Most important takeaways…
- University of Miami launches a formal NP aesthetic certification in fall 2026.
- State practice authority tiers determine your supervisory and prescriptive requirements.
- Neurotoxin and dermal filler training require separate clinical skill progressions.
Weekend workshop versus university-based certificate program: that contrast defines exactly where aesthetic medicine training for nurse practitioners stands in 2026. For years, the field has operated without formalized standards, with many practitioners learning botulinum toxin and filler techniques through one- or two-day courses that vary wildly in quality and clinical depth.
That is starting to change. The University of Miami School of Nursing and Health Studies is launching an aesthetic medicine certification course in fall 2026, developed in partnership with nonsurgical specialist Daniel L. Campos. Hudson Santos, the school's dean, put the problem plainly: "Aesthetics medicine is no longer a niche, but it has no formalized training for those practitioners." The UM program, which targets NPs and APRNs holding board certification and an MSN or DNP, is one of the clearest signals yet that academia is stepping in to fill that gap. For NPs weighing whether to pursue a terminal degree before entering aesthetics, understanding how long a DNP program takes can help you plan your timeline.
The practical tension for NPs is real. Advanced practice nursing trends in 2026 point toward greater credentialing scrutiny across every specialty, and aesthetics is no exception. State scope-of-practice laws, patient safety liability, and career earning potential all hinge on the quality of your training and the credentials behind it.
What Training Do Nurse Practitioners Need for Cosmetic Injectables?
Cosmetic injectables training for NPs sits on a continuum: on one end, quick weekend workshops; on the other, multi-month hybrid certificates anchored in university rigor. Choosing the right path depends on your career goals, your state's scope-of-practice rules, and how deeply you want to understand the anatomy, pharmacology, and safety skills behind neurotoxins and dermal fillers.
Prerequisites: What You'll Need Before Training
Every program expects an active, unrestricted clinical license, but accredited NP-specific courses set the bar higher. For example, the University of Miami School of Nursing and Health Studies is launching a new aesthetic medicine certification in fall 2026 that targets advanced practice registered nurses with an active Florida APRN license. Their prerequisites are a strong model for serious programs: - Board certification as an NP - A MSN or DNP degree from a regionally accredited institution - Current Basic Life Support (BLS) and Advanced Cardiac Life Support (ACLS) certification
Most reputable training providers mirror these gatekeeping standards, often requiring proof of licensure and malpractice insurance before you step into a hands-on lab. Some beginner tracks welcome RNs or other licensed professionals1, but if you want to inject independently as an NP, pick a course that teaches to autonomous practice.
Weekend Workshops vs. Accredited Certificates
The aesthetic industry has long relied on short, intensive courses. A one-day AAOPM NP Botox Training packs 8 CME credits into a single session for around $1,899.2 PracticalCME's Botox and Filler Training offers 7.25 hours total, including 4.75 clinical hours.3 These workshops get you started, but they are often the "weekend courses" that critics worry about. As Daniel Campos, a nonsurgical aesthetic medicine specialist and UM program partner, bluntly put it: "In Florida, if you can prescribe an antibiotic, you can inject the face." His point underscores why formalized, multi-step education is becoming essential.
Accredited programs fill the gap. Columbia University School of Nursing's Clinical Aesthetics Injectables Certificate uses online didactic work plus in-person simulation, with the didactic portion approved for CE credits.4 The National Laser Institute's five-day Core Injection Medical Aesthetics Course provides concentrated hands-on practice.5 These programs emphasize safety, complication management, and a deep understanding of facial anatomy, areas where a two-day workshop can only scratch the surface.
The Core Curriculum: What You'll Learn
A solid training pathway follows a logical progression: - Didactic foundation: You'll study the pharmacology of botulinum toxin type A and hyaluronic acid fillers, facial musculature, vascular danger zones, and patient assessment. Courses like the AACM Comprehensive Course require you to perform a minimum of 10 neuromodulator and 8 filler injections under supervision.3 - Hands-on injecting: After mastering theory, you move to live models. The Derma Institute USA's live activity provides 16 CME credits through extended practice.6 National Trade Institute's 16-hour Cosmetic Injectables Program devotes half its time to lab work.7 - Mentored clinical hours: The final layer is supervised practice, where an experienced injector reviews your technique, guides complication drills, and signs off on your readiness. The number of required cases varies: PracticalCME mandates 4.75 clinical hours; AACM's beginner course sets a minimum of 4 neuromodulator and 4 filler injections.3
How Long Certification Takes
Timelines range dramatically. A weekend intensive gives you fundamentals in 1 to 2 days. A hybrid program like Columbia's certificate might stretch over several weeks, blending self-paced online modules with one or two in-person simulation days. The UM program, launching in fall 2026, signals a shift toward semester-length, graduate-level training that builds lasting competence. For NPs considering whether their current degree positions them well for this path, understanding full practice authority states for NPs can clarify how much independent practice authority your credential actually carries. The right program length for you depends on your baseline knowledge and how independently you plan to practice. For NPs aiming to lead an aesthetic practice, investing in a longer, accredited program is increasingly the standard.
