Most important takeaways…
- Start your certification exam prep before graduation because licensure timelines often delay practice by two to four months.
- New NP salaries typically begin near the 25th percentile nationally and rise toward the median within the first few years.
- Expect to spend one to two extra hours daily on documentation during your first six months, the top driver of early burnout.
- A quarter-by-quarter ramp-up plan, negotiated during onboarding, protects you from unrealistic patient load expectations in year one.
Finishing NP school feels like crossing a finish line, but walking into your first exam room as a provider is an entirely new starting line. The transition from RN to nurse practitioner is one of the sharpest professional pivots in healthcare, and few new graduates grasp its intensity until they are in it. State-by-state credentialing timelines alone can stretch from three to nine months, leaving many new NPs stranded in paperwork during the very months they expected to be earning. The steepest challenges, including imposter syndrome, unrealistic patient loads, and documentation creep, tend to hit within the first six weeks of practice. Data from recent employer surveys indicate that nearly half of new NPs require more than a year to reach full clinical productivity, a reality that contract negotiations rarely address. This guide covers the lessons I wish someone had handed me on day one: from board certification and contract negotiation to patient load benchmarks, imposter syndrome, and the workflow habits that keep you sane past month six.
Board Certification and Licensure: What to Prepare For
The path from graduation to your first patient visit involves a maze of exams, applications, and waiting periods that often surprise new nurse practitioners.
Choosing Your Certification Exam: AANP vs. ANCC
Two national bodies certify NPs: the American Association of Nurse Practitioners Certification Board (AANP) and the American Nurses Credentialing Center (ANCC). The AANP exams focus heavily on clinical diagnosis, treatment, and pharmacology, while ANCC exams also incorporate professional issues, research, and nursing theory. First-time pass rates are comparable, though there are slight differences. In 2025, the AANP FNP exam had an 81% first-time pass rate, while the 2024 ANCC FNP-BC exam sat at 83%.12 For psychiatric-mental health, both saw 82-83%. Adult-gerontology primary care pass rates were 85% across both boards. Most employers accept either certification, so your choice should hinge on test style: the AANP exam uses all multiple-choice questions, whereas the ANCC includes alternative item types like hot spots and multiple-response questions. Plan to dedicate 8 to 10 weeks of full-time study (220-300 hours) or 10 to 14 weeks part-time (250-340 hours). If a retake is necessary, aim for at least 180 hours of focused prep. Our comprehensive nurse practitioner licensing guide walks through each certification pathway in more detail.
The Licensure and Credentialing Timeline
Once you pass your board exam, a flurry of applications begins. State licensure can take anywhere from a few weeks to a couple of months depending on your board of nursing. While you wait, apply for your National Provider Identifier (NPI), which is free and issued quickly. If you plan to prescribe controlled substances, secure a DEA number, which typically takes 4 to 6 weeks. The longest stretch, however, is credentialing with insurers and health systems. Credentialing alone often consumes 3 to 6 months as payers verify your education, licensure, and professional history. Some employers initiate this process on your behalf, but delays are common. Starting early, even before graduation if allowed, can prevent months of sitting idle.
Bridging the Gap Period
That gap between passing boards and seeing patients can feel like an eternity, but it is valuable prep time. Use it to orient yourself to your new practice setting, study for a subspecialty certification (such as diabetes management or suturing), or complete continuing education hours that will count toward your recertification. Many new NPs also explore residency or fellowship programs, which provide a supported transition. If your state allows practice under a provisional or graduate license, you might work in a limited capacity while credentialing finalizes. At minimum, network with colleagues, shadow experienced NPs in your specialty, and fine-tune your workflow. Treat this window as an extended onboarding rather than a forced vacation.
Compact Licensure and Job Mobility
As of 2026, more than 35 states have enacted the Advanced Practice Registered Nurse Compact (APRN Compact), allowing NPs to hold one multistate license and practice across participating state lines. This is a significant shift for new NPs, as it removes the need to apply for multiple separate licenses when moving or working in telehealth roles. Check whether your state has joined the compact; if so, you can apply for a compact license through your board. Even if you are not relocating immediately, a compact license future-proofs your career and opens opportunities in border regions or multistate health systems. For those in non-compact states, plan for extra licensing time and expense if you ever decide to relocate.
