Most important takeaways…
- Affiliation agreements and malpractice verification must be finalized before any student arrives.
- Phased rotation models move students from observation to near-independent practice safely.
- Preceptors can earn CE credits, tax deductions, and tuition benefits as incentives.
Nurse practitioner program enrollment has climbed past 40,000 new graduates a year, yet AANP surveys consistently show students spending months cold-calling clinicians to line up the 500 to 1,000 supervised clinical hours their programs require. The bottleneck is not classroom capacity. It is preceptors.
For practicing NPs, physicians, and site administrators, the decision to host sits at the intersection of competing pressures: patient throughput, malpractice exposure, state-specific supervision rules, and the professional pull to train the next cohort. Compensation is inconsistent, ranging from unpaid goodwill arrangements to CE credits, tax deductions, or stipends of a few hundred dollars per rotation. That nurse practitioner shortage is reshaping how clinical sites approach precepting as a long-term commitment rather than a one-off favor.
Understanding NP program capacity helps explain why the demand for qualified preceptors keeps outpacing supply, and why your decision to host carries real weight for the profession.
What Does It Mean to Host an NP Student?
Hosting a nurse practitioner student means opening your clinical practice so a graduate nursing student can learn hands-on patient care under your direct guidance. You serve as a preceptor, a role that is distinct from the supervisory relationships found in other health professions and one that carries its own expectations, rewards, and responsibilities.
Precepting vs. Supervising: Why the NP Model Is Different
If you have experience working with medical residents, physician assistant students, or new-grad RNs, you already know something about clinical mentorship. Precepting an NP student, however, operates within a different regulatory and educational framework. Unlike physician residency, where graduated autonomy unfolds over several years within a single institution, nurse practitioner clinical rotations are compressed into a set number of hours arranged across one or more community-based sites. And unlike supervising a new RN, precepting an NP student involves guiding someone who is learning to assess, diagnose, and manage patients independently, not execute delegated tasks.
The goal is progressive independence. Early in the rotation, you may co-manage every encounter. By the end, the student should be initiating assessments, formulating differential diagnoses, and proposing treatment plans with you reviewing and co-signing. Your state's nurse practice act and the student's academic program outline the specific scope of what students may and may not do at each stage.
Who Are These Students?
Most NP students arrive with a BSN and at least some bedside nursing experience. They are enrolled in either a Master of Science in Nursing (MSN) or a Doctor of Nursing Practice (DNP) program, pursuing a specialty track such as Family NP, Psychiatric-Mental Health NP, or Adult-Gerontology NP. National accrediting bodies like CCNE and ACEN require a minimum of 750 direct clinical hours for NP programs,1 and certification bodies (ANCC and AANPCB) require at least 500 supervised clinical hours to sit for the board exam.2 In practice, many programs exceed 750 hours, particularly DNP tracks. That means your site may host a student for one rotation of a few hundred hours or serve as one of several clinical sites for nurse practitioner students across the student's program.
The Three-Party Relationship
Hosting an NP student involves a partnership among three parties, each with defined responsibilities:
- The academic program develops the curriculum, sets learning objectives, arranges affiliation agreements, and verifies that clinical hours meet accreditation standards.
- The clinical site and preceptor provide the learning environment, model clinical decision-making, evaluate student competency, and ensure patient safety.
- The student prepares for each clinical day, meets learning objectives, documents hours, and communicates openly about challenges or gaps in knowledge.
An affiliation agreement, sometimes called a clinical contract, formalizes these roles before the rotation begins. It spells out liability coverage, HIPAA compliance, and each party's obligations. If you have not seen one before, expect the student's program to initiate it.
Who Can Precept?
Preceptors are typically experienced NPs or physicians practicing in the same specialty as the student's track. Most programs look for clinicians with several years of practice experience and an active, unencumbered license. One added incentive: ANCC allows faculty and preceptors to count direct clinical supervision of NP students toward their own practice hour requirements for certification renewal, as long as the supervision occurs within the preceptor's NP role and population focus.3 That means the hours you invest in teaching can also help you maintain your own credentials. If you are weighing whether to take on this responsibility, see what NP preceptor compensation typically looks like before committing.
Step-By-Step: How to Set up Your Site to Host NP Students
As NP programs increasingly rely on community preceptors to provide clinical training, having a standardized setup process reduces administrative friction and sets the rotation up for success.