Accredited Cosmetic Injectables Programs for NPs: What to Look For
Cosmetic injectable training for nurse practitioners is shifting from informal weekend workshops toward programs with real academic and accreditation credentials. That shift matters, because the course you choose will shape your clinical competence, your liability exposure, and how your continuing education credits are recognized by certifying bodies.
Program Formats: Hybrid, In-Person, and Online-Plus-Preceptorship
Three delivery models dominate the market right now, and each involves trade-offs.
In-person intensive programs pack didactic content and hands-on injection practice into one or two concentrated days. Empire Medical Training1 and the American Academy of Aesthetic Medicine Professionals (AAOPM)2 both follow this model, with costs ranging from roughly $1,299 to $1,699 and approximately 8 CE credits awarded through ACCME-accredited providers. These programs work well for nurses who want to move quickly and already have a practice setting lined up for supervised follow-through.
Hybrid programs blend online coursework with required in-person clinical sessions. The American Academy of Aesthetic Medicine and Surgery (AAAMS) offers a hybrid course at around $2,500 that awards 17 CE credits,5 giving participants more instructional depth before they ever pick up a syringe. The University of Miami School of Nursing and Health Studies is also entering this space with a new academic hybrid certification launching in fall 2026, co-developed with a nonsurgical aesthetic medicine specialist and targeting APRNs with active Florida licenses.
Online-didactic-plus-preceptorship models separate the theory portion entirely from the clinical component. They offer scheduling flexibility for working nurses but demand that you independently secure a qualified preceptor, which can be a real obstacle in areas with limited aesthetic practices.
Accreditation Markers That Actually Matter
Not all CE credits are equal in the eyes of your certifying body. If you hold AANP or ANCC certification, you need CE credits from providers those organizations recognize. ACCME accreditation (the standard for physician CME) is widely accepted, but confirm acceptance with your specific certifying body before enrolling. Some organization-specific credentials carry little weight for NP license renewal.
Beyond credit recognition, look for nursing program accreditation when a university is involved. An academic program housed within a regionally accredited school of nursing signals a level of curricular oversight that standalone commercial courses cannot always match.
Key Comparison Checklist
When evaluating any program, run through these dimensions before committing:
- Accreditation body: Does the granting organization align with AANP or ANCC CE requirements?
- Hands-on injection hours: How many live patient or model encounters are included, and under what supervision ratio?
- CE credit count: Fewer credits is not necessarily worse, but the count should reflect genuine instructional time.
- Cost: Programs currently range from roughly $1,300 for a focused in-person day to $2,500 or more for hybrid formats with broader curricula.
- Post-course mentorship: Some programs offer follow-up access to instructors or peer networks. For NPs building a new skill set in a high-stakes area, that ongoing support can be as valuable as the course itself.
The right program is the one that matches your current licensure requirements, your learning style, and the clinical environment where you intend to practice.
Questions to Ask Yourself
State-By-State NP Scope of Practice for Aesthetic Injectables
Understanding where you can legally perform cosmetic injectables, and under what conditions, is one of the most important steps before you invest in training or launch an aesthetic practice. State laws vary dramatically, and the rules that govern your prescriptive authority do not always align with the rules that govern the actual injection procedure. Here is a practical breakdown of how the regulatory landscape works across the country.