Navigating the Job Hunt and Negotiating Your First Contract
Your first NP contract is a legal document that will shape your day-to-day life, your earning potential, and sometimes your ability to change jobs for years afterward. Reading it carefully, ideally with an attorney who specializes in healthcare contracts, is one of the highest-return investments a new NP can make. For a deeper walkthrough of the entire process, see our guide to nurse practitioner contract negotiation.
Know What Competitive Pay Looks Like
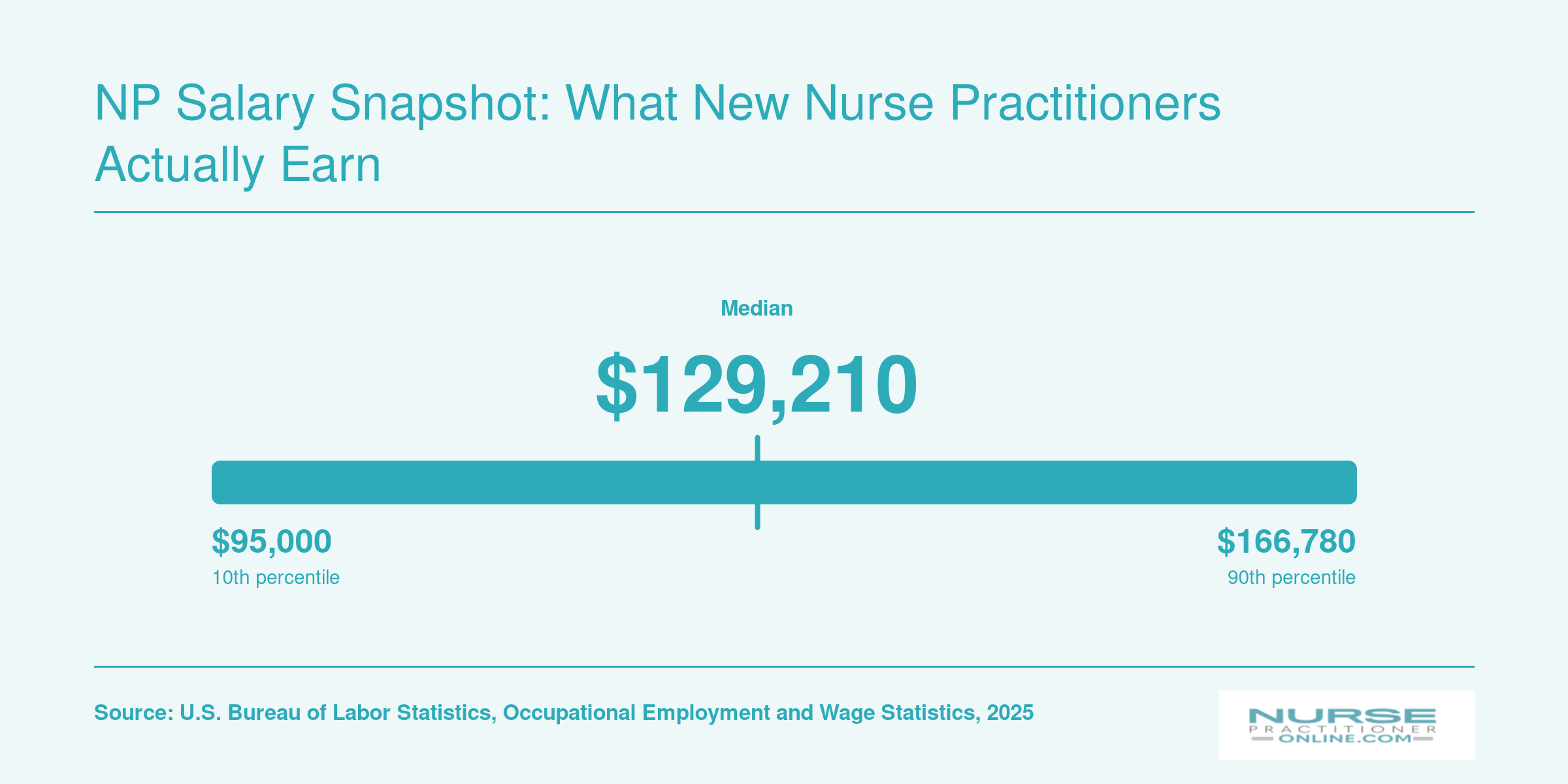
According to the most recent Bureau of Labor Statistics data, the national median annual salary for nurse practitioners is $129,210. The middle range runs from roughly $109,940 at the 25th percentile to $149,570 at the 75th percentile, with a national mean of $132,000. Those numbers give you a real anchor point. If an offer falls well below $110,000 without a compelling reason, that is worth pushing back on. If it clears $130,000, you are in solid territory, though local cost of living and specialty still matter. You can explore how compensation varies across roles in our breakdown of highest paid nurse practitioner specialties.
