Most important takeaways…
- Accredited pediatric NP programs require a minimum of 750 clinical hours, with many exceeding 1,000 hours total.
- Primary care and acute care PNP tracks lead to different scopes of practice, certification exams, and clinical settings.
- Part-time PNP enrollment adds one to two years but lets working nurses keep their income during clinical rotations.
- Preceptor sourcing varies widely by program, so confirming placement support before enrolling protects your timeline.
Pediatric nurse practitioner students must complete at least 750 supervised clinical hours before board certification, but that number understates the real work. Clinical rotations are where a working nurse refines the ability to recognize a subtle heart murmur in an infant or to gently obtain a sexual history from an adolescent, skills that no pre-recorded lecture can teach. For nurses balancing a job while researching online PNP programs, clinical training is not an afterthought; it's the part that will strain your calendar and sharpen your instincts. Programs that pair rigorous simulation hours with well-vetted preceptorships tend to produce graduates who walk into their first pediatric practice with grounded confidence, not textbook theory.
How Many Clinical Hours Do Pediatric NP Programs Require?
The minimum clinical hour requirement for nurse practitioner programs has evolved significantly over the past decade, with the floor rising from 500 to 750 hours as national accreditors and professional organizations standardized advanced practice education.1 Today, nearly all accredited pediatric nurse practitioner programs meet or exceed the 750-hour threshold set by the National Organization of Nurse Practitioner Faculties (NONPF) and endorsed by the American Association of Colleges of Nursing (AACN), and many programs intentionally build in hundreds of additional clinical contact hours to deepen student readiness.
Current Minimum Standards Across Degree Pathways
The 750-hour minimum applies uniformly across MSN PNP programs, DNP-level PNP programs, and post-master's certificate pediatric nurse practitioner tracks as of 2024.1 Legacy programs that required only 500 hours have largely updated their curricula to align with the current standard.2 Programs seeking initial or continuing accreditation from the Commission on Collegiate Nursing Education (CCNE) or the Accreditation Commission for Education in Nursing (ACEN) must demonstrate compliance with the 750-hour floor. In practice, many programs set internal minimums between 600 and 800 hours for MSN pathways, while DNP programs frequently require 1,000 or more total clinical hours when you combine specialty clinical training with the DNP scholarly project.
How Clinical Hours Accumulate Across Semesters
Clinical hours typically ramp across the program timeline. Early rotations often emphasize observation, health assessment, and supervised encounters, with students completing 8 to 12 hours per week. Mid-program semesters shift toward direct patient care under preceptor guidance, often requiring 16 to 20 hours weekly, and final semesters focus on independent patient management with preceptor oversight, sometimes reaching 24 or more hours per week. This progression mirrors the way you built competence as an RN, moving from task-focused care to independent clinical reasoning.
Direct Patient Care vs. Total Clinical Hours
Not all clinical hours involve direct patient contact. Accreditation standards distinguish between direct patient-care hours (face-to-face assessment, diagnosis, treatment planning, and follow-up) and broader clinical experiences such as simulation lab sessions, interprofessional case conferences, quality-improvement activities, and pediatric grand rounds. Some programs count high-fidelity simulation toward the 750-hour minimum, while others require that the full minimum consist of direct patient encounters and log simulation separately. When you compare programs, ask explicitly how they define and allocate clinical hours so you understand what you will actually be doing in those 750-plus hours.
Comparing Program-Specific Hour Totals
Although accreditation bodies set minimum thresholds, individual programs often exceed them to strengthen graduate outcomes and employer confidence. One program may require exactly 750 hours, while another builds a curriculum around 900 hours to ensure students rotate through a wider variety of clinical settings or patient populations. When researching accredited online pediatric nurse practitioner programs, review each program's published clinical hour total and look for detail about whether those hours include both primary-care and acute-care pediatric rotations if you are pursuing a dual-focus track. Higher hour counts are not always better if they come at the expense of scheduling flexibility or work-life balance, but they do signal a program's commitment to hands-on preparation.