The Three-Tier Framework
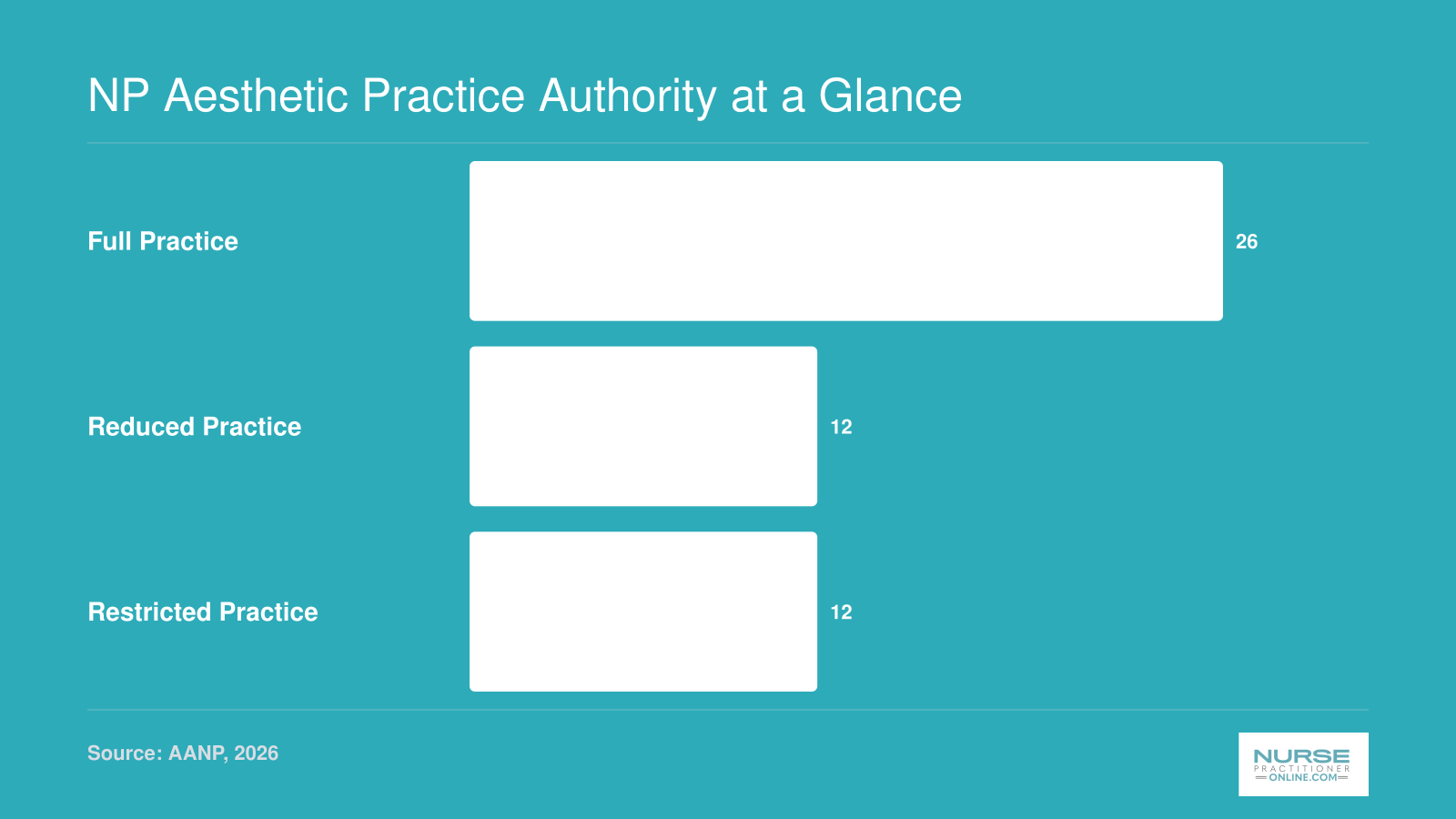
The American Association of Nurse Practitioners categorizes state practice environments into three tiers, and each tier has direct implications for aesthetic injectable work. Nurse practitioner practice authority by state provides a detailed breakdown of where every state currently stands.
- Full practice authority (30 states plus D.C.):1 NPs in these states can evaluate, diagnose, prescribe, and perform procedures independently. If your state grants full practice authority, you can generally perform cosmetic injectables without a collaborative agreement or physician oversight, assuming you have appropriate training and credentialing.
- Reduced practice authority:2 These states require a collaborative agreement with a physician before you can practice. In aesthetic settings, that agreement typically must specify the procedures you are authorized to perform, outline a protocol for managing complications, and establish how the collaborating physician will review your work.
- Restricted practice authority:2 NPs in restricted states must work under direct or indirect physician supervision. In the aesthetic context, this often means a physician must delegate authority for each procedure category and may need to be physically available or on-site during treatment.
The tier your state falls into sets the baseline, but individual state boards can layer on additional requirements for aesthetic procedures specifically.
State Spotlights: Where the Rules Differ Most
A few high-population states illustrate how much variation exists.
