Most important takeaways…
- Most NP programs now require 500 to 1,000 direct patient care hours depending on your chosen specialty.
- Securing a preceptor early is critical because 60% of practicing NPs are not currently precepting students.
- Strong clinical presentations and patient communication directly influence the autonomy your preceptor grants you.
- Clinical rotations function as working auditions that shape your specialty options, references, and first job offers.
NP clinical rotations are the 500 to 1,000 or more hours of supervised patient care that transform classroom knowledge into real diagnostic and treatment skills. For most nurse practitioner students, this phase feels both exhilarating and overwhelming: you are finally practicing medicine, but every assessment, every differential, every patient interaction is being evaluated.
The challenge is not just logging hours. Finding a qualified preceptor, adapting to different clinical sites, and building the confidence to present patients clearly all require deliberate preparation. Working nurses face the added pressure of coordinating rotation schedules around existing shifts and family commitments.
Programs vary widely in how much support they offer, and students who enter clinicals with a clear plan consistently report better outcomes and stronger preceptor relationships. Below, we break down four practical tips to help you navigate every stage of your nurse practitioner rotations with confidence.
What Are NP Clinical Rotations and Why Do They Matter?
Nursing textbooks and simulation labs give you the knowledge, but real clinical confidence only comes from hands-on practice with actual patients. That is exactly what nurse practitioner clinical rotations deliver. Unlike optional observerships or shadowing, these rotations are mandatory, accreditation-driven experiences woven into every NP program. They are the bridge between classroom theory and independent practice.
From Classroom to Clinic: The Core Purpose of NP Rotations
NP clinical rotations are supervised, patient-facing training blocks that immerse you in real-world healthcare settings. Accrediting bodies like the Commission on Collegiate Nursing Education (CCNE) and the Accreditation Commission for Education in Nursing (ACEN) require them because they ensure you develop the diagnostic reasoning, procedural skills, and professional judgment essential for safe, effective care. Without completing the required clinical hours, you simply cannot graduate from an accredited program.
What You'll Actually Do During Clinical Rotations
During rotations, you step into the role of the nurse practitioner student in clinical rotations under the guidance of a licensed preceptor, an experienced NP or physician. Your days will include: - Patient assessments: Conducting comprehensive histories and physical exams. - Diagnostic formulation: Developing nurse practitioner differential diagnosis skills and ordering labs or imaging. - Prescribing under supervision: Writing prescriptions with preceptor approval, learning to manage medication regimens safely. - Documentation and charting: Navigating electronic health records (EHRs) efficiently. - Case presentations: Presenting patient findings to your preceptor and discussing evidence-based plans.
This active involvement builds your clinical reasoning muscles far faster than passive observation ever could.
The Certification and Licensure Connection
You cannot sit for national board certification exams, such as those offered by the American Nurses Credentialing Center (ANCC) or the American Association of Nurse Practitioners (AANP), until you have completed your program's clinical hour requirements. State licensure boards similarly mandate verification of these hours, and nurse practitioner practice authority by state varies once you are certified. In short, clinical rotations are not just a box to check; they are the prerequisite to earning the NP credentials that allow you to practice.
Payment and Financial Considerations
A common question is whether NP students get paid during clinicals. The straightforward answer: rotations are unpaid educational experiences, not employment. You are there to learn, not to provide billable services independently. However, some healthcare employers do offer tuition reimbursement or stipends for employed nurses advancing their education, so it is worth exploring benefits through your current workplace. Keep in mind that arranging your own preceptor may also involve logistical costs, a topic we cover in a later section.