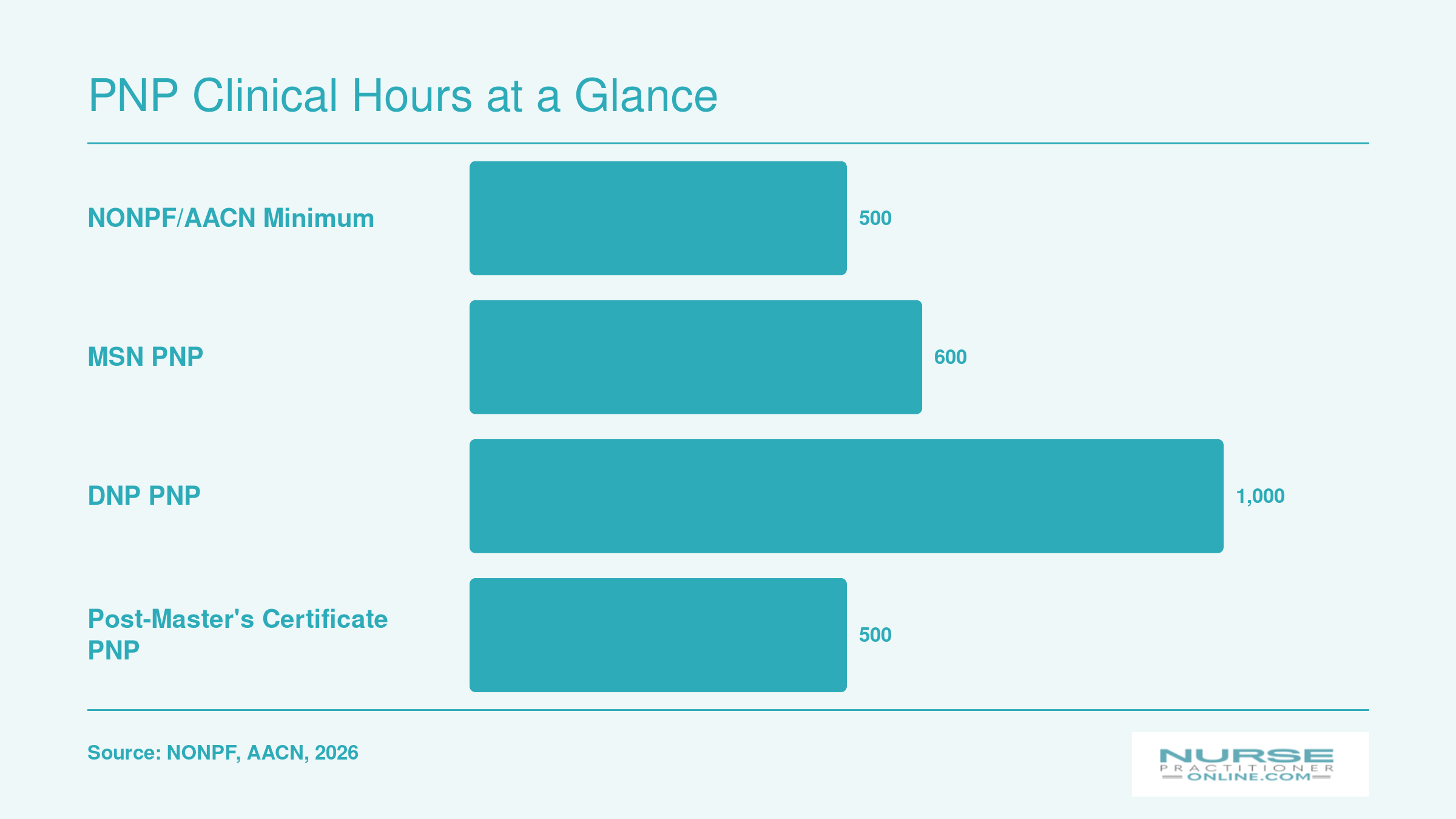
PNP Clinical Hours at a Glance
Clinical hour requirements vary by program type and degree level, but all accredited pediatric nurse practitioner programs must meet the minimum floor set by national accrediting bodies. Here is how the three most common PNP pathways compare.
