Most important takeaways…
- NPs earn a slightly higher median salary than CNMs nationally, though California leads compensation for both roles.
- Projected job growth for nurse practitioners reaches 40% from 2024 to 2034, far exceeding most occupations.
- Only certified nurse-midwives hold clinical privileges to manage labor and deliver babies independently.
- Scope of practice and prescriptive authority for both roles vary significantly by state, affecting day-to-day autonomy.
A projected 40% job growth rate for nurse practitioners places this profession among the fastest-growing in the U.S. economy, yet certified nurse-midwives serve a radically different patient population, focusing on pregnancy, birth, and women's health across the lifespan. Both are advanced practice registered nurses (APRNs) who complete graduate-level education, but a CNM is not simply a type of NP; the two hold distinct national certifications and scopes of practice. The choice often turns on a single question: do you want to attend births as part of your clinical role? The answer directs you toward different degree programs, certification exams, and salary trajectories. This guide walks through each dimension side by side so you can make a confident decision.
NP Vs. CNM at a Glance: Quick Comparison Table
Before diving into the details, a side-by-side snapshot can save you a lot of time. The table below captures the most practical differences between nurse practitioners and certified nurse-midwives so you can orient yourself before exploring each path in depth.
Credential and Education
Both roles require an advanced nursing degree, but the typical entry points differ slightly. NPs can enter practice with either a Master of Science in Nursing or a Doctor of Nursing Practice, and the degree level does not by itself determine scope of practice.1 State law governs that. CNMs most commonly hold an MSN or equivalent graduate degree, and at that level the full scope of midwifery practice is available to them.
Programs for each credential are accredited by separate bodies. NP programs fall under the Commission on Collegiate Nursing Education (CCNE) or the Accreditation Commission for Education in Nursing (ACEN). Midwifery programs are accredited by the Accreditation Commission for Midwifery Education (ACME), which sets its own distinct standards. If you are considering the doctoral route, it helps to understand DNP prerequisites before you apply.
Certification and Licensure
After graduation, NPs sit for exams offered through the American Nurses Credentialing Center (ANCC), the American Association of Nurse Practitioners (AANP), or the National Certification Corporation (NCC), depending on their specialty.1 CNMs take the exam administered by the American Midwifery Certification Board (AMCB). Both credentials result in APRN licensure, just under different designations.
Scope and Settings
Here is where the two paths diverge most visibly:
- Clinical focus: NPs work across primary care and specialty areas. CNMs concentrate on maternal and reproductive health throughout the lifespan.
- Birth attendance: NPs do not typically attend births. Attending births is a defining feature of CNM practice.
- Prescriptive authority: Both NPs and CNMs hold prescriptive authority in all states, though the specific rules vary by state.
- Work settings: NPs practice in clinics, hospitals, telehealth platforms, and specialty offices. CNMs are most commonly found in hospitals, birth centers, and maternity-focused outpatient settings.
- Full practice authority: Roughly 25 states plus Washington, D.C., grant both NPs and CNMs the ability to practice independently without required physician oversight, though the specific rules and any transition-to-practice requirements differ by state and credential type.
Think of this table as a compass, not a complete map. The sections that follow give each row the depth it deserves.
What Does a Nurse Practitioner Do?
What does a nurse practitioner actually do day to day, and how is the role different from a physician's? An NP is an advanced practice registered nurse (APRN) trained at the master's or doctoral level to diagnose conditions, order and interpret tests, prescribe medications, and manage care across the full spectrum of acute and chronic illness. The specifics of that work, though, depend heavily on which population focus you choose.
NP Is an Umbrella, Not a Single Job
When nurses say they want to "become an NP," they are really choosing among several population-focused tracks. Each one trains you for a different patient group:
- FNP (Family Nurse Practitioner): Primary care across the lifespan, from newborns to older adults.
- AGNP (Adult-Gerontology NP): Adults and aging patients, available in primary care or acute care concentrations.
- PMHNP (Psychiatric-Mental Health NP): Diagnosis and treatment of mental health and substance use conditions, including medication management and therapy.