The Six Contract Clauses Most New NPs Miss
- Non-compete: Watch for clauses that restrict you from practicing any NP work in a radius of 25 to 50 miles for one to two years after leaving.1 That is the range most commonly flagged as aggressive. A clause that bars you from all NP practice in a region, rather than just similar roles, is a significant red flag.2
- Tail coverage: If the employer carries claims-made malpractice insurance, ask who pays for tail coverage when you leave. Tail can cost one to two times your annual premium.2 Get the answer in writing before you sign.
- Productivity bonuses and RVU thresholds: Understand what the target is and whether it is realistic for a clinician in their first year. Ask to see what current NPs in the role actually earn in bonuses, not just what is theoretically possible.
- CME allowance: Community practice settings typically offer $1,000 to $2,000 per year for continuing education; hospital systems tend to run $2,000 to $3,500, plus three to five days of paid CME time.3 If the offer is lower, that is a negotiating point.
- Termination clause: A without-cause notice period of 30 days is standard. A clause requiring 90 days notice from you before resigning is a red flag worth flagging.2 Contract terms of three years also deserve scrutiny, since that locks you in longer than the typical one-to-three-year range.
- Sign-on bonus repayment: A clawback requiring full repayment if you leave within a certain window is common, but 100 percent repayment regardless of how much time you have worked is worth negotiating down.2
Non-Compete Clauses and the Current Legal Landscape
Non-compete enforceability has been under federal scrutiny, and rules in this space are still shifting as of 2026. Even so, do not assume a non-compete is unenforceable in your state. Enforceability varies widely by jurisdiction. The practical move is to negotiate the radius down and the duration down before you sign, rather than hoping to challenge it later.
A straightforward counter sounds like this: "I want to work here long-term, and I understand the need for some protection. I would feel comfortable with a 10-mile radius and a one-year term rather than 25 miles and two years. Can we revise the language to reflect that?"
Negotiation Scripts That Actually Work
For a higher base: "Based on BLS data and offers I have reviewed, the median for this specialty and region is closer to [X]. I would like to ask that we start at [X plus 5 to 10 percent]. I am confident I will meet productivity expectations once I have completed orientation."
For a structured orientation period: "I would like to request that a defined orientation period of at least 90 days be written into the agreement, with a reduced patient panel and access to a supervising or collaborating physician during that window. Can we add that language?"
Asking for things in writing protects both sides. Employers who are confident in their offer will not object to putting orientation terms on paper.
NP Salary Snapshot: What New Nurse Practitioners Actually Earn
New nurse practitioners typically start closer to the 25th percentile of the national salary range and climb toward the median within their first few years of practice. Use these figures as a benchmark when evaluating job offers: if a proposed salary falls below $109,940, you have solid data to negotiate. Geographic region, specialty, and practice setting all influence where you land on this spectrum.
What to Expect: Realistic Patient Loads and Productivity Benchmarks
How many patients should a new nurse practitioner see per day in the first year? The honest answer: fewer than your collaborating physician, and fewer than you'll see by month twelve. Most employers build in a ramp-up period, but the specifics vary dramatically by setting. Knowing the benchmarks helps you push back when a schedule feels unsafe or unsustainable.