Primary Care Vs. Acute Care PNP Clinical Tracks
Choosing between the primary care (PNP-PC) and acute care (PNP-AC) tracks is one of the most important decisions you will make as a pediatric nurse practitioner student. Each track prepares you for a distinct scope of practice, and the clinical rotations reflect that difference from day one. Understanding how these tracks compare across settings, skills, and career outcomes will help you pick the path that fits your professional goals and nursing background.
| Dimension | PNP, Primary Care (PNP-PC) | PNP, Acute Care (PNP-AC) |
|---|---|---|
| Primary Clinical Environment | Outpatient and ambulatory settings such as pediatric offices, school-based clinics, and community health centers | Inpatient and high-acuity settings including PICUs, NICUs, pediatric emergency departments, and specialty inpatient units |
| Patient Focus | Well-child visits, common acute illnesses, and stable chronic conditions | Acute, critical, complex, and unstable pediatric patients |
| Typical Skills Emphasized | Developmental surveillance, anticipatory guidance, immunization management, and chronic disease management | Advanced physical assessment, bedside procedures, ventilator management, and stabilization of critically ill children |
| PNCB Minimum Clinical Hour Requirement | At least 500 supervised primary care hours | Varies by program with a required acute care focus |
| Certification Exam | CPNP-PC (administered by the Pediatric Nursing Certification Board) | CPNP-AC (administered by the Pediatric Nursing Certification Board) |
| Typical Applicant Background | Prior pediatric RN experience is recommended but not strictly required | At least two years of acute pediatric RN experience is strongly preferred |
| Common Career Settings After Graduation | Private pediatric practices, federally qualified health centers, school health programs, and public health departments | Children's hospitals, neonatal intensive care units, pediatric trauma centers, and subspecialty inpatient services |
Types of Clinical Rotation Settings for PNP Students
Where will you actually spend your clinical hours as a pediatric nurse practitioner student?
Pediatric NP programs rotate students through a wide variety of settings to build the breadth of experience you'll need in practice. You won't stay in one clinic for your entire program. Instead, expect to move through multiple environments, each teaching different aspects of pediatric care and population health.
Primary Care and Outpatient Settings
Most students complete substantial hours in pediatric primary care offices, where you'll see well-child visits, manage common acute illnesses, and handle chronic disease management. Community health centers serve as another core rotation site, often exposing you to diverse patient populations and social determinants of health. School-based health clinics offer a unique window into adolescent care, mental health screening, and preventive services in an educational setting. Many programs also include urgent care rotations, where you'll develop decision-making skills for acute pediatric presentations that fall between primary care and emergency settings.
Specialty and Hospital-Based Rotations
Pediatric specialty clinics round out your training. Depending on your program and local resources, you may rotate through endocrinology (managing diabetes and growth disorders), pulmonology (asthma, cystic fibrosis), cardiology, gastroenterology, or other subspecialties. These rotations teach you when and how to refer, and help you recognize complex conditions early.
For students in acute care pediatric nurse practitioner programs, hospital-based units become central: pediatric intensive care units, neonatal intensive care units, and pediatric emergency departments. Even primary care track students typically complete at least one hospital rotation to understand inpatient care and continuity across settings.
Rural and Underserved Requirements
Some programs require rotations in rural or underserved areas, recognizing that these communities face provider shortages and unique access challenges. This exposure helps you understand care delivery outside well-resourced urban centers and prepares you to serve populations with limited healthcare infrastructure. Programs in states with significant rural populations often emphasize this component.
