Most important takeaways…
- CRNAs earn a median salary roughly $90,000 higher than NPs nationally, based on 2024 BLS data.
- CRNA programs now require a doctorate, adding one to two years beyond most NP program timelines.
- Higher CRNA tuition typically pays for itself within three to five years of practice.
- NP roles are projected to grow 40% through 2033, offering wider specialty and schedule flexibility.
Nurse practitioners and certified registered nurse anesthetists both hold graduate nursing degrees, both build on bedside RN experience, and both practice at the top of the nursing license. That is roughly where the similarities end. According to 2024 Bureau of Labor Statistics data, CRNAs earn a median of $223,210 a year compared with $129,210 for NPs, a spread of more than $90,000 that reflects sharply different training, scope, and work settings.
The tradeoff is real. CRNA programs now require a doctoral degree, run three to four years full-time, and accept a small fraction of applicants, while most NP tracks remain master's-level and far more accessible. The choice is less about prestige than about which clinical rhythm, debt load, and patient population fit a nurse's next twenty years.
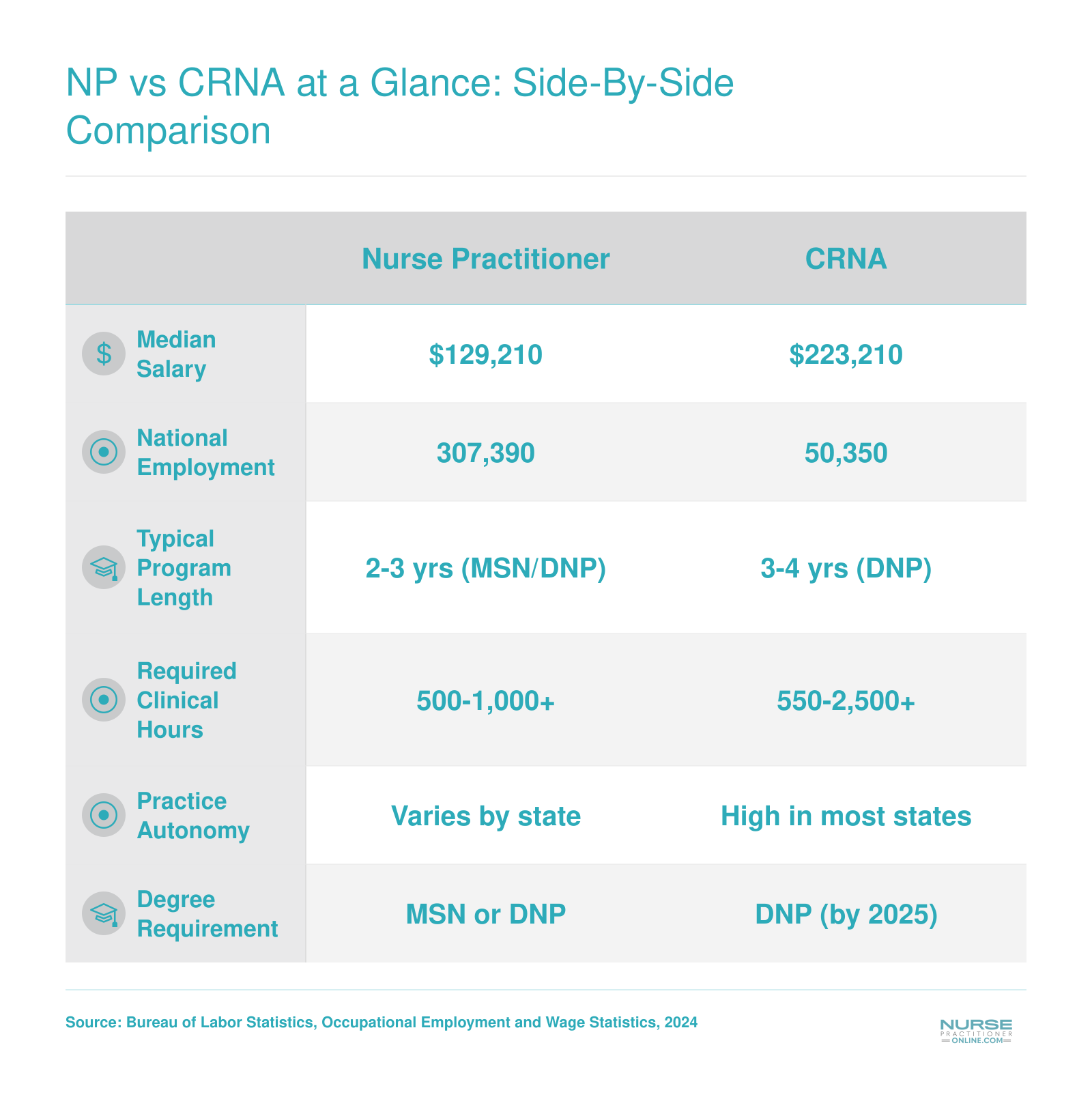
NP vs CRNA at a Glance: Side-By-Side Comparison
Before diving into the details, here is a quick-reference snapshot of how nurse practitioners and certified registered nurse anesthetists compare across key career dimensions. Salary and employment figures reflect 2024 national data from the Bureau of Labor Statistics.