New York operates under full practice authority as of 2026, meaning NPs with proper training can offer Botox, dermal fillers, and other injectables independently.1 This makes New York one of the more straightforward states for NPs who want to build an aesthetic practice without a formal supervisory arrangement.
Florida presents a more complex picture. Despite its reputation as a hub for cosmetic procedures, Florida classifies aesthetic medicine as a practice of medicine, which means NPs cannot perform injectables independently.3 Physician delegation is required, and a good faith examination must be completed before any aesthetic procedure.4 As aesthetic medicine specialist Daniel Campos noted in connection with the University of Miami's new certification program, "In Florida, if you can prescribe an antibiotic, you can inject the face," highlighting the gap between prescriptive authority and procedural oversight that the state's regulatory framework creates. Registered nurses in Florida face even tighter restrictions, requiring direct physician supervision for any injection.5
California also falls into the restricted category. NPs performing cosmetic injectables must work under physician supervision, and the supervising physician is expected to establish standardized procedures for the services being offered.2
Texas similarly requires physician supervision for NPs performing aesthetic procedures.2 The state's prescriptive authority rules are detailed and may impose additional documentation requirements for controlled substances or prescription medications used in aesthetic settings.
Illinois operates under reduced practice authority, so NPs need a collaborative agreement to practice.1 If you are considering aesthetic work in Illinois, your collaborative agreement should explicitly cover the injectable modalities you plan to offer, the protocols for patient screening, and the process for referring complications.
Prescriptive Authority Is Not the Same as Procedural Authority
This is a distinction that catches many NPs off guard. Even if your state permits you to prescribe Botox (which is a prescription drug), that prescriptive authority does not automatically mean you are cleared to perform the injection itself. Some states treat the act of injecting a cosmetic product as a medical procedure that requires separate authorization, delegation, or supervision. To understand how this intersects with broader scope of practice for nurse practitioners, review your state's procedural rules carefully before assuming your prescribing privileges cover you.
Who Regulates What
In most states, your board of nursing is the primary regulatory body governing NP scope of practice. However, aesthetic procedures sometimes also fall under the jurisdiction of the state medical board, particularly in states that classify cosmetic injectables as a medical act rather than a nursing act. A few states also have specific med spa or aesthetic facility licensing requirements administered by separate agencies.
The practical advice here is straightforward: check both your state board of nursing and your state medical board before you start treating patients. When a collaborative agreement is required, ask whether your collaborating physician needs to have aesthetic experience. Some states are silent on this point, while others specify that the collaborator should be practicing in a related specialty.
What a Collaborative Agreement Should Cover
If you practice in a reduced or restricted state, your collaborative agreement is the legal backbone of your aesthetic practice. At a minimum, it should address the specific procedures you are authorized to perform, protocols for managing adverse events such as vascular occlusion or allergic reactions, the frequency and method of chart reviews, and how the collaborating physician can be reached during patient treatment hours. Some states also require that the collaborating physician be within a certain geographic radius or available within a defined response time. Failing to meet these requirements can put your license at risk, so treat the agreement as a living document that you review and update regularly.
NP Aesthetic Practice Authority at a Glance
Not every state treats NP aesthetic injectable authority the same way. Practice authority falls into three tiers that directly affect how independently you can offer cosmetic injectables. Understanding where your state lands helps you plan training, collaborating physician requirements, and business structure before you invest in a certification program.
Patient Safety: Preventing and Managing Injectable Complications
Preventing and managing injectable complications isn't an optional skill , it's a professional obligation for every nurse practitioner entering aesthetic medicine. Safety begins long before the first injection and continues through every follow-up. Formalized training, like the new University of Miami certification, directly addresses the gaps that have left many NPs relying on weekend courses and anecdotal protocols.
Common Complications and Their Root Causes
Most injectable complications are minor, but the rare serious events demand immediate, competent response. NPs must be able to distinguish between expected side effects and genuine emergencies.
- Bruising and swelling: Nearly universal after needle trauma or vessel injury. Proper pre-injection icing, use of blunt-tip cannulas, and avoidance of anticoagulants can minimize severity.
- Infection: Uncommon with sterile technique but rises when aseptic protocols lapse, with reactivation of dormant infections like herpes simplex, or in immunocompromised patients.
- Allergic reactions: Ranging from local urticaria to rare anaphylaxis. History-taking for lidocaine or filler-component allergies is critical.