Geographic Flexibility in Online Programs
Online and hybrid PNP programs frequently allow students to complete clinical rotations in their home communities, which helps working nurses maintain their current jobs and family responsibilities. However, geographic constraints vary. Some programs have preceptor networks only in certain states, while others support placements wherever state nursing regulations and program accreditation standards allow. Always verify a program's clinical placement support in your specific region before enrolling.
Questions to Ask Yourself
Finding Preceptors and Securing Clinical Placements
Two paths stand between you and the clinical hours that define your pediatric nurse practitioner training: school-arranged placements, where the program takes the wheel, and student-sourced placements, where you drive the search. The path you walk can shape your entire timeline and stress level.
How Placement Models Differ
In a school-arranged model, the program's clinical coordination office does the heavy lifting. They identify sites, vet preceptors, and secure a spot for you. This is common in well-established programs with deep community ties and dedicated placement staff.1 Hybrid or assisted models fall in between: the school may provide a list of approved preceptors or help with initial contacts, but you still play an active role in finalizing arrangements. Student-sourced models shift the burden entirely to you. You must find a board-certified pediatric NP or physician willing to supervise your hours, often with nothing more than a list of requirements and a deadline.
If You Need to Self-Source
Self-sourcing demands early networking and persistence. Start tapping your professional circle months before your clinical rotations begin. Leverage current employer relationships, as your workplace may already have pediatric providers who precept. Cold-call or email local children's hospitals, private pediatric practices, and community health centers. Ask program alumni for referrals; they've walked this road and often know which preceptors are open to students. For a deeper look at strategies that work, see our guide on how online nursing programs arrange local clinical placements. Join online PNP student groups and professional networks, where preceptor leads are frequently shared.
Be strategic: have a polished CV and a brief pitch ready that explains your clinical goals and timeline. Follow up politely but consistently. The search can take weeks or even months, so plan ahead.
Why Program Support Matters
Preceptor shortages in pediatric specialties are a genuine hurdle. Limited sites, busy clinicians, and competition from other NP students can delay your progress. Programs with established clinical partnerships and dedicated placement coordinators absorb much of this friction.2 National nursing organizations like NONPF and AACN encourage coordinated partnership models, where schools build formal preceptor networks rather than leaving students to fend for themselves. This is not just a convenience; it's a retention and completion issue. Before enrolling, ask programs directly: "What percentage of your PNP students are placed by the school?" and "What is the average time from request to confirmed placement?" The answers can reveal whether you'll be spending your energy on learning or on logistics.
Clinical Objectives and Core Skills You'll Develop
Clinical objectives are the specific, measurable skills and competencies pediatric nurse practitioner students must demonstrate during patient-care rotations. They transform classroom theory into hands-on ability, ensuring you are ready to manage young patients safely and effectively by graduation.
Competency Domains Evaluated During PNP Clinicals
Preceptors and faculty assess your progress across several core domains:
- Health assessment across developmental stages: Conducting age-appropriate physical exams on infants, toddlers, school-age children, and adolescents, including neurodevelopmental evaluation.
- Differential diagnosis: Formulating and ranking possible causes of symptoms, using critical thinking to rule out serious conditions.
- Evidence-based treatment planning: Designing management strategies aligned with current guidelines, from prescribing medications to coordinating referrals.
- Developmental screening: Performing structured screenings (e.g., ASQ, M-CHAT) and interpreting results to identify delays early.
- Immunization management: Applying CDC schedules, managing catch-up vaccines, and counseling hesitant families.
- Family-centered communication: Adapting explanations to caregivers' health literacy, addressing psychosocial concerns, and engaging patients in shared decision-making.
How Clinical Objectives Build Across Rotations
Early rotations emphasize focused history-taking, systematic physical exam technique, and identifying normal versus abnormal findings. You learn to gather data concisely and recognize red flags. Mid-program, expectations shift to formulating a nurse practitioner differential diagnosis and proposing initial management plans for common pediatric conditions. Advanced rotations expect you to independently manage a small patient panel, integrating behavioral, social, and chronic disease considerations. By the final semester, you should handle complex cases, such as a medically fragile infant or a teenager with multiple comorbidities, with minimal prompting, demonstrating clinical reasoning that mirrors experienced practitioners.