Primary Care: The Slow Build to a Full Panel
In primary care, new NPs typically start at 8 to 16 patients per day and grow toward a full schedule of 15 to 20 visits per day over 6 to 12 months.1 A mature panel size hovers around 800 patients, though scoping reviews from McMaster University show wide variation based on patient complexity and team support.1 If your offer letter expects 18 visits per day in month two, that's a red flag, not a goal.
Urgent Care: Faster Pace, Faster Ramp
Urgent care moves quickly. New NPs commonly see 18 to 26 patients across a 12-hour shift, with full productivity around 20 to 28 patients per 8-hour shift, or roughly 3 patients per hour.2 The ramp-up is still 6 to 12 months, but the learning curve is steep because acuity and chief complaints shift constantly. Expect heavy support from protocols and standing orders early on.
Specialty Clinics and Inpatient: Complexity Slows the Curve
Specialty outpatient settings (cardiology, endocrinology, oncology) typically start new NPs at 6 to 14 patients per day, building to 10 to 16 visits over 12 to 18 months.3 Productivity is often measured in work RVUs, with annual targets in the 3,000 to 4,500 range once you're established.3 Inpatient and hospitalist roles look similar: a daily census of 6 to 14 patients early on, climbing toward 10 to 16 within the first year. If unsustainable workloads go unchecked, they can contribute to nurse practitioner burnout, so tracking these numbers matters for your well-being as much as your performance reviews.
What to Ask Before You Sign
During contract negotiations, ask three specific questions: What is the expected patient volume in months 1, 3, 6, and 12? How are RVU or panel benchmarks calculated? Is there a productivity bonus, and when does it activate? Employers who can answer these clearly are usually the ones who actually honor a ramp-up. The AANP and published APP benchmarking surveys both reinforce that protected onboarding time correlates with retention, so it's a fair ask, not a favor.43
Questions to Ask Yourself
Managing Imposter Syndrome and the RN-To-NP Role Transition
Feeling like a seasoned expert at the bedside versus feeling like a novice all over again in a provider role: that contrast defines the RN-to-NP transition for most new nurse practitioners, and it catches people off guard. You spent years building clinical instincts as a registered nurse, yet the moment you start writing orders and making diagnostic decisions, a nagging voice insists you are not qualified. That voice has a name, and understanding it is the first step toward silencing it.
Why Imposter Syndrome Hits New NPs So Hard
Research consistently shows that imposter syndrome is widespread among new nurse practitioners, with published prevalence estimates suggesting a majority of early-career NPs experience it to some degree during their first one to two years of practice. The phenomenon is not a character flaw. It is a predictable byproduct of shifting from a collaborative, task-oriented RN scope to an autonomous, decision-driven provider scope. If you want to dig into the evidence yourself, search PubMed or CINAHL using terms like "imposter syndrome nurse practitioner transition." Seeing the data can be surprisingly reassuring because it confirms you are in good company.
Organizations like the American Association of Nurse Practitioners (AANP) and the National Organization of Nurse Practitioner Faculties (NONPF) have published white papers and survey findings that frame imposter syndrome as a transition-to-practice challenge rather than a personal shortcoming. Reviewing those resources on the AANP and NONPF websites can give you language to describe what you are experiencing and strategies backed by professional consensus.
Practical Strategies That Actually Help
Coping is not about "just believing in yourself." It is about building external scaffolding while your internal confidence catches up.
- Seek structured mentorship: Formal mentorship programs, whether through your employer, a state NP association, or an online NP community, pair you with an experienced provider who normalizes the learning curve. Ask questions early and often.
- Tap your alumni network: Many NP programs maintain alumni groups and career centers that offer peer-based advice, local transition data, and even informal case-review circles. These connections are goldmines for honest conversation about what the first year really feels like.
- Join online NP communities: Forums, social media groups, and professional platforms host thousands of NPs sharing real-world coping strategies. Hearing someone describe your exact struggle in a post from last Tuesday can dissolve the isolation imposter syndrome feeds on.
- Keep a "wins" journal: At the end of each shift, jot down one clinical decision you made well. Over weeks, the evidence accumulates and counters the internal narrative that you do not belong.