- PNP (Pediatric NP): Care for infants, children, and adolescents.
- WHNP (Women's Health NP): Gynecologic, reproductive, and obstetric care for women across the lifespan.
- Neonatal NP: Critically ill newborns, often in NICUs.
You can explore these tracks in greater depth in our guide to nurse practitioner specialties.
Clinical Responsibilities
Across specialties, NPs perform physical exams, develop treatment plans, prescribe and adjust medications, order labs and imaging, manage chronic conditions like diabetes and hypertension, counsel patients on prevention, and refer to specialists when needed. In states with full practice authority, they do this independently. In reduced or restricted practice states, a collaborative agreement with a physician is required. Understanding the difference between acute care vs primary care tracks can help you decide where your clinical interests fit best.
Where NPs Work
NPs practice in primary care offices, hospitals, urgent care centers, specialty clinics (cardiology, oncology, dermatology), school-based health, correctional facilities, retail clinics, and telehealth platforms. An FNP in a rural clinic and a PMHNP delivering virtual psychiatric care have very different days, but both carry the same NP credential. That breadth is what makes the role flexible, and why "NP" alone never fully describes the work.
What Does a Certified Nurse-Midwife Do?
For many nurses weighing the NP versus CNM career path, the central question comes down to a single, defining privilege: Do you want to deliver babies? While nurse practitioners can specialize in women's health across the lifespan, only certified nurse-midwives are trained and licensed to independently manage labor and birth, a responsibility that shapes every aspect of their practice. Yet the CNM role extends far beyond the delivery room.
The CNM Scope: Beyond the Delivery Room
Certified nurse-midwives provide a full range of women's health services. Their care spans preconception counseling, prenatal visits, labor and delivery management, postpartum support for mother and infant, and newborn care in the first weeks of life. Throughout a woman's reproductive years, CNMs also perform annual gynecological exams, prescribe contraception, screen for and treat sexually transmitted infections, and diagnose reproductive health conditions. Beyond childbearing, they manage perimenopausal and postmenopausal care, offering hormone therapy guidance, bone density monitoring, and preventive health screenings. In essence, a CNM is a primary care provider for women, with a deep focus on the childbearing cycle.
Where CNMs Practice and Manage Births
A key differentiator is the setting. CNMs attend births in hospitals, freestanding birth centers, and private homes, depending on their practice arrangements and state regulations. In all of these environments, they function as independent providers of low-risk obstetric care. They assess fetal well-being, monitor labor progression, provide pain management (including regional anesthesia when collaborating with an anesthesiologist), manage spontaneous vaginal deliveries, perform episiotomies and repairs, and address emergency situations such as postpartum hemorrhage using the full scope of their training. When complications arise that exceed the low-risk criteria, CNMs consult with or transfer care to an obstetrician, making the collaborative relationship an important aspect of their work.
Yes, CNMs Deliver Babies: Here's What That Means
The question we hear most often is straightforward: Can a nurse midwife deliver babies? The answer is unequivocally yes. This is the defining clinical privilege that separates CNMs from other advanced practice registered nurses, including women's health nurse practitioners (WHNPs) and family nurse practitioners (FNPs). While WHNPs may provide comprehensive prenatal and postpartum care, they do not attend births in an intrapartum capacity. The hands-on responsibility of catching a newborn, managing the third stage of labor, and ensuring maternal stability during the immediate postpartum period is exclusively held by midwives and physicians. For nurses who feel called to be present at the miracle of birth and to support families through one of life's most transformative events, becoming a CNM offers a direct path to that role.
A Lifespan Focus That Surprises Many
It's a common misconception that CNMs only care for pregnant women. In reality, many CNMs continue to see patients for years after their last delivery, building lasting relationships that cover contraception choices, perimenopause symptom management, and routine preventive care. Schools and national certification standards emphasize that CNMs are prepared to offer primary care to women from adolescence through senior years. To explore what this role looks like in a broader context, consider how a nurse practitioner can be a primary care provider across settings. This broader lens means that a CNM career can be just as varied as that of a primary care NP, while still keeping birth at its core, offering a unique blend of continuity and high-acuity event-based care that few other roles provide.