The Affiliation Agreement: Your Legal Foundation
The affiliation agreement is the contract between your practice and the university. It outlines responsibilities, liability coverage, and the scope of the student's activities. In most cases, the university initiates the agreement: a clinical placement coordinator sends a draft, and your site's legal or administrative contact reviews it. Turnaround varies from a few days to several weeks, depending on the complexity and whether your organization has an existing master agreement with the school.
Key elements to review include: - Insurance and indemnification: Verify that the university's malpractice coverage extends to the student and that the hold-harmless clause does not shift undue risk onto your practice. - Scope of practice: Ensure the agreement clearly states that the student practices only under your direct supervision, consistent with state regulations and your collaborative agreement. - Term and termination: Confirm the start and end dates of the rotation, and what happens if either party needs to end the placement early.
Negotiate only what truly matters. Most terms are standard, but if you need the university to provide additional documentation (like proof of HIPAA training) before the student starts, get that in writing.
Operational Onboarding: Getting the Student Ready
Once the agreement is signed, front-load the practical logistics. These details prevent first-day chaos and are easy to overlook.
- EMR access: Request a temporary login for the student at least two weeks before the rotation begins. Many systems require manager approval and IT tickets, so start early. Clarify what level of access the student needs: view-only, documentation with co-sign, or order entry under supervision.
- HIPAA training verification: The university typically provides this, but double-check that the student's certificate is current and on file with your compliance department.
- Background check and drug screen: Often handled by the school, but some clinical sites require recent results (within 90 days). Specify your policy in advance.
- Badge and parking: Arrange for a temporary ID badge and parking pass. These small gestures make the student feel welcome and reduce anxiety on day one.
Day One Orientation: Setting Expectations
A structured first-day orientation should include: - Site policies: Review hours, dress code, phone use, and confidentiality rules. - Population overview: Describe the typical patient mix, common conditions, and any special populations (e.g., pediatric, geriatric) so the student can prepare. Understanding nurse practitioner clinical hours and population expectations before day one helps students arrive ready to contribute. - Documentation standards: Walk through how notes are written, the use of templates, and co-signature workflows. - Emergency protocols: Cover fire drills, code blue procedures, and what to do if a patient decompensates.
Provide a one-page summary of these items so the student can refer back later. Assign a point person for questions during the first week, perhaps an office manager or a seasoned MA.
Plan Ahead: The Credentialing Timeline
Many sites underestimate how long credentialing takes. Start the process two to three months before the rotation start date. This includes time for the affiliation agreement, IT provisioning, and any internal approvals required by your health system. If your site requires the student to apply for a temporary license or for a supervisory form to be filed with the state board, build in an extra month. Delayed credentialing can derail the entire rotation, and most universities will not bend on NP clinical placement deadlines. If a placement does fall through late, understanding how to switch NP preceptors mid-rotation can help both parties navigate next steps quickly.
Questions to Ask Yourself
Legal Requirements, Liability, and Malpractice Coverage for NP Preceptors
Taking on an NP student adds a layer of legal complexity to your practice. While clinical education is foundational to the profession, you need to understand who carries coverage, where liability falls, and what state rules apply to supervisory arrangements.
Malpractice Coverage: Who Carries the Policy?
Most accredited NP programs secure professional liability insurance for students during clinical rotations. For example, Herzing University provides school-carried coverage for every enrolled student, and CCNE accreditation standards (effective January 2025) require programs to document proof of professional liability insurance from all parties involved in clinical education.1
However, coverage often operates in layers. A typical setup includes school-provided primary coverage, supplemental site policy, and sometimes an individual student policy.1 Preceptors should confirm minimum coverage limits in the affiliation agreement before signing. The current standard in most agreements is one million dollars per claim and three million dollars aggregate.
Do not assume your existing malpractice policy automatically covers trainee supervision. Some insurers require an explicit rider for student oversight.2 If you supervise a student who commits an error, your carrier may deny a claim if you did not disclose your precepting role. Call your insurer before you host your first student and confirm in writing whether a rider is needed and what it costs.
Vicarious Liability and Respondeat Superior
Under the legal doctrine of respondeat superior, an employer or supervising practitioner can be held liable for acts performed by a student under their supervision. This means that if an NP student makes a clinical decision that harms a patient, and that decision was carried out while you were serving as the preceptor, you may share responsibility even if the student holds separate insurance.
To mitigate risk, preceptors should validate every history and physical, review all labs and diagnostic studies personally, and co-sign every note and prescription.3 Documentation is your strongest defense. If a chart does not show your direct review and approval, a plaintiff's attorney will argue the student practiced independently.