- Set realistic benchmarks: Compare yourself to where you were last month, not to a colleague who has been practicing for a decade. Growth is measurable if you choose the right yardstick.
Reframing the Transition
The discomfort you feel is not evidence that you chose the wrong career path. It is evidence that you are growing into a broader scope of practice, and there are many nurse practitioner advancement opportunities worth exploring once your confidence solidifies. Most experienced NPs will tell you that somewhere between month six and month eighteen, the anxiety fades and pattern recognition kicks in. Until then, lean on evidence, lean on mentors, and remind yourself that every provider you admire once sat exactly where you are sitting now.
Time Management and Clinical Workflow Tips for New NPs
Time management in clinical practice means structuring every patient visit, from chart review through documentation, so you finish your work within scheduled clinic hours rather than staying late every night. New nurse practitioners often underestimate how much longer each step takes when you are still building clinical confidence and learning systems.
Building a Realistic Visit Structure
A typical primary care visit has three phases: pre-visit chart review, the patient encounter, and documentation. During your first six months, plan for roughly two minutes of chart review before each patient, fifteen to twenty minutes for the encounter itself, and another ten to fifteen minutes for charting. This structure exceeds standard scheduling templates, which is why you should negotiate reduced patient loads or longer appointment slots during your ramp-up period. If your clinic schedules fifteen-minute visits, ask whether you can start with twenty or twenty-five minute slots and gradually decrease as your efficiency improves. Most practices expect new providers to reach full productivity between six and twelve months.
EHR Efficiency Tactics That Save Hours
Your electronic health record can either drain your time or dramatically accelerate documentation. These strategies help new NPs avoid the charting trap:
- Dot phrases or smart phrases: Build text shortcuts for your most common assessments and plans. A single period followed by a keyword can insert entire paragraphs of documentation.
- Template customization: Modify default visit templates to match your specialty's typical presentations so you are not deleting irrelevant sections every time.
- Voice-to-text dictation: Many EHR systems support Dragon or built-in speech recognition. Dictating notes during or immediately after the encounter can cut documentation time by half.
- Pre-built order sets: Create order bundles for conditions you see repeatedly, such as hypertension follow-up or well-child visits, so you are not clicking through dozens of individual orders.
- Favorite lists: Populate your medication and lab favorites early. Searching the full database for common prescriptions wastes valuable seconds that compound across a full clinic day.
Delegating Effectively to Support Staff
Medical assistants handle tasks that do not require your clinical judgment, but you need to communicate expectations clearly. Before your first day seeing patients, meet with your MA to establish workflows. Appropriate delegation includes rooming patients and obtaining vitals, administering screening questionnaires like PHQ-9 or fall risk assessments, completing medication reconciliation before you enter the room, and preparing routine order requisitions based on visit type. When support staff complete these tasks consistently, you walk into each encounter with updated information and can focus entirely on clinical decision-making. If you want to formalize these improvements, exploring nurse practitioner workflow improvement strategies can help you measure and sustain gains over time.
Escaping the After-Hours Documentation Trap
Spending two hours after clinic finishing charts is unsustainable and contributes to burnout. The most effective strategy is same-day completion, meaning you close every note before leaving the building. To make this work, document in real time by typing or dictating key findings while the patient is still in the room. Use the last two minutes of each appointment to finalize your assessment and plan rather than saving it for later. If you fall behind, use any cancellation or no-show slots to catch up immediately rather than checking email. Some new NPs block fifteen minutes at the end of each half-day session specifically for completing documentation. This approach treats charting as protected clinical time rather than an afterthought. Accurate, timely documentation also matters for primary care billing and coding, since incomplete notes can lead to denied claims and lost revenue.
Building Your Support System: Mentorship, Collaboration, and Resources
Some employers assign a formal mentor; others leave you to find your own guide entirely on your own. That distinction defines how your first year as a new NP unfolds. Proactively constructing a support system is not a sign of weakness. It is the most strategic investment you can make in your clinical confidence and career longevity.