Procedural Skills You'll Practice
Specific hands-on skills vary by track (primary care vs. acute care) and site, but commonly include:
- Otoscopic exams: Correctly visualizing the tympanic membrane and identifying infections or effusions.
- Point-of-care testing interpretation: Using and interpreting rapid strep, influenza, urine dipstick, glucose, and other tests.
- Newborn assessments: Performing thorough physical exams, evaluating feeding, and screening for congenital conditions.
- Suturing (acute care track): Wound closure and laceration repair in urgent or emergency settings.
- Lumbar puncture assistance (acute care track): Positioning the patient, collecting specimens, and monitoring during the procedure.
Every skill is practiced under supervision until both you and your preceptor are confident in your independent ability.
Documenting Competency: Logs and Evaluations
PNP programs use two primary tools to verify progress. Preceptor evaluations are completed at mid-rotation and end-of-rotation, grading you on specific competencies with written feedback. You also maintain a detailed clinical log, tracking patient encounters, demographics, diagnoses, and procedures performed. Programs set minimum benchmarks, for example, a required number of well-child visits or acute-care cases, that you must meet before advancing to the next clinical phase. Understanding the role of the nurse practitioner student in clinical rotations can help you approach these requirements with the right mindset. These records not only keep you on track but also become part of your portfolio for certification and licensure.
Related Articles
Simulation Labs and Technology in PNP Training
Simulation has become a cornerstone of pediatric NP education, giving you a safe space to build confidence before you touch your first real patient in a rotation. Here's how modern programs use it, and where the limits sit.
High-Fidelity Pediatric Manikins
Most PNP programs now train with a range of pediatric manikins (infant, toddler, and school-age) that breathe, cry, mottle, seize, and respond to medications in real time. You'll work through scenarios you cannot ethically rehearse on a sick child: a wheezing toddler sliding into respiratory failure, a febrile infant tipping toward septic shock, an anaphylactic reaction during a routine immunization visit. Faculty can pause the scenario, debrief your clinical reasoning, and rerun it until your assessment and intervention sequence feels automatic. By the time you encounter the real thing in a pediatric ED or urgent care rotation, your hands already know where to go.
Accreditation Limits: Supplement, Not Substitute
Simulation is powerful, but it is not a shortcut. CCNE and ACEN do not publish a hard numeric cap on simulation hours for graduate NP programs, yet both are explicit that simulation cannot replace direct patient care.12 National APRN certification bodies still require a minimum of 500 direct patient care hours, and AACN reinforces that virtual or simulated experiences supplement rather than substitute for hands-on practice.3 The NCSBN's well-known 50% simulation guideline applies to prelicensure RN education, not advanced practice training, so be wary of programs that wave that number around.4 ACEN further requires programs to report simulation hours separately from clinical hours, which helps maintain transparency.5
When comparing MSN pediatric nurse practitioner programs, pay close attention to how each program distinguishes simulation time from direct patient care hours in its curriculum.
Telehealth and Immersion Weekends
Telehealth simulation is the newest addition, and it matters most for primary care PNP students who will increasingly run virtual well-child follow-ups, lactation check-ins, and behavioral health screenings. Practicing a video-visit physical exam, including coaching a parent through an otoscope-free ear assessment, is a teachable skill.
If you're in an online or hybrid program, expect simulation to be front-loaded during on-campus immersion weekends, usually one to three intensives before your first direct care rotation begins. Take them seriously: they are your dress rehearsal.