State-Level Variation in Supervision and Collaborative Agreements
Preceptor requirements vary by state. In full practice authority states, an independent NP can serve as a primary preceptor without physician involvement. As of mid-2026, Oklahoma granted independent prescriptive authority in November 2025, New Jersey extended full practice authority to primary care and behavioral health NPs in March 2026, and New York's FPA deadline arrived in July 2026.4 In these states, a solo NP with FPA can host students without a collaborative agreement.
In restricted-practice states, a preceptor may need an active collaborative or supervisory agreement with a physician, even if the preceptor themselves is an experienced NP. Check your state board of nursing website for current nurse practitioner scope of practice standards before accepting a student.
Put It in Writing: Affiliation Agreements and Coverage Verification
Before any student sets foot in your clinic, review the affiliation agreement. Confirm which party carries primary and excess liability coverage, what the policy limits are, and whether the agreement indemnifies you in the event of a student-related claim. If the school or student policy excludes certain acts (for example, invasive procedures or prescribing controlled substances), clarify those exclusions and adjust your rotation structure accordingly.
Request a certificate of insurance from the school and keep it on file. If the student carries an individual policy, ask for a copy of the declarations page. This documentation protects you if a claim arises months or years later.
Recent Regulatory Changes Affecting NP Preceptors
The landscape shifted notably in 2025 and 2026. The CCNE accreditation standard requiring proof of liability insurance took effect in January 2025, tightening documentation requirements across all programs.1 On the legislative side, South Carolina repealed its preceptor tax credit effective January 2026,5 while states like Georgia and Hawaii continue to offer credits (Georgia's is $6,375 with no sunset date; Hawaii's APRN credit has been active since 2019).2 At the federal level, the proposed PRECEPT Nurses Act would provide a $2,000 tax credit to preceptors who supervise at least 200 hours, though as of mid-2026 the bill remains pending.6
These changes underscore the importance of staying current with both insurance and regulatory requirements as you host NP students.
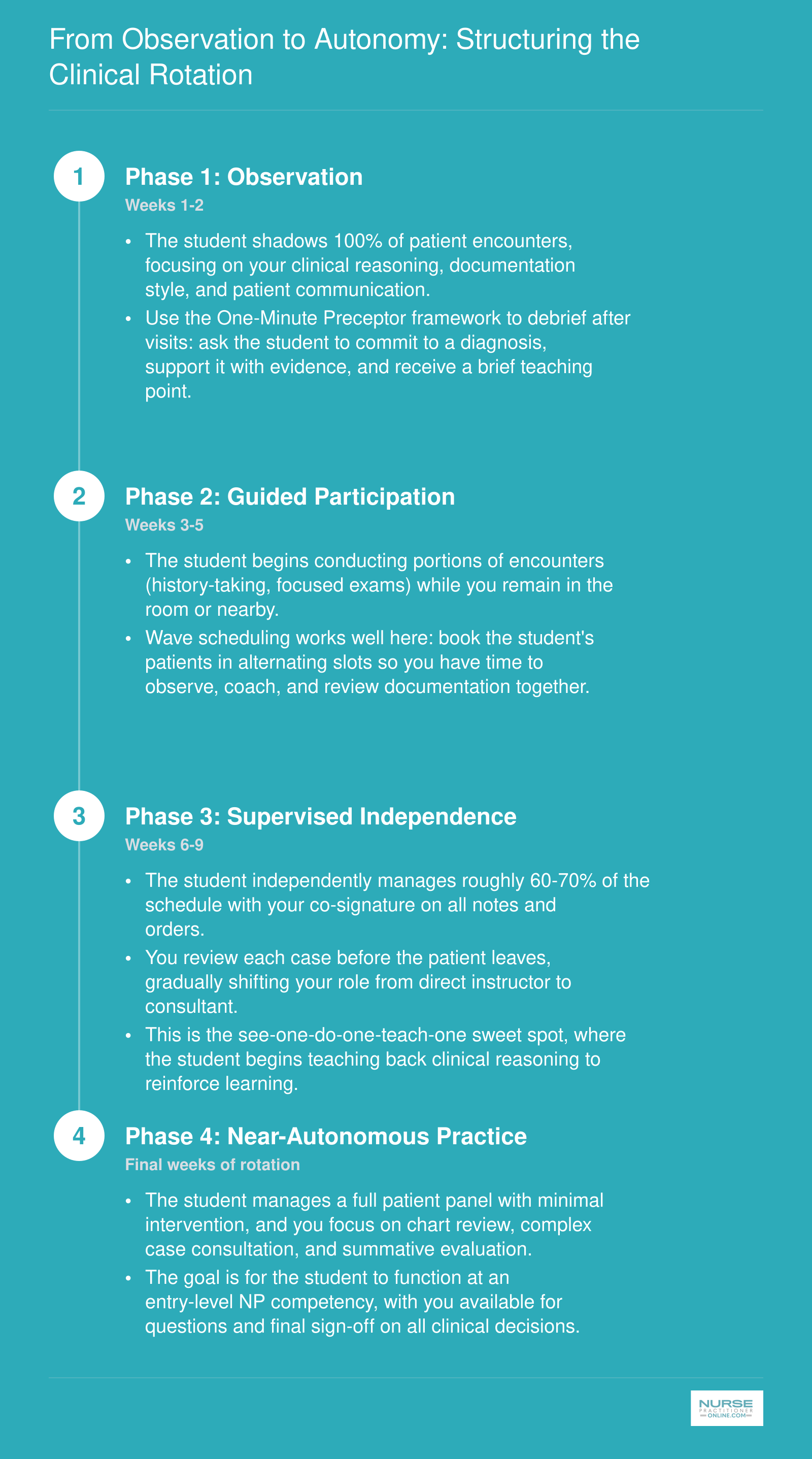
From Observation to Autonomy: Structuring the Clinical Rotation
A well-structured clinical rotation builds student competence gradually while protecting patient safety. Most successful preceptors use a phased model that moves students from passive observation to near-independent practice over the course of the rotation. Frameworks like wave scheduling, the One-Minute Preceptor model, and the classic see-one-do-one-teach-one approach fit naturally into this progression.
Teaching Strategies and Feedback Frameworks for NP Preceptors