Finding a Mentor When Your Employer Doesn't Assign One
If your practice does not pair you with a mentor, start by leveraging NP professional organizations. The American Association of Nurse Practitioners (AANP) and most state NP associations maintain directories or host events where experienced members are eager to connect. Specialty-specific online communities, like NP Facebook groups or forums, are also rich with clinicians who remember exactly how hard the transition felt. Nurse practitioner networking strategies can help you identify the right connections faster. And do not overlook the physicians you work alongside. Many are willing to offer informal guidance if you simply ask. A direct conversation with a collaborating physician often leads to the most natural and effective mentorship.
Structuring the Mentorship for Maximum Growth
Effective mentorship thrives on structure, not just sentiment. Aim for weekly thirty-minute check-ins during your first three months, then shift to monthly sessions as you gain footing. Bring something concrete to each meeting: a specific patient case, a differential you are wrestling with, or a workflow bottleneck. Vague anxiety can overwhelm the conversation, while targeted clinical questions create a productive learning loop. Structured transition-to-practice programs typically span six to twelve months, but mentorships can productively extend to twelve to twenty-four months as you tackle complex specialties and independent decision-making.12
Clinical Resources Every New NP Should Have on Day One
Your phone and office should be armed with these categories of tools before you see your first patient. For a deeper look at the best options, check out our guide to best apps for nurse practitioners.
- Point-of-care references: UpToDate or DynaMed give you rapid, evidence-based answers at the bedside.
- Prescribing support: Epocrates provides dosing, interactions, and safety checks in seconds.
- Clinical guidelines apps: The CDC Vaccine Schedules app, USPSTF screening tools, and specialty society pocket guides keep standards within reach.
- Peer consultation networks: Build a group chat with NP colleagues from your program or join a local NP consortium. When you need a second opinion fast, these connections are invaluable.
Collaborating with Physicians: A Clinical Asset, Not a Burden
Frame your collaborative relationship with physicians as an ongoing educational resource. Most physicians welcome the opportunity to share knowledge with an engaged NP. Use their experience as a safety net while you sharpen your clinical judgment. Competency-based orientation frameworks, like those mapped to NONPF core competencies, emphasize that new NPs grow through supported practice, not isolation.34 When you approach collaboration with curiosity and respect, you turn a regulatory requirement into the most powerful learning tool in your first year.
Common Mistakes New NPs Make (And How to Avoid Them)
What mistakes do new nurse practitioners make most often, according to disciplinary boards and peer-reviewed studies? The American Association of Nurse Practitioners (AANP) and state boards of nursing publish disciplinary reports that reveal recurring patterns: scope-of-practice violations, documentation gaps, and prescribing errors top the list. Understanding these pitfalls before you encounter them can save your license and your patients.
Diagnostic Errors: Anchoring and Premature Closure
New NPs often lock onto an initial diagnosis too quickly, a cognitive trap called anchoring bias. Systematic reviews show that novice providers close their differential too early, missing red flags or alternative explanations. The fix: force yourself to generate at least three plausible diagnoses for every chief complaint during your first year. Write them down. Ask yourself what findings would rule each one in or out, then look for those findings. Experienced preceptors emphasize this discipline, and many AANP continuing education modules teach structured decision-making frameworks that counter bias.
Over-Ordering Tests and Imaging
Anxiety drives new NPs to order more labs and imaging than necessary, inflating costs and sometimes triggering cascades of false positives. Peer-reviewed studies on diagnostic stewardship recommend evidence-based algorithms, such as Ottawa Ankle Rules or Choosing Wisely guidelines. Before you order a test, ask: Will this result change my management? If not, skip it. Mentors can help you calibrate clinical judgment faster than any textbook. Using nurse practitioner tools like clinical decision support apps can also keep you aligned with current evidence at the point of care.
Documentation Gaps That Invite Legal Risk
State board reviews frequently cite incomplete or inconsistent documentation. Common errors include failing to document informed consent for procedures, omitting your clinical reasoning for prescription changes, or neglecting to note follow-up plans for abnormal results. Chart as if you are explaining your thinking to a peer reviewer, because someday you might be. Many malpractice carriers offer free documentation audits for new providers.