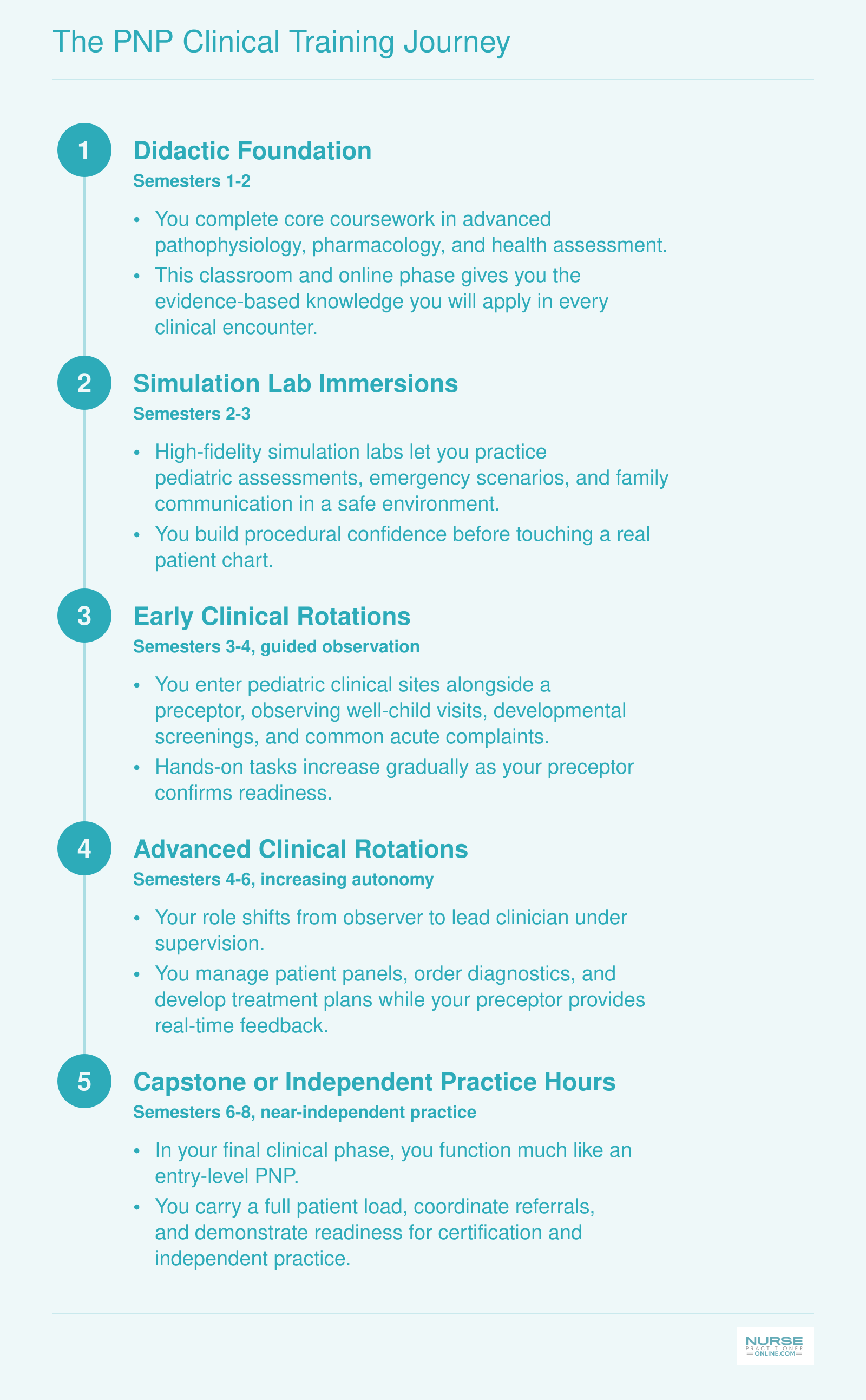
The PNP Clinical Training Journey
Most MSN-level Pediatric Nurse Practitioner programs follow a structured progression that builds your confidence and competence over roughly six to eight semesters. Here is what that path typically looks like, stage by stage.