Effective precepting is not lecturing at a student between patients; it is a deliberate practice built on adult learning principles, structured feedback models, and a clinical culture where asking questions is safer than hiding gaps.
Build on What the Student Already Knows
Every NP student walks into your clinic with years of bedside nursing experience. That foundation matters. Rather than treating a student like a blank slate, start each encounter by asking what they already know about the presenting complaint. Use Socratic questioning ("What diagnoses are you considering, and why?") instead of simply telling them the answer. This approach respects the student's professional identity while exposing the nurse practitioner differential diagnosis skills they still need to develop.
Real-time feedback at the point of care is far more powerful than a summary at the end of the week. When you notice a student missing a key assessment finding or ordering an unnecessary test, address it in the moment, briefly and without an audience. Waiting until a formal evaluation to mention a pattern you noticed weeks earlier frustrates students and wastes learning time.
Two Feedback Frameworks Worth Using
You do not need to reinvent the wheel. Two well-established models translate easily to a busy clinical day.
The One-Minute Preceptor model gives you a five-step sequence you can run through in roughly sixty seconds:
- Commit: Ask the student to state their assessment or plan.
- Probe: Follow up with "What led you to that conclusion?"
- Teach: Offer a brief teaching point tied to the case.
- Reinforce: Name what the student did well.
- Correct: Identify one specific area to improve.
The RIME framework helps you gauge where a student falls on the developmental continuum:
- Reporter: Can gather and present data accurately.
- Interpreter: Can synthesize findings into a differential.
- Manager: Can propose and begin executing a plan.
- Educator: Can teach back, cite evidence, and identify learning gaps.
Early in a rotation, most students operate at the Reporter or Interpreter level. Knowing where a student sits on this spectrum helps you calibrate your expectations and your teaching.
Create Psychological Safety
Students who fear being shamed in front of patients or staff will hide knowledge gaps instead of asking the questions that drive growth. Set the tone on day one: tell the student explicitly that you expect them to say "I don't know" when they do not know. Normalize uncertainty. Correct errors privately and without sarcasm. A preceptor who creates psychological safety will get more honest self-assessments, better clinical questions, and a student who progresses faster. Understanding how to tackle difficult conversations in clinical settings can also help you model composed, respectful communication for your student.
Establish a Consistent Feedback Cadence
Structure prevents important conversations from slipping through the cracks. A practical cadence looks like this:
- Brief morning huddle: Review the schedule, flag complex patients, set one learning goal for the day.