CNM Vs. WHNP Vs. FNP: Clearing up the Three-Way Confusion
All three credentials are advanced practice registered nurse (APRN) roles, but they differ sharply in scope of practice, patient populations, and clinical privileges. Certified nurse-midwives (CNMs) are licensed to provide full-spectrum reproductive care including pregnancy management and intrapartum care (labor and delivery). Women's health nurse practitioners (WHNPs) focus on gynecologic and reproductive health across the lifespan but generally do not attend births. Family nurse practitioners (FNPs) provide primary care to patients of all ages and genders, with women's health as one component of a broader practice.
Can WHNPs Attend Births?
No uniform national rule exists. A handful of states permit WHNPs with specialized training to provide intrapartum care, but most do not. To determine whether WHNPs can attend births in your state, check your state Board of Nursing scope-of-practice documents and compare them with the NCSBN APRN Consensus Model guidelines. State-by-state verification is essential because scope authority varies widely, and understanding full practice authority states can help you navigate these differences.
Dual Certification: CNM and WHNP
Some clinicians pursue both CNM and WHNP credentials to maximize employment flexibility. For current trends, review annual certification statistics published by the American College of Nurse-Midwives (ACNM) and the National Certification Corporation (NCC), available on their websites. Top midwifery programs such as Frontier Nursing University and Georgetown offer pathways that prepare graduates for dual certification, though completing both exams requires additional clinical hours and study time.
Staying Current on Scope Changes
Scope-of-practice regulations evolve. Monitor ACNM position statements and legislative updates for CNM developments, and review NCC core competencies, which were revised in 2024 and 2025. The Bureau of Labor Statistics (BLS.gov) publishes occupational outlook updates that reflect workforce and regulatory shifts. Beyond formal sources, interview current CNMs and WHNPs through professional forums or LinkedIn to hear how scope differences play out in day-to-day practice. Formal data often lags behind real-world changes, so first-person accounts fill critical gaps.
Education and Certification Requirements Compared
MSN versus DNP, ANCC versus AANP, CCNE versus ACME: the choice between nurse practitioner and certified nurse-midwife training comes down to which accrediting bodies, certification exams, and clinical hour structures fit your goals. Both paths start from the same baseline (an active RN license and a BSN), but they diverge sharply once you enter graduate school.
Degree Pathways and Accreditation
NP programs are accredited by the Commission on Collegiate Nursing Education (CCNE) or the Accreditation Commission for Education in Nursing (ACEN). You can learn more about how ACEN vs CCNE accreditation affects your program choice. You can enter the workforce with a Master of Science in Nursing (MSN) or a Doctor of Nursing Practice (DNP), with the DNP increasingly offered as the terminal practice degree.
CNM programs follow a different track. They must be accredited by the Accreditation Commission for Midwifery Education (ACME) for graduates to sit for the certification exam. Like NP programs, CNM education is available at the MSN, post-master's certificate, or DNP level.
The accrediting body matters because eligibility for nurse practitioner licensing and certification depends on it. A nursing program without ACME accreditation will not qualify you for midwifery boards, no matter how strong the curriculum.
Certification Exams at a Glance
- AMCB (CNM): 175 multiple-choice questions, roughly $500, with a 2024 pass rate near 80%.1
- AANP (FNP): 150 single-answer multiple-choice questions, 180 minutes, about $315, with a 2024 pass rate around 83%.23
- ANCC (FNP): 175 questions in mixed formats (multiple-choice, multiple-response, drag-and-drop, hotspot), 210 minutes, roughly $395, with a 2024 pass rate around 83%.23
NP candidates choose between ANCC and AANP based on test style; CNMs have a single national exam through the American Midwifery Certification Board. For a deeper comparison of the two NP board exams, see our guide to the NP certification exam.
Clinical Hours and the DNP Question
NP programs typically require 500 to 750 direct patient care hours. CNM programs often require more, particularly in intrapartum care, because graduates must demonstrate competency managing labor and birth.