Balancing Clinical Rotations With Work and Life
Most nurses entering a PNP program are already managing full-time jobs, families, and the quiet exhaustion that comes with bedside work. Fitting clinical rotations into that reality takes deliberate planning, not wishful thinking.
Part-Time vs. Full-Time Pacing
One of the most practical choices you will make is how quickly to move through your program. Many accredited PNP programs allow students to spread clinical hours across additional semesters, which lowers the weekly burden considerably. A full-time student might complete rotations in two to three semesters of concentrated scheduling, while a part-time student might stretch that same workload across three to four years. Neither path is wrong. The right choice depends on your current job demands, your financial situation, and how much runway your employer is willing to give you.
Some programs have also expanded their rotation options to include weekend blocks or evening clinic sites, particularly in primary care settings. If schedule flexibility is a top priority for you, ask programs directly about these options before you commit.
Practical Tactics for Working Nurses
A few strategies consistently help working nurses get through clinical-intensive semesters without burning out:
- Shift negotiation: Talk to your nurse manager early, ideally before your first clinical semester begins. Many managers will adjust your shifts if they understand the timeline and can plan coverage in advance.
- Strategic PTO use: Identify your most demanding clinical rotations ahead of time and reserve paid time off for those weeks rather than spreading it evenly across the year.
- Preceptor communication: Most preceptors have worked with students who hold jobs. Being upfront about your availability at the start of a rotation usually leads to a more workable schedule than trying to adjust it midway through.
Tuition Reimbursement and Employer Support
Before you enroll anywhere, spend time investigating what your employer actually offers. Many hospital systems and large outpatient practices provide tuition reimbursement or schedule accommodations for nurses pursuing graduate degrees, but these benefits are often underused simply because nurses do not ask about them. Human resources departments and nurse managers are both good starting points for that conversation.
Even partial reimbursement can reduce financial pressure significantly, and a supportive employer can make the difference between finishing your program on time and putting it on hold.
How to Evaluate a PNP Program's Clinical Training Quality
Some programs advertise clinical training prominently; others bury the details in fine print. Knowing how to read between the lines protects you from choosing a program that looks strong on paper but leaves you scrambling for placements or underprepared for certification.
Start With Accreditation
Accreditation by either CCNE or ACEN is not optional. It is a hard requirement for sitting for both the PNCB and ANCC pediatric NP certification exams.1 A program without one of these credentials disqualifies you from those exams regardless of how many clinical hours you complete. Confirm accreditation status directly through each accrediting body's public database before you apply anywhere.
Use Certification Pass Rates as a Quality Signal
Once you confirm accreditation, certification pass rates become one of the most honest indicators of clinical preparation quality. According to 2024 PNCB data, the first-time pass rate for the primary care exam (CPNP-PC) was 80.69% across 1,318 candidates, while the acute care exam (CPNP-AC) came in at 69.57% across 691 candidates.2 Those numbers are the national benchmarks. Programs that consistently outperform them tend to have more rigorous clinical structures behind them.
For the acute care track in particular, the spread across programs is wide. Data from 2022 shows that 63% of programs achieved first-time pass rates of 80% or higher on the CPNP-AC, while 24% of programs came in at or below the national average.3 That gap reflects real differences in clinical preparation. Ask programs directly for their most recent cohort pass rates, not just aggregate numbers.
ANCC does not publish pediatric NP pass rates publicly, so if you are considering a program that prepares you for the ANCC pathway, focus your due diligence on the structural quality indicators below.4
Look Beneath the Pass Rate Numbers
Pass rates tell you the outcome. These questions help you understand why:
- Faculty-to-student ratio in clinical oversight: Lower ratios generally mean more individualized feedback during rotations.
- Dedicated clinical coordinators: Programs that employ staff whose only job is managing clinical placements are better equipped to troubleshoot problems and build site partnerships over time.
- Established site partnerships: Ask how many unique rotation settings students have accessed in the last two years. Breadth matters because pediatric patients present very differently across primary care offices, specialty clinics, and hospital units.