Clinical Hour Requirements by NP Specialty
Every nurse practitioner program in the United States must meet a minimum of 500 direct patient care hours as mandated by the National Task Force on Quality Nurse Practitioner Education, but the current standard across all major accrediting bodies has risen to 750 clinical hours for master's-prepared programs and 1,000 total practice hours for DNP programs as of 2025-2026.1
Standard Clinical Hour Minimums Across All NP Specialties
The Commission on Collegiate Nursing Education (CCNE) and the Accreditation Commission for Education in Nursing (ACEN) both enforce the same baseline: 750 clinical hours for MSN programs and 1,000 hours for Doctor of Nursing Practice programs.1 This standard applies uniformly to Family Nurse Practitioner (FNP), Adult-Gerontology Acute Care Nurse Practitioner (AGACNP), Adult-Gerontology Primary Care Nurse Practitioner (AGPCNP), Psychiatric-Mental Health Nurse Practitioner (PMHNP), Pediatric Nurse Practitioner Acute Care (PNP-AC), Pediatric Nurse Practitioner Primary Care (PNP-PC), Women's Health Nurse Practitioner (WHNP), and Neonatal Nurse Practitioner (NNP) tracks.
Many programs voluntarily exceed these minimums. It's common to see FNP programs requiring 600 to 700 clinical hours even at the master's level, and some institutions build in an extra 100 to 200 hours to give students greater exposure to complex cases and specialty settings. The 2021 AACN Essentials framework does not prescribe higher hour counts but emphasizes competency-based progression, which often translates to more time in the field.2
Direct Patient Care vs. Total Clinical Hours
Accrediting bodies distinguish between direct patient care hours and total clinical or practice hours. Direct patient care means face-to-face time with patients under preceptor supervision, conducting assessments, formulating diagnoses, creating treatment plans, and performing procedures. The 750-hour minimum for master's programs refers specifically to this direct care component.3
Simulation lab hours, case studies, and skills workshops may count toward total practice hours in DNP programs but cannot substitute for direct patient care hours in any of the eight major NP specialties as of 2026.3 Both CCNE and ACEN explicitly prohibit replacing direct care time with simulation when calculating the 750-hour threshold, though simulation remains a valuable supplement for procedural skills and rare-event training.
Typical Number of Clinical Rotation Sites by Specialty
The breadth of settings varies by track. FNP students typically rotate through three to five sites: primary care clinics, pediatric offices, women's health centers, and often an urgent care or hospital setting. AGACNP students, who focus on high-acuity environments as described in our acute care nurse practitioner career guide, concentrate on two to three acute care settings such as intensive care units, emergency departments, and specialty inpatient services. PMHNP rotations usually span two to four sites, including outpatient mental health clinics, inpatient psychiatric units, substance use treatment centers, and sometimes correctional or community mental health settings.
PNP-AC and NNP students often complete rotations in neonatal intensive care units, pediatric ICUs, and pediatric emergency departments, usually across two to three hospital systems. If you are considering this path, exploring online PNP programs can help you compare rotation structures. WHNP students rotate through OB-GYN clinics, family planning centers, and labor and delivery units, typically at two to three locations. AGPCNP students mirror FNP settings but focus exclusively on adult and older adult populations, usually requiring three to four rotation sites.
Understanding these hour and setting requirements early helps you plan your schedule, coordinate preceptor placements, and ensure you graduate ready for certification and practice.
What a Typical Week in NP Clinicals Looks Like
Clinical rotations follow a rhythm that most students describe as intense but sustainable, especially once you find the right balance between patient care, documentation, and life outside the clinic. Most NP students dedicate two to three full days per week to clinical practice, with shifts ranging from eight to twelve hours depending on the specialty and site. The remaining days are reserved for coursework, exam preparation, clinical logs, and the reading that follows you home after every patient encounter.
A Day in the Life of Clinical Practice
Your clinical day typically starts thirty to sixty minutes before the first scheduled patient. You arrive early to review charts, flag complex cases, and align with your preceptor on the day's learning priorities. Once clinic begins, you will see eight to fifteen patients depending on the setting and your stage of training. Family practice and urgent care rotations tend toward higher volume, while specialty clinics such as cardiology or women's health may involve fewer but more complex presentations.
Between patient visits, you document findings, draft assessment and plan notes, and present cases to your preceptor. Early in your program, these presentations may feel scripted and slow. By your final semesters, you will move through them with the fluency of a seasoned clinician. The day wraps with a debrief, sign-off on documentation, and often a handful of follow-up questions your preceptor encourages you to research before the next shift.