As of 2024, the DNP is not mandatory for CNM entry into practice.1 The AACN has long advocated the DNP as the preferred preparation for advanced practice nurses, and the ACNM accepts master's, post-master's certificate, and DNP pathways. Expect continued movement toward doctoral preparation, but a well-designed MSN remains a valid route into both careers today.
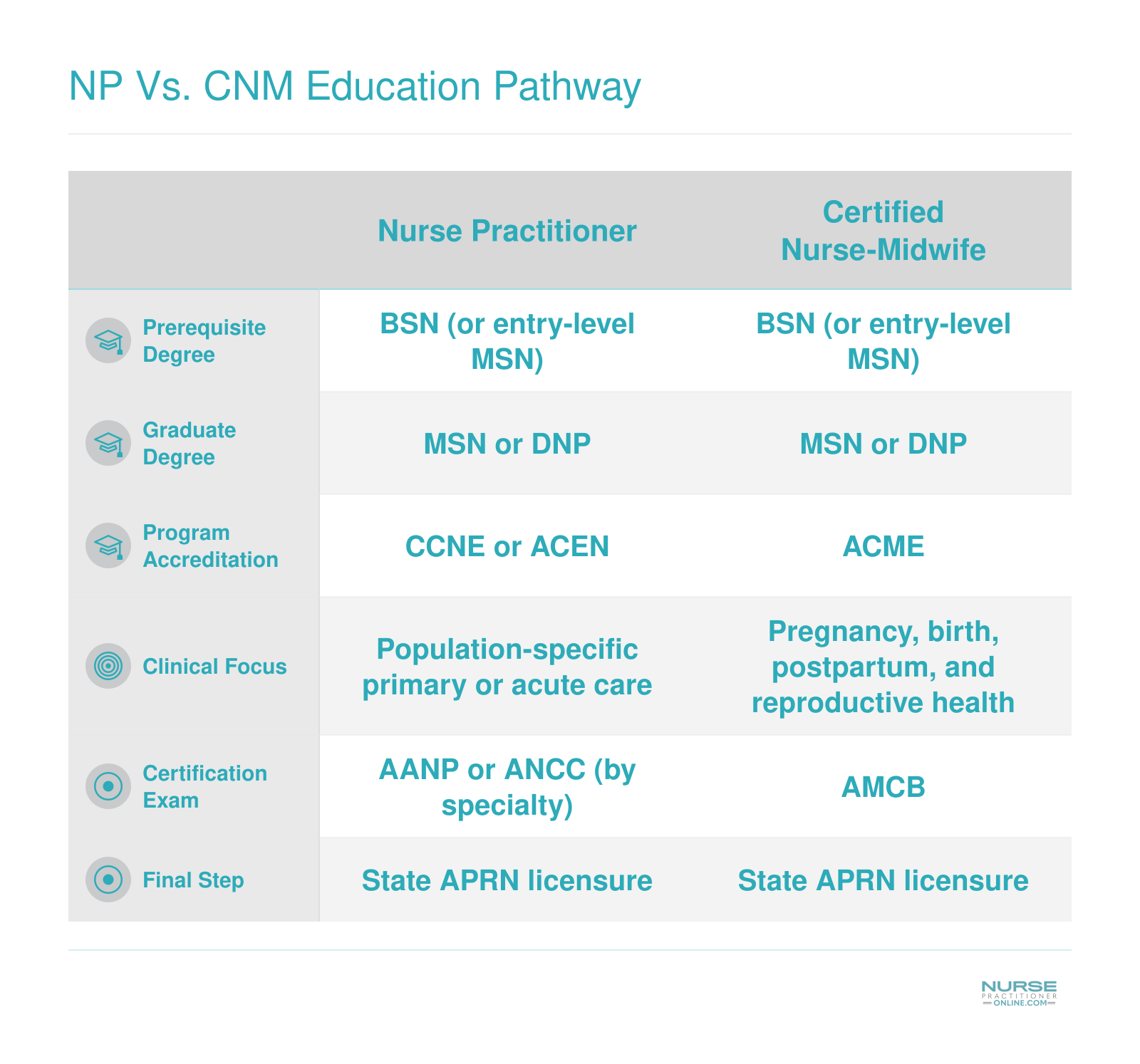
NP Vs. CNM Education Pathway
Both nurse practitioners and certified nurse-midwives follow a similar four-stage credentialing journey, starting with a BSN and ending with state licensure. The key differences emerge in program accreditation, clinical training focus, and the national certification exam each role requires.