- Average time to placement: Programs with strong coordinator infrastructure place students faster. Delays cost you time and can push back your graduation timeline.
Evaluating these factors alongside pass rate data gives you a much clearer picture of whether a program's clinical training will actually prepare you to practice confidently on day one.
What Pediatric NPs Earn After Training
The Bureau of Labor Statistics does not break out pediatric nurse practitioners as a separate category, so the figures below reflect the broader nurse practitioner occupation. Even so, they paint a compelling picture: NPs earn significantly more than registered nurses, and the profession is growing at roughly 40 percent over the 2024 to 2034 decade, ranking among the fastest growing occupations in the country. With more than 307,000 NPs employed nationally, demand remains strong across specialties. Graduates who complete rigorous pediatric clinical training position themselves competitively in this expanding market, because employers consistently value hands on experience when hiring for pediatric primary care and acute care roles.
| Occupation | Total National Employment | 25th Percentile Salary | Median Salary | 75th Percentile Salary | Mean Salary |
|---|---|---|---|---|---|
| Nurse Practitioners | 307,390 | $109,940 | $129,210 | $149,570 | $132,000 |
| Registered Nurses | 3,282,010 | $78,610 | $93,600 | $107,960 | $98,430 |
Common Questions About PNP Clinical Training
Clinical training is one of the most important parts of any pediatric nurse practitioner program, and it naturally raises a lot of questions. Below are answers to the concerns we hear most often from working nurses exploring PNP education.
- How many clinical hours are required for a pediatric nurse practitioner program?
- Most accredited PNP programs require a minimum of 500 direct patient care clinical hours, though many programs set the bar at 600 to over 700 hours depending on certification track and state requirements. Acute care tracks sometimes require additional hours in specialty settings. Check with your target program and state board for exact requirements, and see the clinical hours section earlier in this guide for a fuller breakdown.
- Do pediatric NP programs arrange clinical placements or do students find their own?
- It varies by program. Some schools coordinate placements through established partnerships with pediatric clinics and hospitals, while others expect students to identify and secure their own preceptors. Many programs take a hybrid approach, providing placement support and a preceptor database but asking students to finalize arrangements. Our earlier section on finding preceptors covers strategies for both scenarios.
- What is the difference between primary care and acute care PNP clinical rotations?
- Primary care PNP rotations focus on well-child visits, developmental screenings, chronic disease management, and community health settings such as outpatient pediatric offices. Acute care rotations center on critically or acutely ill children in environments like pediatric emergency departments, intensive care units, and inpatient hospital floors. The comparison section earlier in this article breaks down the key differences in scope, settings, and career paths.
- What pediatric nursing experience do you need before starting a PNP program?
- Admission requirements differ across schools, but most programs require an active RN license and a BSN. Some prefer or require one to two years of clinical nursing experience, ideally in a pediatric or family care setting. That said, several programs accept applicants with general nursing backgrounds and build pediatric competencies through coursework and clinical rotations. Direct pediatric bedside experience can give you a head start in clinical placements.
- How do simulation labs supplement clinical training in pediatric NP programs?
- Simulation labs let you practice high-stakes scenarios, such as pediatric resuscitation or managing a deteriorating patient, in a controlled environment before encountering them in real clinical settings. Many programs use high-fidelity pediatric mannequins, virtual patient encounters, and standardized patient actors. While simulation hours typically cannot replace all direct patient care hours, they reinforce clinical decision-making and build confidence. See our simulation section above for more detail.
- Can I complete PNP clinical rotations in my local area if I'm in an online program?
- In most cases, yes. Online PNP programs are designed so students can arrange clinical placements near where they live and work. Programs often maintain networks of approved clinical sites across multiple states. You will need to confirm that your chosen site and preceptor meet your program's requirements, and some states may have specific regulations. Starting the placement process early gives you the best selection of local sites.