How Autonomy Grows Across Semesters
First-semester clinicals are heavily shadowed. You observe more than you perform, absorbing workflow, communication styles, and clinical reasoning in real time. By mid-program, you are expected to take the lead on initial assessments, formulate differential diagnoses, and propose management plans before your preceptor weighs in. Final rotations mirror independent practice: you manage patients from intake through disposition, with your preceptor available for consultation and final sign-off but no longer hovering.
Patient volume scales accordingly. Where you might have seen five patients in a four-hour block during your first rotation, you will handle twelve to fifteen in the same window by graduation, and your documentation will be faster, more precise, and less reliant on templates. Rotations in areas like adult gerontology nurse practitioner care can be especially demanding, given the complexity of geriatric presentations.
Study and Administrative Work Outside Clinical Days
Clinical learning does not end when you leave the site. Expect to spend several hours each week reading up on diagnoses you encountered, reviewing lab results and imaging studies, and preparing for clinical conferences or case presentations. You will also maintain clinical logs, update competency checklists, and complete midterm and final evaluations with your preceptor. If you are still exploring how to begin this journey, our guide on how to enroll in NP school online walks you through the process step by step. The administrative layer of clinicals is non-negotiable and often more time-consuming than students anticipate during their first rotation.
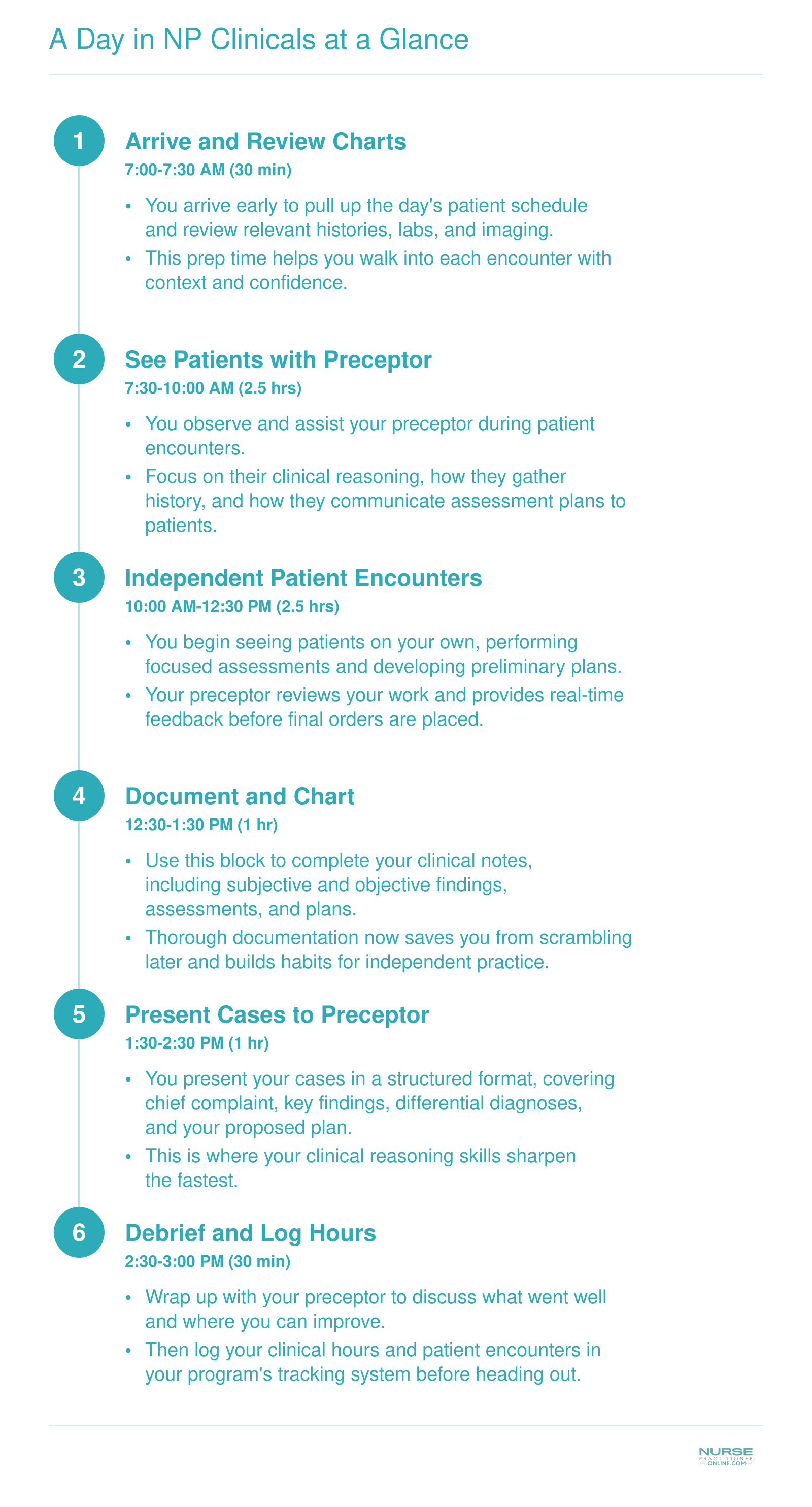
A Day in NP Clinicals at a Glance
Wondering what a full day in nurse practitioner clinicals actually looks like? Here is a realistic breakdown of the pacing and flow you can expect during a typical clinical rotation shift. Times will vary by site and specialty, but this sequence gives you a solid sense of how the day unfolds.
How to Find and Secure a Clinical Preceptor
Securing a preceptor is one of the most critical steps in your NP education, yet it often becomes a source of stress. A 2022 survey of 334 NPs revealed that 60% are not precepting, with common barriers including never being asked (38%) and employer restrictions (33%).1 With an estimated 28,000 NP students needing clinical placements annually and more than 80,000 qualified nursing applications turned away in 2024 due to faculty shortages, the competition for preceptors is real.23 Understanding the landscape and starting early can make all the difference.