- Vascular occlusion: The most feared complication, occurring in roughly 1 in every 6,000 filler syringes,1 with some estimates between 1 in 2,000 and 1 in 10,000 injections.2 Even with low incidence, the rise in procedures has driven a 1,700% increase in serious filler-related injuries between 2005 and 2020,3 a 30-fold jump in ischemic skin injuries, and a 300% increase in stroke reports.4
Vascular Occlusion: The Emergency Every NP Must Master
Vascular occlusion happens when filler is accidentally injected into an artery, starving downstream tissue of oxygen. High-risk zones include the glabella, nasolabial fold, nasal tip, and alar triangle.5 Without prompt reversal, it can lead to skin necrosis, blindness, or cerebral infarction.6
Every aesthetic NP must internalize the ASDS Task Force protocol for vascular occlusion:
1. Stop injecting immediately at any sign of blanching, severe pain disproportionate to the injection, or mottled skin. 2. Activate your emergency kit and inject hyaluronidase into the occluded territory at 10, 20 units per injection point.7 3. Support circulation with warm compresses and administer aspirin (if not contraindicated) to reduce platelet aggregation. 4. Refer emergently if vision changes, ocular pain, or neurological symptoms appear, as ophthalmic artery occlusion requires multidisciplinary hospital care.
Infection Control as a Daily Discipline
Even outpatient aesthetic practice demands rigorous aseptic technique. Dermatology nurse practitioners working in aesthetics apply the same infection control standards used across procedural specialties. Before any injection:
- Conduct a thorough contraindication screen: active cold sores, immunocompromised status, pregnancy, breastfeeding, and recent dental or surgical procedures near the treatment area.
- Cleanse skin with an alcohol- or chlorhexidine-based agent and allow it to dry completely.
- Use single-use, sterile needles or cannulas and never recap.
Post-procedure, give patients clear written instructions: no touching or applying makeup for several hours, and report any spreading redness, warmth, or fever immediately. For lip filler patients, advise against straws or vigorous mouth movement for 24, 48 hours.
Protecting Your License and Livelihood with Malpractice Insurance
Standard NP liability policies often exclude cosmetic procedures or limit coverage. Aesthetic NPs need a specialty occurrence-based policy with minimum limits of $1 million per claim and $3 million aggregate, which is typical for this field. Claims in aesthetics are not just about negligence; they increasingly allege lack of informed consent around vascular occlusion risk or off-label product use. An experienced broker can help you assess whether your policy covers hyaluronidase administration and emergency transport to a higher level of care. Understanding how to negotiate an NP contract , including coverage terms , matters here; NP contract negotiation guidance can help you ask the right questions before signing on with any aesthetic practice. As dermal filler complications rise, a robust safety net is no longer optional , it's part of competent practice.
Related Articles
Botox Vs. Dermal Fillers: How NP Training Differs by Modality
Neurotoxin injections and dermal filler placements may both fall under the umbrella of cosmetic injectables, but from a pharmacological, anatomical, and risk standpoint, they are fundamentally different procedures that demand distinct training tracks.
How the Products Work Differently
Neurotoxins like Botox, Dysport, and Xeomin act by temporarily blocking acetylcholine release at the neuromuscular junction. In practical terms, they reduce muscle contraction in targeted facial areas, softening dynamic wrinkles such as crow's feet and forehead lines. Injections are relatively superficial, directed into specific muscles, and the anatomical margin for error is comparatively forgiving.
Dermal fillers operate on an entirely different mechanism. Products based on hyaluronic acid, calcium hydroxylapatite, or poly-L-lactic acid restore lost volume, sculpt contours, or smooth static lines by physically occupying space within the tissue. Injection depths vary widely depending on the product and the treatment zone, and each filler type has its own rheological properties (viscosity, elasticity, cohesivity) that influence how and where it should be placed. Vascular anatomy becomes a critical concern because inadvertent intravascular injection of filler can lead to tissue necrosis or, in rare cases, blindness.
Why Training Follows a Clear Progression
Well-structured programs typically introduce neurotoxins first. The lower complication profile and more forgiving anatomy allow new aesthetic NPs to develop core injection skills, build confidence with patient assessment, and learn facial musculature mapping before facing higher-stakes procedures. Once a practitioner demonstrates competence with neurotoxins, training advances to dermal fillers, starting with lower-risk zones like the lips and marionette lines before progressing to high-risk areas such as the periorbital region, nasolabial fold, and temple. Some advanced programs then add procedures like PDO thread lifts or liquid rhinoplasty, which carry elevated vascular and structural risks.
This progression is not arbitrary. It mirrors the escalating complexity of each modality and prepares NPs to recognize and manage complications appropriate to each level. For nurse practitioner advancement opportunities in aesthetics, understanding this hierarchy early helps you map a deliberate, competency-driven career path.
