory changes. During the COVID-19 pandemic, temporary emergency waivers demonstrated that NPs could safely practice independently, prompting several states to permanently adopt full practice authority. This shift directly addresses the mission Ford and Henry Silver launched: delivering high-quality care to communities that lack sufficient physician coverage. Today, the expanding role of nurse practitioners continues to open new pathways for career growth and patient impact.
Research Confirms Equivalent Quality of Care
A landmark 2018 Cochrane systematic review by Laurant and colleagues concluded that NP-provided care leads to similar or better patient outcomes compared to physician care, including blood pressure control, patient satisfaction, and mortality rates.4 Earlier, Newhouse and co-authors reviewed 28 studies from 1990 to 2008 and found no significant differences in quality measures.4 These rigorous analyses have dismantled long-standing skepticism and paved the way for NPs to practice at the top of their education and clinical training.
Becoming a Nurse Practitioner Today
The pathway to becoming a nurse practitioner has grown more accessible than ever, with online programs now allowing working nurses to advance their careers without leaving the bedside. What began as a single pilot program at the University of Colorado has evolved into a well-defined educational ladder that welcomes nurses from diverse backgrounds and clinical settings.
The Modern NP Pathway
Today's aspiring nurse practitioners follow a structured route that builds on their nursing foundation:
- BSN completion: Most NP programs require a Bachelor of Science in Nursing as the entry point.
- RN licensure: Candidates must hold an active registered nurse license.
- Clinical experience: Programs typically expect one to two years of bedside nursing practice.
- Graduate education: Students complete either a Master of Science in Nursing or a Doctor of Nursing Practice with NP specialization.
- National certification: Graduates sit for board exams through organizations like the ANCC or AANP.
- State licensure: Final approval comes from the state board of nursing where the NP plans to practice.
MSN programs generally take two to three years to complete, while post-BSN DNP tracks run three to four years. Many institutions now offer these programs fully online, with clinical rotations arranged in the student's local community. For nurses weighing the doctoral route, understanding DNP prerequisites early can help streamline the application process.
The FNP Legacy Continues
Among all NP specialties, the Family Nurse Practitioner track remains the most popular and versatile choice. This is no coincidence. FNP students today are direct inheritors of Loretta Ford's original vision: primary care providers trained to serve patients across the lifespan, from newborns to older adults. The comprehensive scope that made Ford's 1965 graduates so valuable in underserved communities now makes FNP certification appealing to employers in clinics, hospitals, retail health settings, and telehealth platforms alike.
A Career Built on Historic Foundations
The profession these pioneering women built now represents one of the fastest-growing, highest-impact career paths in American healthcare. The Bureau of Labor Statistics projects continued strong demand for nurse practitioners through the coming decade, driven by physician shortages, an aging population, and expanding scope-of-practice laws. For nurses curious about how long it takes to become a nurse practitioner, exploring MSN-FNP and DNP program options opens the door to a career shaped by six decades of advocacy, research, and patient-centered care.
Frequently Asked Questions About NP History
The nurse practitioner profession has a rich history rooted in innovation and a commitment to expanding healthcare access. Below are answers to the most common questions about how, when, and why the NP role came to be.
- When did nurse practitioners start?
- Nurse practitioners started in 1965, when the first NP program was established at the University of Colorado. Dr. Loretta Ford and Dr. Henry Silver developed the program to train pediatric nurse practitioners who could deliver primary care in underserved communities. The concept grew rapidly through the late 1960s and 1970s as more universities launched their own programs.
- Who was the first nurse practitioner?
- The first nurse practitioners were graduates of the University of Colorado's pediatric NP program in the mid 1960s. While no single individual is credited as "the first NP," Dr. Loretta Ford is widely recognized as the founder and driving force behind creating the role. She envisioned nurses practicing at an advanced level to fill critical gaps in primary care.
- Why were nurse practitioners created?
- Nurse practitioners were created to address a severe shortage of primary care physicians, especially in rural and underserved areas, during the 1960s. Many communities lacked adequate access to basic healthcare. Dr. Loretta Ford recognized that experienced nurses already possessed clinical skills that, with additional training, could be expanded to include health assessments, diagnosis, and treatment planning for common conditions.
- When did nurse practitioners gain prescriptive authority?
- Nurse practitioners began gaining prescriptive authority in the 1970s, with North Carolina becoming one of the first states to grant it. By the mid 1990s, most states had enacted some form of prescriptive authority for NPs. Today, all 50 states and the District of Columbia allow NPs to prescribe medications, though the degree of physician oversight required still varies by state.
- What was the first nurse practitioner program?
- The first nurse practitioner program was the Pediatric Nurse Practitioner Program at the University of Colorado, launched in 1965. Co-founded by Dr. Loretta Ford, a nurse, and Dr. Henry Silver, a physician, the program trained registered nurses to perform physical exams, manage common childhood illnesses, and provide well-child care in settings where physicians were scarce.
- How long have nurse practitioners been around?
- Nurse practitioners have been around for over 60 years, dating back to 1965. In that time the profession has grown from a single pilot cohort in Colorado to more than 400,000 licensed NPs practicing across the United States as of 2026. The role has expanded well beyond pediatrics into family practice, acute care, psychiatry, and dozens of other specialties.