School-Placed vs. Self-Placed Rotations
NP programs generally follow one of two models: school-placed or self-placed. In a school-placed model, the program coordinates clinical sites and matches you with a preceptor. This reduces the burden on you but may limit flexibility in location or specialty. Self-placed rotations, on the other hand, put you in the driver's seat: you are responsible for finding a preceptor and site that meet program requirements. While this gives you more control, it can be daunting. If you are enrolled in a distance-learning track, our guide on online programs and local clinical placements walks through the logistics in detail. The current preceptor shortage has pushed many programs toward the self-placed model, so even if your program assists, being prepared to network on your own is wise.
A Realistic Timeline for Securing a Preceptor
Start your search four to six months before rotations are scheduled to begin. This allows time for initial outreach, follow-ups, and the administrative steps that follow. Once a preceptor agrees, the credentialing and affiliation agreement process can take 8 to 12 weeks. Identify two or three backup sites early to avoid scrambling if your first choice falls through. Align your timeline with the academic calendar: for summer rotations, begin looking in winter; for fall, start in spring.
Outreach Strategies That Work
- Start with your network: Reach out to NPs, physicians, or clinical educators you know. Colleagues from your current workplace are often willing to help.
- Tap professional organizations: The AANP, state NP associations, and specialty nursing groups frequently have member directories or mentorship programs. Attend conferences and local chapter meetings to build relationships.
- Approach providers directly: Polished, personalized emails or phone calls to practices in your area can open doors. Explain why you're interested in their specialty and what you hope to learn.
- Consider third-party placement services: Companies like Preceptor Link, NPHub, and Clinical Placement Solutions match students with preceptors for a fee. As of 2026, costs typically range from $2,000 to $5,000 per rotation depending on specialty and location. Factor this into your budget early if you anticipate needing paid assistance.