Credentialing Can Differ by Modality
Some states and credentialing bodies draw a line between neurotoxin and filler competency. An NP who has completed training for Botox injections may not automatically be credentialed to perform dermal filler procedures without additional coursework, supervised clinical hours, or documentation of competency. Before advertising filler services, verify whether your state board of nursing or collaborative physician agreement (if applicable) requires separate authorization.
Building Your Progression Plan
Rather than trying to learn everything at once, approach your training as a stepwise build:
- Start with neurotoxins: Complete a reputable training course, perform supervised injections, and gain comfort with patient selection and dosing before branching out.
- Add fillers deliberately: Choose a program that includes cadaver lab or live-model training focused on vascular anatomy and emergency protocols, particularly hyaluronidase use for hyaluronic acid complications.
- Progress to high-risk zones with mentorship: Areas like the glabella, temples, and nose carry the highest complication potential. Seek one-on-one mentorship or advanced workshops specifically addressing these zones before treating patients independently.
- Document everything: Keep a log of procedures performed, complications encountered, and continuing education hours. This record supports credentialing applications and demonstrates due diligence if questions arise.
Mastering one modality before layering in the next is not just a best practice in training; it is a patient safety imperative. The NPs who build the strongest reputations in aesthetic medicine are the ones who resist the temptation to offer every service immediately and instead demonstrate new nurse practitioner confidence through measured, documented growth in their clinical competence.
NP Salary Potential in Aesthetic Medicine
The tradeoff most NPs weigh here is straightforward: aesthetics can pay well, but the earnings picture is less predictable than a hospital or primary care role with a published pay scale. Compensation in aesthetic medicine varies widely based on employment structure, location, patient volume, and whether you earn a flat salary, commission on procedures, or a mix of both.
Where to Find Reliable Salary Data
Because aesthetic-specific NP compensation surveys are rare, you'll need to triangulate from several sources rather than rely on a single number.
- BLS Occupational Outlook Handbook: The Bureau of Labor Statistics (bls.gov) publishes median wages and job growth projections for nurse practitioners as a whole. This gives you a baseline, though it does not break out aesthetics as a subspecialty.
- AANP and Medscape reports: The American Association of Nurse Practitioners and Medscape's annual NP compensation surveys offer ranges by setting, region, and years of experience. Aesthetic figures are usually folded into broader categories, but the general NP data still applies as a floor.
- Aesthetic-focused communities: Groups tied to the American Academy of Aesthetic Medicine, along with peer forums and NP-specific aesthetic networks, often surface real-world employer offers, commission structures, and 1099 arrangements that formal surveys miss.
- Program alumni outcomes: Universities offering aesthetic certification tracks sometimes track post-graduation placement. Ask program coordinators directly about typical starting arrangements for their graduates.
What Actually Drives Your Income
Two NPs with the same certification can earn very different amounts. Nurse practitioner salary by state is one of the clearest external signals, since geographic demand shapes both base pay and procedure volume in aesthetic practices. The variables that matter most are the compensation model (W-2 salary, hourly, or percentage of revenue), whether you're building your own patient book or joining an established practice, and how many procedures you can safely and comfortably perform per day. It's also worth understanding why nurse practitioners leave primary care for specialties like aesthetics, since that shift often comes with a real change in how income is structured. NPs who own or co-own med spas take on more risk but generally have the highest ceiling. Those who work part-time in aesthetics alongside a clinical role often use it as supplemental income while they build volume and referrals.