Scope of Practice and Prescriptive Authority by State
What can a nurse practitioner or certified nurse-midwife do independently in your state, and can a nurse midwife prescribe medication?
These questions matter enormously because practice authority varies dramatically across the country. Where you work determines whether you can evaluate patients, diagnose conditions, and prescribe treatments without physician oversight, or whether you need a collaborative agreement to practice at all.
NP Practice Authority: Three Tiers Explained
The American Association of Nurse Practitioners categorizes state practice environments into three tiers based on how much autonomy NPs have:1
- Full practice: NPs can evaluate, diagnose, interpret tests, and manage treatments independently without physician collaboration. As of 2025, approximately 28 states (or 30 states and territories) grant full practice authority.2
- Reduced practice: NPs must maintain a collaborative agreement with a physician but can still practice in many settings. About 12 to 15 states fall into this category.2
- Restricted practice: NPs require physician supervision, delegation, or team management for at least one element of practice. Roughly 11 states maintain these restrictions.2
States like Arizona, Colorado, and Oregon exemplify full practice environments where NPs can open independent practices, prescribe controlled substances, and manage patient care autonomously. In contrast, Texas and California maintain more restrictive frameworks requiring various levels of physician involvement. For a deeper look at how these categories play out, see our NP scope of practice guide.
CNM Practice Authority: A Different Landscape
Certified nurse-midwives operate under their own set of state regulations, which do not always align with NP rules. Some states grant CNMs full independent practice, allowing them to manage pregnancies, attend births, and provide primary care to women without physician oversight. Other states require collaborative practice agreements or physician supervision, particularly for hospital-based deliveries.
The American College of Nurse-Midwives tracks these variations, and the patchwork can surprise nurses comparing career paths. A state granting NPs full practice authority may still require CNMs to have collaborative agreements, or vice versa. New Mexico, for example, has long supported midwifery autonomy, while some southeastern states impose stricter collaboration requirements on CNMs than on NPs.
Prescriptive Authority: Yes, Both Can Prescribe
To answer the common question directly: yes, certified nurse-midwives can prescribe medications in all 50 states, including controlled substances in most jurisdictions. Both NPs and CNMs hold prescriptive authority, though the specifics vary by state.
Most states permit both roles to prescribe Schedule II through V controlled substances, which means CNMs can manage pain during labor and prescribe postpartum medications as needed. A handful of states impose additional requirements, such as DEA registration protocols or collaborative agreement stipulations for controlled substance prescribing, but outright prohibition is rare.
The Trend Toward Expansion
Both AANP and ACNM actively advocate for full practice authority, arguing that removing unnecessary barriers improves healthcare access, particularly in rural and underserved areas. The legislative trend over the past decade has moved toward expansion for both roles, and this shift reflects the evolving role of nurse practitioners in the broader healthcare system. Several states have upgraded their practice environments in recent years, and more bills are pending.
If you are choosing between these paths, research your intended state of practice carefully. AANP maintains updated state issue maps tracking current regulations, and ACNM offers similar resources. These tools are essential for understanding what your daily practice will actually look like after graduation.