- Use your school's resources: Even in self-placed programs, faculty may have lists of prior preceptors or alumni who are open to taking students. Don't assume you're entirely on your own.
What to Look For in a Quality Preceptor
Not every willing NP or physician is the right fit. Seek a preceptor who is board-certified in your target population focus (for example, family, adult-gerontology, or psychiatric-mental health) and actively practicing in that role. Students pursuing a family nurse practitioner program, for instance, should confirm the preceptor's panel reflects outpatient primary care. The ideal preceptor:
- Enjoys teaching and has experience with students.
- Practices in a setting with sufficient patient volume and variety to expose you to common conditions and procedures.
- Works in an environment that aligns with your certification exam requirements (for instance, outpatient primary care for FNP students).
- Has clear communication and realistic expectations.
A quick phone call or in-person visit can reveal whether the practice fit feels right. Trust your instincts: a supportive, hands-on preceptor is worth far more than a prestigious name on your resume.
Build Strong Relationships With Your Preceptor and Clinical Team
As nurse practitioner education shifts heavily online, the clinical relationship you build with your preceptor now carries more weight than any lecture or simulation. It is the direct pipeline to competence, references, and job offers.
Your Preceptor Is Your Most Important Asset
A preceptor shapes your clinical judgment, advocates for you, and often becomes the first call when a practice has an opening. Treat this relationship as the single most important factor in your clinical success. The NP community is small, and a preceptor who trusts your work will refer you to colleagues, invite you into professional networks, and vouch for your skills. Many students secure their first NP position directly through a preceptor connection. Protect and nurture that relationship from day one.
Start the Conversation Before Day One
Reach out via a short, professional email a week before rotations begin. Introduce yourself, summarize your nursing background, and share two or three specific learning goals for the rotation. This gives the preceptor a framework for tailoring your experience. Early in the first week, ask directly how your preceptor prefers to give feedback (written notes, real-time debriefs, or end-of-week summaries) and what communication style works best during busy clinic hours. Schedule a short weekly check-in to discuss progress, cases that challenged you, and any gaps you need to address. This proactive habit signals maturity and makes feedback a normal part of the process, not a corrective event.
Show Up Prepared and Stay Curious
Nothing impresses a preceptor more than a student who does the preclinical work. Before a scheduled patient visit, review the chart and have a working differential in mind. Formulate thoughtful questions to ask between patients, not during the encounter when the preceptor is focused on workflow. Volunteer for procedures you find uncomfortable or unfamiliar, such as suturing, incision and drainage, or joint injections, and let your preceptor walk you through them. This demonstrates initiative and a learner mindset. After a difficult case, ask what clinical pearls the preceptor would want a new NP to remember. These exchanges build mutual respect and accelerate your clinical reasoning.
Cultivate Your Network Beyond the Preceptor
Meaningful professional connections extend to the entire clinical team. Learn the names and roles of the medical assistants, front-desk staff, nurses, and office manager. A medical assistant who trusts you will pull you into an interesting case or cue you about the patient's mood. The office manager might know which local practices are hiring before a position is posted. Specialists who see your collaborative attitude during a patient referral may later welcome you as a colleague, whether you pursue a path as an emergency nurse practitioner or land in primary care. In the NP world, these horizontal relationships often become the foundation of a career-long referral network and a source of future job opportunities.
Master Patient Communication and Clinical Presentations
Strong clinical presentations and patient communication skills distinguish competent NP students from those who earn enthusiastic recommendations and job offers. These abilities directly impact patient outcomes and determine how much autonomy your preceptor grants you throughout your rotation.
Use the SBAR Framework for Clinical Presentations
Most preceptors expect you to present patients using the SBAR format: Situation, Background, Assessment, and Recommendation. This structure appears frequently on certification exams and mirrors how practicing NPs communicate with physicians and specialists.
When presenting, lead with the situation (why the patient is here today), provide relevant background (pertinent medical history, current medications, allergies), state your assessment (what you believe is happening clinically), and offer a recommendation (your proposed plan). Keep presentations concise, typically under two minutes, while including all clinically relevant information.