Prescribing Errors and Scope Violations
New NPs sometimes prescribe outside their state's formulary restrictions or fail to check drug interactions and renal dosing. Studies quantifying these mistakes point to clear prevention strategies: double-check every unfamiliar medication in a clinical decision support tool, verify state scope rules before signing a prescription for a controlled substance, and never assume your supervising physician's scope equals yours. If you plan to serve as a primary care nurse practitioner, understanding your prescriptive authority inside and out is essential from day one.
Failure to Follow Up on Results
Ordering a test creates a legal duty to follow up. Set calendar reminders, use your EHR's task manager, and build a system for tracking pending labs and imaging. Studies show that result-tracking failures are a leading cause of malpractice claims among all advanced practice providers.
Consult experienced NPs in your specialty, review free Medscape modules on reducing diagnostic bias, and treat every near-miss as a learning opportunity. Your first year is when habits form, good or bad.
Related Articles
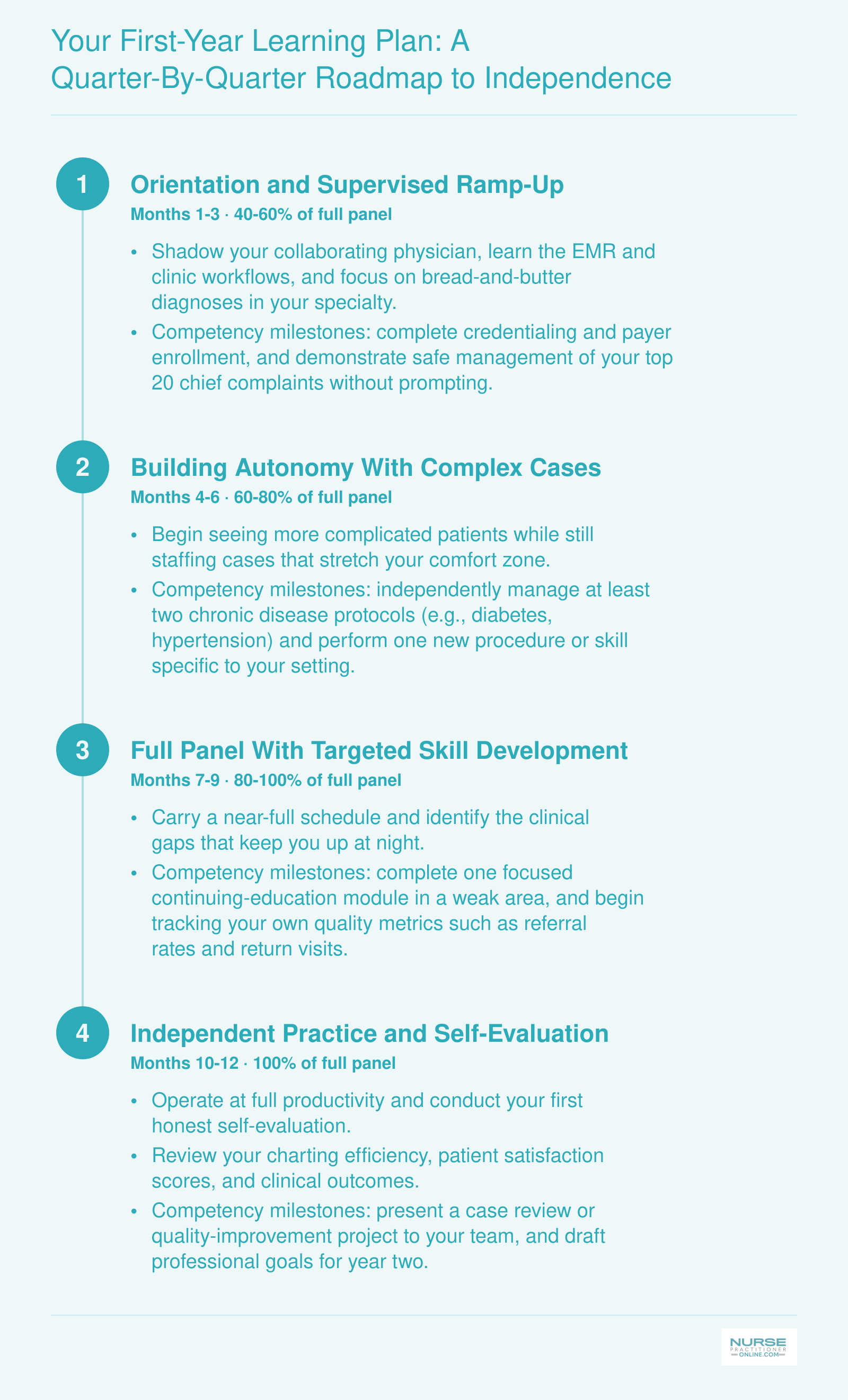
Your First-Year Learning Plan: A Quarter-By-Quarter Roadmap to Independence
This roadmap is not just a personal aspiration. It is a framework you can bring to your employer during onboarding or contract negotiation. Many new NPs never discuss productivity ramp-up expectations, then feel blindsided when they are expected to carry a full panel by month two. Print this out, share it with your collaborating physician or supervisor, and use it to set realistic, measurable goals together.