- Mini-debrief after complex cases: Two to three minutes to discuss clinical reasoning, differential refinement, or communication strategies.
- Formal mid-rotation evaluation: A sit-down review using the evaluation tool provided by the student's program. This is the time to document progress, reset goals, and address any concerns before they become end-of-rotation surprises.
- End-of-rotation evaluation: A comprehensive assessment aligned with the competency framework the program requires.
Know the Evaluation Tools
Most NP programs will send you their own clinical evaluation instrument, and you should use it. These tools are typically mapped to national competency frameworks. The AACN Essentials, revised in 2021, outline competency domains for both entry-level and advanced practice education.1 The NONPF NP Role Competencies, updated in 2022, define nine domains including Scientific Foundation, Independent Practice, Ethics, and Health Delivery System, among others.1
Some programs use the Nurse Practitioner Student Competency Assessment, a psychometrically validated, competency-based instrument aligned with both the AACN Essentials and the NONPF competencies.2 Others use program-specific tools. For example, some schools employ a four-point rating scale ranging from unsatisfactory to very good3, while others use a three-point scale that benchmarks performance as below expectations, appropriate for the student's level, or exceeding expectations.4 Evaluation frequency varies as well; some programs require assessments twice per semester.5
Regardless of which tool lands in your inbox, review it before the rotation starts. Understanding the competency domains the school is measuring helps you focus your teaching and ensures your feedback aligns with what the student will ultimately be graded on. If the school has not sent evaluation materials by the time the rotation begins, ask for them. You should never be guessing what "meets expectations" looks like. For a closer look at what students experience on NP clinical rotations, including hours and expectations, that context can sharpen how you pace your teaching across the rotation.
NP Student Evaluation Checklist: Core Competency Areas
A structured evaluation checklist helps preceptors provide consistent, objective feedback throughout a clinical rotation. The following competency areas align with national NP education standards and give you a practical framework for assessing student progress at key milestones during the placement.
| Competency Domain | What to Assess | Example Milestone Behaviors | Assessment Method |
|---|---|---|---|
| Health Assessment and Diagnosis | Ability to gather a thorough history, perform focused and comprehensive physical exams, and formulate accurate differential diagnoses | By midpoint, independently performs a complete H&P with minimal prompting; by rotation end, narrows differentials with confidence and clinical reasoning | Direct observation, chart review, oral case presentation |
| Clinical Reasoning and Decision Making | Critical thinking when interpreting findings, ordering diagnostics, and prioritizing problems | Moves from requiring step-by-step guidance early in rotation to proposing evidence-based plans independently by final weeks | Think-aloud exercises during patient encounters, written case analyses |
| Pharmacology and Prescribing | Knowledge of drug classes, dosing, contraindications, and patient education on medications | Accurately selects first-line agents for common conditions and identifies potential drug interactions before prescribing | Prescription review, verbal questioning on pharmacologic rationale, simulated prescribing scenarios |
| Patient Communication and Education | Rapport building, health literacy awareness, shared decision making, and culturally sensitive communication | Adapts language to patient education level, confirms understanding using teach-back methods, and addresses patient concerns empathetically | Direct observation during patient encounters, patient feedback when available |
| Professionalism and Ethical Practice | Timeliness, accountability, respect for interprofessional team members, adherence to HIPAA and informed consent protocols | Consistently arrives prepared, accepts constructive feedback without defensiveness, and maintains appropriate boundaries with patients and staff | Ongoing behavioral observation, self-reflection journals, midpoint and final evaluations |
| Procedural Skills (Specialty Specific) | Competence in hands-on procedures relevant to the clinical setting, such as suturing, joint injections, or incision and drainage | Progresses from assisted performance to independent completion of designated procedures with appropriate technique and documentation | Skills checklist with sign-off, direct supervision during procedures, return demonstration |
| Care Coordination and Systems-Based Practice | Understanding of referral processes, care transitions, insurance considerations, and interprofessional collaboration | Initiates appropriate referrals, follows up on pending results, and communicates effectively with specialists, social workers, and other team members | Chart audit for referral and follow-up documentation, team feedback, case management discussions |
| Evidence-Based Practice and Scholarly Inquiry | Ability to locate, appraise, and apply current research to clinical decisions | Identifies a clinical question during rotation and presents a brief evidence summary supporting a recommended practice change | Written evidence brief, journal article critique, integration of guidelines into care plans |
Related Articles
Handling Difficult Situations: Remediation, Patient Consent, and Boundaries
A student who needs extra coaching and a student who poses a patient safety risk call for very different responses, and knowing how to distinguish between the two is one of the most important skills a preceptor can develop. Most challenges fall somewhere on a spectrum, so having a clear framework before problems arise will help you respond with confidence rather than uncertainty.