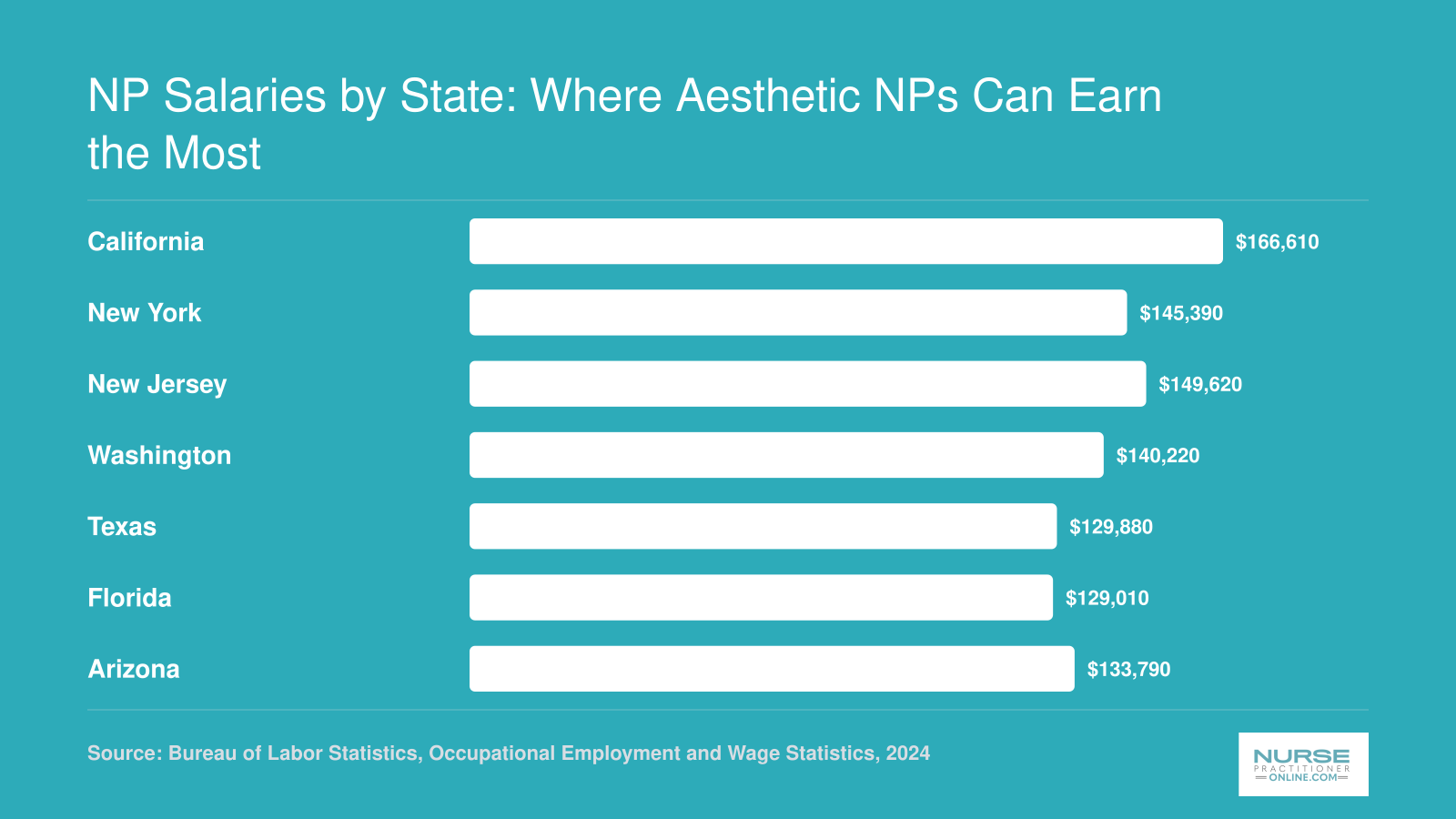
NP Salaries by State: Where Aesthetic NPs Can Earn the Most
Geographic location plays a major role in nurse practitioner earning potential, and several of the highest-paying states also happen to be hotspots for aesthetic medicine demand. Below are median annual salaries for nurse practitioners in seven states that combine strong compensation with robust cosmetic injectables markets. Aesthetic NPs in private practice or med spas may earn above these medians, but these figures offer a reliable baseline.
How to Choose the Right Cosmetic Injectable Course as an NP
Choosing the right injectables course is one of the most consequential decisions you'll make as an NP entering aesthetics. The market is crowded, quality varies wildly, and the wrong program can leave you undertrained and legally exposed. Use the framework below to separate rigorous training from marketing gloss.
Five Criteria to Evaluate Every Program
- Accreditation and CE recognition: Confirm the course is recognized by your state board of nursing for continuing education and, ideally, is affiliated with a university, medical school, or nationally recognized aesthetic organization. If a program cannot name its accrediting body, walk away. How to evaluate FNP programs offers a useful parallel framework for vetting any advanced nursing credential.
- Hands-on hours and live-patient count: Ask how many live patients you will personally inject, not just observe. Reputable programs disclose exact numbers. A two-day didactic course with one or two injections is not enough to practice safely. NP simulation training in nurse practitioner education can help you understand what rigorous hands-on clinical preparation actually looks like before you enroll.
- Post-course mentorship: Look for structured follow-up, whether that's case review, virtual consultation on treatment plans, or a mentor you can text photos to during your first months. This ongoing support is often what separates confident new injectors from cautious ones.