Frequently Asked Questions About Starting as a New NP
Starting your first year as a nurse practitioner raises a lot of questions, and most of them do not have simple answers. Below are the questions new NPs ask most often, with practical guidance drawn from the topics covered throughout this article.
- How hard is it to be a nurse practitioner in your first year?
- The first year is genuinely challenging. You are adjusting to autonomous decision-making, learning new documentation workflows, and building confidence in a role that feels very different from bedside nursing. Most new NPs say the steepest learning curve lasts about six to twelve months. The sections on managing imposter syndrome and realistic productivity benchmarks above offer strategies to help you navigate this transition with less stress.
- What is a realistic patient load for a new nurse practitioner?
- Most practices ramp new NPs up gradually, starting around 8 to 12 patients per day in the first few months and increasing toward 18 to 22 over the first year, depending on specialty and visit complexity. Jumping to a full panel too quickly leads to burnout and clinical errors. See the section on realistic patient loads and productivity benchmarks for more detail on what to expect.
- How long should a new NP orientation be?
- A thorough orientation typically runs 90 days at minimum, though many experienced NPs recommend at least six months of structured support. During that time you should have access to a collaborating provider for questions, a reduced patient schedule, and regular feedback sessions. If a job offer includes little or no orientation, treat that as a red flag during your contract negotiation.
- How do I handle imposter syndrome as a new NP?
- Imposter syndrome is nearly universal among new nurse practitioners. Acknowledging it is the first step. Build a peer support network, seek out a mentor who remembers their own transition, and keep a log of clinical wins to review on tough days. The section on managing imposter syndrome and the RN to NP role transition covers specific techniques for reframing self-doubt into professional growth.
- What do I wish I knew as a new nurse practitioner?
- The most common answers include: negotiate your first contract carefully, ask for a longer orientation, invest in a solid mentorship relationship early, and accept that discomfort is a normal part of growth. Many NPs also wish they had understood the real cost of staying late to chart and had built better time management habits from day one. The quarter by quarter learning plan in this article maps out priorities for your entire first year.
- What mistakes do new nurse practitioners commonly make?
- Common missteps include accepting the first job offer without negotiating, skipping a structured orientation, trying to see a full patient panel too soon, and isolating yourself instead of seeking mentorship. Some new NPs also over-order tests out of anxiety or under-document clinical reasoning. The section on common mistakes new NPs make breaks these down with specific strategies to avoid each one.
Every new nurse practitioner struggles in the first year, and that struggle is not a sign of incompetence. It is the universal cost of transitioning from expert RN to novice provider. The NPs who thrive are the ones who stop white-knuckling through it and start building systems early: a mentor who answers your 9 p.m. text, EHR templates that shave minutes off every note, a quarter-by-quarter learning plan that turns vague anxiety into measurable progress.
Pick one action from this article and do it this week. Negotiate one contract clause before you sign. Build one documentation template tonight. Send one email to a potential mentor. A single step, taken now, changes the trajectory of your entire first year.