When a Student Is Struggling: The Remediation Process
Knowledge gaps are normal, especially early in a rotation. If you notice a student consistently missing clinical reasoning steps or struggling with documentation, address it promptly rather than hoping things improve on their own.
- Document specific deficits. Note dates, clinical scenarios, and what the student did or failed to do. Vague concerns like "she just doesn't seem ready" are hard for anyone to act on.
- Contact the clinical coordinator early. The student's academic program has a stake in the outcome and likely has remediation protocols already in place. Reaching out is not a failure on your part; it is responsible mentorship.
- Create a written improvement plan. Include measurable goals (for example, "accurately complete three differential diagnoses without prompting by week four"), a clear timeline, and scheduled check-ins. Share this plan with the student and the program.
Unsafe clinical behavior is a different matter. If a student acts outside their scope, administers a medication without verification, or behaves in a way that puts a patient at risk, intervene immediately. Remove the student from the encounter, document everything, and contact the program's clinical coordinator the same day. Patient safety always takes priority over the student's feelings or academic progress.
Introducing Students to Patients and Handling Consent
Patients have a right to know that a student will be involved in their care, and they have a right to decline. A simple, direct introduction works best: "This is [name], a nurse practitioner student working with me today. They may ask you questions and participate in your exam with your permission." If a patient says no, thank them and excuse the student without further discussion.
Use your judgment about sensitive encounters. Conversations involving substance use, psychiatric crises, or reproductive health may warrant asking the student to step out even if the patient has not objected, particularly early in the rotation when trust between patient and student has not been established. Understanding simulation training for NP students can help you appreciate why some students arrive less prepared for emotionally charged clinical encounters than others.
Setting Boundaries Around Scope and Feedback
Scope-of-practice creep can happen gradually, especially with enthusiastic students. A student who begins ordering labs or making treatment recommendations to patients without your explicit direction has stepped beyond the preceptor-student relationship. Clarify expectations at the start of the rotation and revisit them as the student gains more independence.
Occasionally you will encounter a student who resists constructive feedback, becomes defensive, or dismisses suggestions. Address the pattern directly in a private conversation: explain that receiving and integrating feedback is a core professional competency, not optional. Conflict management in healthcare takes practice, and the strategies useful with patients apply here too. If resistance continues, loop in the clinical coordinator and document the conversations you have had. Protecting the learning environment, your patients, and your own professional standing all depend on your willingness to name difficult dynamics rather than work around them.
Benefits and Incentives for NP Preceptors
The time you invest in hosting an NP student can translate into professional and financial rewards that extend well beyond the clinical rotation. Many states, universities, and healthcare systems now recognize the shortage of preceptors by offering structured incentives that offset the administrative burden and opportunity cost of supervising learners.
Continuing Education Credit for Precepting
Many NP programs and state boards grant continuing education hours to preceptors, helping you meet certification renewal requirements while teaching. Some programs offer one CE contact hour for every ten to fifteen clinical hours supervised, although the exact ratio varies by institution. The ANCC, for example, requires 120 hours of precepting over a five-year cycle to satisfy part of its recertification pathway.1 Check with your student's university and your state board to confirm eligibility and documentation requirements, as many programs provide a certificate of completion at the end of each rotation.
Adjunct and Clinical Faculty Appointments
Several universities extend adjunct clinical faculty titles to active preceptors, granting access to library databases, online journals, professional development webinars, and a faculty email address. These appointments carry no salary obligation but add a recognized academic title to your CV and LinkedIn profile. To request an appointment, reach out to the program director or clinical placement coordinator when you first agree to host a student. The application typically requires a current CV, proof of licensure, and a brief statement of teaching interest. The title can be particularly valuable if you plan to pursue a DNP or teach part-time later in your career.