Salary Comparison: NP Vs. Nurse Midwife
Nurse practitioners and certified nurse midwives earn comparable salaries, though NPs hold a slight edge in median and mean pay. The figures below reflect the most recent national data from the Bureau of Labor Statistics. Both roles offer strong earning potential, and actual compensation can vary significantly based on specialty, geographic location, practice setting, and years of experience.
| Metric | Nurse Practitioners | Certified Nurse Midwives |
|---|---|---|
| Total National Employment | 307,390 | 8,280 |
| Mean Annual Salary | $132,000 | $128,110 |
| Median Annual Salary | $129,210 | $128,790 |
| 25th Percentile Salary | $109,940 | $104,260 |
| 75th Percentile Salary | $149,570 | $146,520 |
Highest-Paying States for NPs and CNMs
Geography plays a major role in APRN compensation. Below are the top-paying states for nurse practitioners and certified nurse midwives, ranked by median annual salary. California leads both lists by a wide margin, and several states appear in the top tier for both roles. Keep in mind that high-paying states often have a higher cost of living, so it is worth weighing salary against local expenses when planning a move or job search.
| State | NP Median Salary | CNM Median Salary |
|---|---|---|
| California | $166,610 | $196,700 |
| New Jersey | $149,620 | $135,680 |
| Alaska | $145,450 | $130,030 |
| New York | $145,390 | $137,860 |
| Massachusetts | $138,890 | $155,710 |
| Washington | $140,220 | $145,000 |
| Vermont | $129,740 | $140,240 |
| Iowa | $129,420 | $136,450 |
| New Hampshire | $132,440 | $135,860 |
| Arizona | $133,790 | $135,590 |
| Wisconsin | $128,580 | $135,360 |
| Minnesota | $128,570 | $127,180 |
| Rhode Island | $130,710 | $127,480 |
| Indiana | $128,280 | $129,010 |
| Colorado | $129,750 | $132,670 |
Job Outlook and Workforce Demand
A projected 40% job growth rate for nurse practitioners between 2024 and 2034 places this profession among the fastest-growing occupations in the entire U.S. economy, far outpacing the 3.1% average for all occupations and even the robust 8.4% growth expected across the healthcare sector as a whole.1 This translates to approximately 128,400 new NP positions over the decade, creating substantial opportunities for nurses pursuing this advanced practice pathway.2
NP Demand Drivers
Several converging factors fuel the exceptional demand for nurse practitioners:
- Primary care shortage: Physician shortages in primary care continue to expand NP hiring across clinics, hospitals, and health systems seeking to maintain patient access.
- Aging population: As baby boomers require more chronic disease management and preventive services, NPs fill critical gaps in geriatric and family care.
- State scope expansions: More states are granting full practice authority to NPs, allowing them to practice independently and increasing employer willingness to hire.
- Telehealth growth: Virtual care platforms have created entirely new practice settings where NPs deliver remote consultations and follow-up care.
CNM Demand Drivers
Certified nurse-midwives experience an 11% projected growth rate during the same period.2 While more modest than NP growth, this still significantly exceeds the national average. Demand drivers include:
- Midwifery workforce shortages: Many regions lack adequate midwifery providers, creating persistent openings in underserved communities.
- Maternal health deserts: Rural areas with limited or no obstetric services increasingly rely on CNMs to provide prenatal, birth, and postpartum care.
- Consumer preference: Growing interest in the midwifery model of care, which emphasizes physiologic birth and shared decision-making, expands demand in hospital and birth center settings alike.
- Medicaid expansion: In states that have expanded Medicaid, more birthing people gain coverage for midwifery services, increasing utilization and CNM hiring.
Workforce Size and Competition
The NP workforce is dramatically larger than the CNM workforce. Current employment data shows over 307,000 nurse practitioners working nationally compared to roughly 8,600 certified nurse-midwives.3 This size difference means NPs encounter far more job postings overall, but it also means more applicants competing for those positions. To learn more about where openings are concentrated, see our breakdown of which states need nurse practitioners the most. CNMs, by contrast, face less competition per opening in many markets, particularly in rural healthcare areas where employer need is high and qualified candidates are scarce. Both pathways offer strong employment prospects, though the competitive landscape differs significantly.
How to Decide: CNM or NP?
Choosing between certified nurse-midwife and nurse practitioner comes down to four practical dimensions: the patients you want to serve, your interest in birth attendance, your desired scope of practice, and the schedule you can sustain over the long haul.