Practice SBAR presentations at home using patient scenarios before your rotation begins. Record yourself, listen for unnecessary tangents or missing details, and refine your delivery until it feels natural.
Develop Patient Communication That Builds Trust
Several communication techniques separate exceptional students from adequate ones:
- Motivational interviewing: Use open-ended questions and reflective listening to help patients articulate their own reasons for change, particularly with lifestyle modifications or chronic disease management.
- Health literacy adjustments: Assess each patient's understanding level and adapt your explanations accordingly. Avoid medical jargon with patients who seem confused, and provide written instructions for complex regimens.
- Delivering difficult news: Pause after delivering a diagnosis, allow silence for the patient to process, and follow with clear next steps rather than overwhelming them with information.
- Managing disagreement: When patients refuse recommended care, explore their concerns without judgment. Document the conversation thoroughly and offer alternatives when appropriate.
Prioritize and Triage Your Patient Schedule
Learning to manage a full patient schedule requires deliberate prioritization. Review your schedule before patients arrive, identifying potential red-flag presentations that may need immediate escalation, such as chest pain, sudden neurological changes, or signs of sepsis. These patients should be seen first regardless of appointment order.
Document in real time rather than saving notes for the end of the day. Even brief shorthand entries between patients prevent the overwhelming documentation pile that leads to burnout and errors. Your preceptor can advise on efficient documentation strategies specific to their practice. Students rotating through high-acuity settings like ICUs or emergency departments may find that working toward a critical care nurse practitioner certification sharpens these triage instincts even further.
Practice Clinical Reasoning Aloud
Preceptors evaluate your thought process, not just your final diagnosis. Verbalize your differentials systematically: state what you are considering, explain what findings support or refute each possibility, and describe the tests or history elements that would help narrow your list.
For example, when evaluating a patient with abdominal pain, walk through your reasoning: "I am considering appendicitis given the migration of pain and rebound tenderness, though the absence of fever and normal white count makes me less concerned. I want to rule out ovarian pathology given her age and last menstrual period timing."
This transparency helps preceptors identify gaps in your clinical reasoning early, when correction is most valuable.
NP Clinical Rotation Evaluation Methods and Competency Frameworks
How are NP students evaluated during clinical rotations, and what does it take to pass? Let's walk through the tools and frameworks your program will use to measure your growth.
Common Evaluation Methods in NP Clinicals
Your clinical performance will be assessed through a blend of formative and summative methods.1 The most frequent is the preceptor evaluation, a standardized form on which your preceptor rates your skills from novice to competent across domains like patient assessment, diagnosis, and professionalism.2 Many programs also use the Nurse Practitioner Student Competency Assessment (NPSCA), a rubric aligned with NONPF core competencies.3 For high-stakes skill demonstration, expect Objective Structured Clinical Exams (OSCEs) at critical points: pre-clinical, mid-program, and as a capstone.1 These simulated patient encounters test your ability to integrate knowledge under pressure. Increasingly, programs layer on Entrustable Professional Activities (EPAs), a conceptual framework that defines the tasks you should be trusted to perform independently by graduation, using a 4- or 5-level entrustment scale.2
Clinical Logging: Tracking Every Patient Encounter
Nearly every best online MSN nurse practitioner programs accredited program requires a detailed clinical log. You'll document each patient encounter in a dedicated platform like **Typhon, E*Value, EXXAT, or RXpreceptor**.4 Typical entries include diagnoses, procedures, patient demographics, and time spent. These logs verify that you meet required minimums for patient contacts and procedures across the lifespan, so meticulous logging is non-negotiable. Many sites require real-time entry, and some preceptors may co-sign your logs.
Malpractice Insurance: What Coverage Do You Need?