Financial Incentives: Stipends, Grants, and Tax Credits
A growing number of universities pay NP preceptors directly through community stipends. Amounts range from five hundred to fifteen hundred dollars per student per rotation, depending on the program, specialty, and contact hours. Academic medical centers and VA systems sometimes offer salary supplements of five hundred to five thousand dollars for preceptors who supervise multiple students over the course of a year.3
State-level tax incentives are expanding as well. Georgia's Preceptor Tax Incentive Program provides a three hundred seventy-five dollar tax credit per student, with an annual cap of six thousand three hundred seventy-five dollars.1 Virginia's Nursing Preceptor Incentive Program awards between five hundred and five thousand dollars for precepting twenty-five to two hundred fifty hours.2 Washington offers five hundred to one thousand dollars through its Student Nurse Preceptor Grants,4 and Arizona provides one thousand dollars through APRN Preceptor Grants.3 Tennessee's Hospital Association Nurse Preceptor Incentive pays up to fifteen hundred dollars per rotation.5
At the federal level, the PRECEPT Nurses Act, signed in 2025, allows a two thousand dollar tax credit for preceptors who complete at least two hundred hours of clinical supervision.6 You can claim this credit even if you also receive a university stipend, as long as you maintain proper documentation of hours and student progress.
Be aware that stipends and grants often require a formal agreement or memorandum of understanding between your practice and the university. Some states also mandate that you complete a preceptor training module before qualifying for tax credits or reimbursement.
Non-Financial Rewards and Professional Growth
Hosting NP students builds a recruitment pipeline. Many practices hire their former students once they graduate, saving thousands of dollars in recruiting fees and onboarding time. Students already know your workflows, patient population, and documentation standards, which shortens the orientation period.
Precepting also keeps you current with evidence-based practice. Students bring recent journal articles, updated clinical guidelines, and fresh perspectives on population health and social determinants. Explaining your clinical reasoning aloud sharpens your own diagnostic skills and can reveal gaps in your documentation or prescribing habits.
The professional reputation boost is tangible. Academic programs remember consistent, high-quality preceptors and refer colleagues when other sites need hosting. Your name may appear in program newsletters, advisory councils, and conference panels, raising your visibility in the NP community.
Telehealth Precepting as an Emerging Model
Some programs now accept a portion of clinical hours via synchronous telehealth supervision. In this model, the student conducts a telemedicine visit while you observe the video encounter in real time, either from another room or from a separate location. You remain available to answer questions immediately via chat or phone and co-sign the documentation. This arrangement can ease scheduling constraints and expand access to specialty preceptors in underserved regions. For a broader look at how virtual care is reshaping advanced practice, APRN telehealth trends in 2026 offer useful context. However, most programs cap telehealth hours at twenty to thirty percent of the total rotation, and not all state boards recognize virtual supervision for licensure requirements. Confirm the policy with your student's program before agreeing to remote oversight.
How Hosting NP Students Impacts Your Schedule and Productivity
Time burden ranks as the primary barrier cited by NP preceptors in national surveys,1 and the concern is understandable. Taking on a student means splitting your attention between patient care and teaching, at least initially. The good news is that the productivity dip is temporary, and the data shows most preceptors end up in a much better position than they expected.
The Early Weeks: Expect a Temporary Slowdown
During the first one to two weeks of a clinical rotation, plan for roughly 25 to 50 percent slower patient throughput. You will spend extra time orienting the student to your electronic health record, your documentation standards, your patient population, and the rhythm of your clinic day. National survey data indicates that NP preceptors work an average of two additional hours on precepting days during this phase.2 Only about 24 percent of NP preceptors reported a positive productivity impact during the first semester of working with a student.3
The Turning Point: Mid-Rotation and Beyond
As students gain competence, the calculus shifts. By the final semester of a rotation, a striking 80 percent of NP preceptors reported a positive impact on productivity, meaning the student was carrying enough of the patient load to offset or exceed the time spent teaching.3 For context, physician preceptors reported a positive impact at a rate of 68 percent during the same period.3 The takeaway is clear: the student's growing independence translates directly into shared workload.
By mid-rotation, many students are managing their own small panel of patients. You still review their assessments and plans, but the time per encounter drops considerably. Several preceptors describe this phase as net-neutral or even net-positive, with the student handling straightforward visits while the preceptor focuses on more complex cases. Preceptors who also deal with decision fatigue as a nurse practitioner often find this shared load especially welcome by the final weeks of a rotation.
Scheduling Strategies That Protect Your Pace
Smart scheduling is the single most effective way to minimize disruption.4 Consider these approaches:
- Wave scheduling: Cluster several patients in a block so the student can see two or three while you review charts and finalize notes from the previous wave. This keeps your own pace steady while giving the student meaningful clinical time.2
- Focused half-day blocks: Dedicate specific mornings or afternoons to precepting rather than spreading student encounters across the full day. Research shows this reduces the feeling of fragmentation and lowers perceived time burden.4
- Gradual load increases: Start the student with two to three patients per half-day and increase incrementally. By week four or five, many students can manage a near-full schedule with your oversight.