Patient Population and Practice Focus
If you love working across the lifespan (pediatrics, adults, geriatrics) and want a broad primary-care role, nurse practitioner tracks offer that width. Family nurse practitioners manage hypertension in grandparents and strep throat in toddlers, and understanding the difference between FNP and AGNP can help you pick the right track. Certified nurse-midwives concentrate on women's reproductive health and newborn care. If attending births excites you, CNM is the clear path. If the idea of middle-of-the-night deliveries feels draining, an NP specialty will keep you in clinic-based or inpatient rotations with more predictable hours.
Autonomy, State by State
Neither role is categorically more autonomous. Full practice authority for both NPs and CNMs varies by state. In some jurisdictions, CNMs have broader prescriptive rights than certain NP specialties. In others, the reverse is true. Your independence will depend on your state's APRN statutes, your employer's protocols, and your specialty's regulatory landscape, not the letters after your name.
Career Pivots Are Expensive
Switching from NP to CNM later (or the reverse) is not a simple post-master's certificate. You will need to complete an entirely new graduate program, often 18 to 24 months and costing tens of thousands of dollars. Choose carefully on the front end.
Shadow Before You Commit
Before you submit your first application, spend a full shift shadowing both a CNM and an NP in the specialty that interests you. Watch the workflows, the patient interactions, the charting load, and the team dynamics. A single day of observation will answer questions no website can.
Frequently Asked Questions: NP Vs. CNM
Choosing between a nurse practitioner and a certified nurse midwife path raises plenty of practical questions. Below are concise, evidence-based answers to the ones working nurses ask most often.
- Is a CNM considered a nurse practitioner?
- Not exactly. Both CNMs and NPs are Advanced Practice Registered Nurses (APRNs), but they hold different certifications and operate under separate regulatory categories. CNMs are certified by the American Midwifery Certification Board, while NPs are certified through bodies such as the AANP or ANCC. Some states group them together for licensing purposes, yet their scopes of practice, educational focus, and clinical training differ significantly.
- Can a nurse midwife prescribe medication?
- Yes. CNMs hold prescriptive authority in all 50 states, though the specifics vary. In states with full practice authority, CNMs prescribe independently, including controlled substances. In reduced or restricted practice states, a collaborative agreement with a physician may be required. Before practicing, CNMs should verify their state board's current prescriptive authority rules, because legislation in this area continues to evolve.
- Can a nurse midwife deliver babies?
- Absolutely. Delivering babies is central to a CNM's role. Certified nurse midwives manage labor, perform deliveries, and provide postpartum care in hospitals, birth centers, and home settings. They handle normal, low-risk pregnancies independently and collaborate with obstetricians when complications arise. CNMs attend a notable share of vaginal births in the United States each year, making them essential members of the maternal health workforce.
- Do nurse midwives make more than nurse practitioners?
- In most cases, NPs earn slightly more on average. According to the Bureau of Labor Statistics, the median annual wage for nurse practitioners was approximately $126,260 as of the latest published data, while nurse midwives earned a median of around $120,880. However, compensation varies widely by state, specialty, practice setting, and experience level, so individual CNMs in high-demand regions can out-earn many NPs.
- Which has more autonomy, an NP or a CNM?
- It depends on the state. Both roles are governed by state practice authority laws, and roughly half of U.S. states now grant full practice authority to NPs and CNMs alike. In states with restricted frameworks, either role may need a physician collaboration agreement. CNMs sometimes enjoy broader autonomy within their specialty because midwifery-specific statutes can differ from general NP regulations. Always check your state's current APRN practice act for the most accurate comparison.
- Can you switch from NP to CNM without going back to school?
- Generally, you will need additional education. NP and CNM programs have distinct clinical competencies, and midwifery certification requires completion of an accredited nurse midwifery program. Some schools offer bridge or post-graduate certificate programs that let experienced NPs, especially Women's Health NPs, complete midwifery training in a shorter timeframe than a full master's or doctoral program. These bridge options can save time while meeting certification requirements.