Coverage is typically a two-layer system: your school carries a blanket policy, but many clinical sites and states also mandate an individual student policy.5 Standard limits are $1 million per claim with a $3 million to $6 million aggregate.6 Verify with your program coordinator whether a personal policy is required and secure proof before your first clinical day. Some full-practice states have stricter facility requirements, so don't skip this step.5
Mid-Rotation Feedback: Don't Wait Until the End
The strongest students treat evaluation as an ongoing conversation. Request a brief mid-rotation check-in with your preceptor to ask, "What's one thing I can improve before the final evaluation?"1 This gives you time to adjust, shows professional maturity, and often leads to a stronger summative rating. If concerns arise, your program will typically create a remediation plan with targeted goals and resources.2
Navigating Common Clinical Rotation Challenges
Clinical rotations are among the most rewarding parts of your NP program, but they come with real obstacles that can catch you off guard if you are not prepared. Knowing the most common challenges ahead of time, along with practical solutions, helps you stay on track and get the most out of every clinical day.
Pros
- Have two or three backup clinical sites lined up so a preceptor cancellation does not derail your hours or timeline.
- Contact your clinical coordinator the same day a preceptor no-shows so they can help you find a replacement quickly.
- Document specific incidents in toxic or unsupportive clinical environments, including dates, quotes, and witnesses.
- Request reassignment through your program's formal process rather than trying to tough it out in a harmful setting.
- Batch your clinical days into consecutive blocks to reduce commute time and protect dedicated study days each week.
- Meal prep on weekends and set non-negotiable study blocks on your calendar so burnout does not creep up gradually.
- Talk with your employer early about schedule flexibility, since most nursing managers understand NP program demands.
- Review the ten most common diagnoses for each rotation specialty before your first day so you walk in with a baseline.
Cons
- Preceptor cancellations or last-minute schedule changes can cost you weeks of progress toward your required clinical hours.
- Toxic clinical environments with dismissive or hostile staff can erode your confidence and stall your learning.
- Juggling work shifts, clinical days, and coursework simultaneously puts you at high risk for physical and emotional burnout.
- Feeling underprepared for a new specialty rotation is common and can lead to anxiety that affects your clinical performance.
- Programs sometimes offer limited guidance on finding backup preceptors, leaving students to navigate the process alone.
- Peer support networks may be hard to access when classmates are spread across different clinical sites and time zones.
How Clinical Rotations Shape Your NP Career
Clinical rotations are working auditions that can determine where you practice, what specialty doors open, and who advocates for you throughout your career. The relationships, skills, and portfolio you build during clinicals become tangible assets the moment you start applying for jobs.
Rotations as Extended Job Interviews
Many nurse practitioners receive their first job offers directly from clinical rotation sites. Hiring managers see students in action over weeks or months, observing clinical reasoning, communication with patients, collaboration with staff, and ability to handle volume and complexity under supervision. A strong rotation performance carries more weight than any resume. Treat every shift as if the attending physician, office manager, or clinical director is evaluating you for a permanent role, because they often are. Show up early, stay late when appropriate, volunteer for challenging cases, and ask thoughtful questions. The student who demonstrates reliability, humility, and growth becomes the candidate leadership remembers when a position opens.
Strategic Rotation Choices Open Specialty Niches
Rotation placements influence which specialties you can realistically access after graduation. Students who complete rotations in underserved rural clinics, urgent care centers, cardiology practices, dermatology offices, or other specialized settings gain both procedural experience and professional credibility in those niches. Employers in competitive specialties favor candidates with documented rotation hours in their field. If you hope to work in dermatology, a rotation with a dermatology NP or physician builds the patient encounter logs, procedure counts, and references that distinguish your application. Similarly, rotations in federally qualified health centers or Indian Health Service sites open pathways to loan repayment programs and underserved-area positions that value that specific exposure. Students interested in musculoskeletal care, for example, can explore the orthopedic nurse practitioner pathway to understand how targeted rotation hours translate into a competitive application.