- Structured teaching models: The One-Minute Preceptor framework, a five-step method for bedside teaching, has been shown to increase time efficiency without adding a significant perceived time burden.5 It keeps teaching moments focused and prevents lengthy post-visit debriefs from eating into your schedule.
Simulated clinic models have also found that hosting two students simultaneously can actually decrease patient wait times while doubling non-face-to-face teaching time, all without increasing the preceptor's overall time burden.6 If your practice has the volume, pairing students is worth considering.
The Long View
Redesigning your schedule around precepting days is an investment, but it pays off. Most preceptors find that their patient load on precepting days remains unchanged or even increases once the student hits their stride.2 The weeks you spend orienting a new student are a short-term cost that yields a longer-term return: a capable new nurse practitioner who lightens your workload, brings fresh clinical questions that sharpen your own practice, and may eventually join your team as a licensed NP.
What Nurse Practitioners Earn Nationally
Competitive salaries are fueling record NP program enrollment, which in turn increases demand for qualified preceptors and clinical sites. Understanding the national pay landscape helps explain why the profession needs more practitioners willing to host students.

Frequently Asked Questions About Hosting NP Students
Below are answers to the questions preceptors and clinical site managers ask most often. Each response draws on the guidelines and strategies covered throughout this article.
- How many clinical hours do NP students need?
- Most NP programs require between 500 and 1,000 supervised clinical hours, depending on the specialty and the accrediting body. Some states or certifying organizations may set higher minimums. The student's university will provide a specific hour requirement and documentation forms. As a preceptor, you will verify completed hours and confirm the student met program expectations before signing off on the rotation. For example, pediatric clinical training follows its own hour benchmarks set by specialty accreditors.
- What are the legal responsibilities of an NP preceptor?
- Preceptors must ensure they have a current affiliation agreement with the student's program, verify that malpractice coverage extends to the student, and supervise care in a manner consistent with state regulations. You are responsible for reviewing the student's clinical decisions and cosigning documentation. As discussed earlier in this guide, confirming liability coverage before the rotation begins is essential to protecting both yourself and your practice.
- Do NP preceptors get paid or receive benefits?
- Direct payment for precepting is uncommon, though some programs offer modest stipends, nurse practitioner continuing education credits, adjunct faculty appointments, or tuition discounts. Several states have introduced tax incentives or grant programs to encourage precepting. Beyond financial perks, many preceptors cite professional development, staying current on evidence-based practice, and the satisfaction of shaping the next generation of nurse practitioners as meaningful benefits.
- What qualifications do you need to be an NP preceptor?
- Programs generally require preceptors to hold an active, unencumbered NP license (or physician license in the relevant specialty), a minimum of one to two years of clinical experience, and national board certification. Some universities also ask for a current curriculum vitae and completion of a brief preceptor orientation. Specific requirements vary by program and state, so confirm eligibility with the student's school before committing.
- How does hosting an NP student affect clinic productivity?
- Expect a temporary dip in your personal productivity during the first few weeks while the student orients to your workflow. As detailed in the scheduling section of this guide, a gradual progression from observation to semi-autonomous practice helps the student contribute meaningfully over time. Many preceptors find that by mid-rotation, a well-prepared student actually lightens the workload by handling intake assessments, patient education, and follow-up documentation.
- What should an NP preceptor do if a student is not performing well?
- Address concerns early with specific, documented feedback using the competency-based evaluation checklist outlined in this article. Hold a private conversation to set clear improvement goals and a realistic timeline. If performance does not improve, contact the student's faculty liaison to discuss a formal remediation plan. Keeping written records of feedback sessions and clinical incidents protects both you and the student throughout the process.
- Can NP students participate in telehealth visits during clinical rotations?
- Yes, many programs now accept telehealth encounters as part of the clinical rotation, though policies vary by school and state. The preceptor should confirm with the student's program whether virtual visits count toward required hours and what documentation is needed. During telehealth sessions, the student should participate in real time while the preceptor observes or co-manages the visit, maintaining the same supervisory standards as in-person care. Understanding how to demonstrate telehealth skills in an NP interview can also help students articulate this experience as they enter the job market.