- Cost relative to earning potential: Tuition ranges from roughly $2,000 for weekend courses to $15,000 or more for university certificates. Weigh the price against the depth of training, not the length. A cheap course you cannot legally use is not a bargain.
- Recertification and renewal: Ask what's required to stay current. Aesthetics evolves quickly, and programs that build in annual updates or refresher modules signal a serious commitment to competence.
Red Flags to Avoid
- No live-patient injection component
- No named or verifiable accrediting body
- Instructors whose aesthetic credentials cannot be confirmed independently
- Any promise to certify you in neurotoxins, fillers, PDO threads, and biostimulators over a single weekend
Plan for Supervision Before You Enroll
If you practice in a collaborative-agreement or reduced-practice state, you will need a physician collaborator in place before you inject your first patient. Ask prospective programs whether they help graduates connect with collaborating physicians or medical directors, particularly if you plan to open your own practice. Some university-affiliated programs maintain referral networks; most weekend courses do not. Sorting out supervision after you've paid tuition is a costly way to learn this lesson. NP residency programs are another avenue some NPs use to build supervised procedural experience in structured clinical settings.
Common Questions About NP Cosmetic Injectables Training and Practice
Aesthetic medicine is one of the fastest growing areas of NP practice, but it raises real questions about legality, training standards, and risk. Below are the questions nurse practitioners ask most often before entering the cosmetic injectables space.
- Can nurse practitioners legally perform cosmetic injectables in every state?
- Not uniformly. NP authority to perform cosmetic injectables varies significantly by state. In full practice authority states, NPs can typically prescribe and administer injectables independently. In restricted or reduced practice states, a collaborative agreement or physician supervision may be required. Some states have additional board of nursing rules specific to aesthetic procedures. Always verify your own state board's current regulations before offering injectable services.
- What training is required for nurse practitioners to administer Botox and fillers?
- At minimum, NPs need their active APRN license, board certification, and completion of a cosmetic injectables training program that covers facial anatomy, injection techniques, product pharmacology, and complication management. Programs like the University of Miami's new aesthetic medicine certification, launching fall 2026, combine online didactics with hands-on clinical training. Most credible programs also require current BLS and ACLS certification as prerequisites.
- How long does cosmetic injectables certification take for NPs?
- Program length varies widely. Weekend or short-format courses can run two to four days, but these often lack the depth needed for safe, competent practice. More comprehensive programs, such as hybrid academic certifications offered through university partnerships, may span several weeks to a full semester. Programs with substantial nurse practitioner clinical rotations and mentored injections generally produce better prepared practitioners.
- Do nurse practitioners need physician supervision for aesthetic procedures?
- It depends on your state. In the 27 states and territories that grant full practice authority, NPs can practice independently, including in aesthetics. In states with reduced or restricted authority, a collaborative agreement or supervisory arrangement with a physician is typically required. As Daniel Campos noted about Florida's regulatory landscape: "If you can prescribe an antibiotic, you can inject the face." Check your state's specific requirements carefully.
- What are the most serious risks of cosmetic injectables that NPs should know?
- The most critical risks include vascular occlusion (which can lead to tissue necrosis or even blindness if filler is inadvertently injected into or near an artery), severe allergic reactions, infection, nerve damage, and asymmetry. NPs must be trained in emergency protocols, including hyaluronidase use for filler reversal. Understanding detailed facial vascular anatomy is essential, and this is a key reason formalized training matters far more than weekend courses.
- How much do aesthetic nurse practitioners earn compared to other NP specialties?
- Aesthetic NPs often earn at the higher end of the NP salary range, with experienced practitioners in metropolitan areas frequently earning above the national NP median. For context, the highest paid nurse practitioner specialties consistently reward procedural and specialty skills. Compensation can include base salary plus production bonuses or commission on injectable services. Earnings vary by state, practice setting, patient volume, and whether the NP owns their practice versus working for a medical spa or physician group.
- Do NPs need separate malpractice insurance for aesthetic procedures?
- Yes, in most cases. Standard NP malpractice policies may not cover cosmetic or elective aesthetic procedures. NPs entering this specialty should confirm that their policy explicitly includes aesthetic injectables, or purchase a separate rider or specialty policy. Coverage should address both claims related to injection complications and any business liability if operating an independent practice. Reviewing your contract terms carefully before starting is equally important , nurse practitioner contract negotiation resources can help you understand what to look for. Speak with your insurer before performing your first procedure.