The Lasting Power of Preceptor Networks
Preceptors become professional references, collaborators, mentors, and connectors long after your rotation ends. A preceptor who trusts your clinical judgment will refer patients to you, recommend you for job openings, co-author case studies or quality improvement projects, and introduce you to colleagues across the region. Maintain these relationships intentionally after graduation by sending thank-you notes, sharing updates on your career progress, and offering to precept students yourself once you are practicing. The NP community is smaller and more interconnected than most students realize. The preceptor who supervised your family practice rotation may sit on a hospital credentialing committee five years later or know the hiring manager at your dream employer.
Your Clinical Portfolio as a Tangible Asset
The documentation you compile during rotations becomes a portfolio used in every job interview and credentialing application for the first several years of practice. Patient encounter logs that demonstrate breadth across age groups, diagnoses, and procedures reassure employers that you can handle their patient population. Procedure counts for suturing, joint injections, IUD placements, or other skills prove competency beyond the theoretical. Specialty exposure documented through rotation summaries and preceptor evaluations opens doors to niche roles, whether you are pursuing a women's health nurse practitioner career or another focused practice area. Keep meticulous records, request detailed evaluation letters, and organize your portfolio into a format that clearly shows the depth and variety of your clinical training. This portfolio answers the question every employer asks: what can you actually do on day one?
Frequently Asked Questions About NP Clinical Rotations
NP clinical rotations raise a lot of practical questions, especially for working nurses juggling school, shifts, and family life. Below are answers to the questions we hear most often, drawn from current program policies and national guidelines.
- How many clinical hours do you need for nurse practitioner programs?
- Most NP programs require a minimum of 500 direct patient care clinical hours, though many DNP programs now require 1,000 or more total practice hours. The exact number depends on your specialty and degree level. Family nurse practitioner tracks, psychiatric mental health programs, and acute care concentrations each set their own minimums. Your program handbook will spell out the precise requirement, and every hour must be documented and verified by a preceptor.
- Do NP students get paid during clinical rotations?
- In almost all cases, NP clinical rotations are unpaid. Paid rotation models are rare, and no major national organization such as the AACN currently endorses a standard paid rotation structure. To offset the financial strain, students commonly tap into scholarships, employer tuition reimbursement programs, and federal loan repayment options. If finances are a concern, talk to your program's financial aid office early in the process.
- How far in advance should I secure a clinical rotation site?
- Plan to begin your search at least six to twelve months before your rotation start date. Securing a site involves finding a willing preceptor, completing an affiliation agreement between your school and the clinical site, and clearing any credentialing requirements. Programs generally do not guarantee preceptor placement, so starting early gives you a buffer if your first option falls through.
- What is the hardest part of NP clinical rotations?
- Many students say the toughest part is managing time. Balancing 16 to 24 hours per week of clinical work on top of coursework and, often, a nursing job can be exhausting. Another common challenge is the transition from the RN role to the provider role, where you are expected to independently assess patients, form differential diagnoses, and present cases to your preceptor with confidence.
- Can I complete NP clinical rotations in a different state than my program?
- Yes, but it is conditional. Your program must have authorization to operate in the other state, often through the State Authorization Reciprocity Agreement (SARA). You will also need a valid RN license in the state where you plan to complete rotations, and a signed affiliation agreement must be in place between your school and the clinical site. Some programs, such as Ohio State University's MSN program, limit placements to in-state or adjacent authorized states.
- What happens if my preceptor cancels or my site falls through mid-rotation?
- Notify your program immediately. Most schools will work with you to identify a replacement site. Any clinical hours you have already completed are typically retained, and a term extension may be granted to help you make up lost time. At Washington State University's DNP program, for example, the student collaborates directly with faculty to arrange a new placement. You should never make a unilateral site change without formal discussion and program approval.
The success of your clinical rotations is not decided on your first day in clinic. It is built months in advance when you secure a preceptor, review specialty-specific content, and put support systems in place at home and work. Students who treat preceptor outreach like a job search and start six months early consistently report smoother placements and stronger mentor relationships. Every clinical shift is both a learning opportunity and a professional audition, so approach each day prepared to demonstrate the communication skills, clinical reasoning, and professionalism that will turn your preceptor into your strongest reference and advocate. If your first rotation is within six months, start your preceptor search today.