What Does a Nurse Practitioner Do Vs. A CRNA?
The daily work of a nurse practitioner and a certified registered nurse anesthetist barely overlap, even though both roles require an advanced nursing degree and share a commitment to patient safety.
The NP's Day: Breadth Across Specialties
Nurse practitioners deliver primary and specialty care across a remarkably wide landscape. On a typical day, an NP in a family practice clinic might see 15 to 25 patients, diagnosing conditions that range from hypertension and diabetes to acute infections and mental health concerns. NPs prescribe medications, order and interpret labs, coordinate referrals, and counsel patients on prevention. That same scope of practice can look very different depending on the sub-specialty: a Family NP (FNP) manages all ages in an outpatient setting, a Psychiatric Mental Health NP (PMHNP) focuses on behavioral health, an Adult-Gerontology Nurse Practitioner (AGNP) cares for aging populations, and a Pediatric NP (PNP) treats children from birth through young adulthood.
Clinical settings are equally varied. NPs practice in outpatient clinics, urgent care centers, hospitals, VA facilities, school-based health centers, and increasingly through telehealth platforms. Many build longitudinal relationships with patient panels they follow for years, a defining feature of the role and one of its greatest rewards.
The CRNA's Day: Procedural Focus in High-Acuity Settings
CRNAs spend most of their time in operating rooms and procedure suites. A typical shift begins with pre-operative assessments, reviewing medical histories, airway evaluations, and anesthesia plans. Once the patient enters the OR, the CRNA induces and maintains anesthesia, monitors vital signs continuously, adjusts medications in real time, and manages the airway throughout surgery. After the procedure, the CRNA guides the patient through post-anesthesia recovery before the next case begins.
The environment is fast-paced and highly procedural. CRNAs work in hospital ORs, ambulatory surgery centers, labor and delivery units, and pain management clinics. Patient encounters are brief but carry significant acuity: every decision in the OR directly impacts whether a patient wakes up safely.
Patient Relationships: Longitudinal vs. Episodic
One of the starkest contrasts between these two paths is the nature of the patient relationship. NPs often follow the same individuals over months or years, managing chronic conditions and tracking progress. CRNAs typically meet a patient shortly before a procedure and hand off care within hours. If you thrive on continuity and coaching patients through long-term health goals, the NP model may feel more fulfilling. If you prefer high-stakes, focused encounters where your clinical skills produce immediate results, the CRNA environment is a natural fit.
Autonomy and Practice Authority
NP practice authority varies by state. Some states grant full practice authority, allowing NPs to evaluate, diagnose, and prescribe without physician oversight. Others impose reduced or restricted authority that requires a collaborative agreement or direct supervision. The regulatory landscape continues to evolve, and it is worth checking your state's current rules before committing to a program.
CRNAs, by contrast, have independent practice authority in most states. According to the American Association of Nurse Anesthesiology, CRNAs are the sole anesthesia providers in many rural hospitals and military settings. The 2024 removal of the federal physician-supervision requirement for Medicare anesthesia services further expanded CRNA autonomy nationwide.
Both roles offer meaningful independence, but the path to that independence, and the clinical setting in which you exercise it, looks quite different depending on which career you choose. For a broader look at how nurse practitioner specialties map to different practice environments, our specialties guide is a helpful starting point.
Education, Admissions & Training Timeline
The 2025 doctoral mandate for nurse anesthesia programs has reshaped the conversation around advanced practice nursing education, making the training gap between the NP and CRNA pathways wider than ever. If you are weighing these two routes, understanding the differences in prerequisites, program length, and admissions selectivity will help you plan realistically.
The NP Path
Nurse practitioner programs offer one of the most accessible on-ramps to advanced practice. You can pursue either an MSN (typically two to three years) or a DNP (three to four years), and many programs are available fully online or in a hybrid format, a major advantage for working nurses. If you are curious about the overall commitment, our guide on how hard it is to become a nurse practitioner breaks it down in detail. Key admissions benchmarks include:
- GPA floor: Most programs require a minimum of 2.75 to 3.0, with average accepted GPAs landing in the 3.3 to 3.6 range.
- RN experience: Preferred but often not required, so newer nurses can apply.
- GRE: Often not required.
- Clinical hours: Programs typically require 500 to 750 direct patient care hours.
- Acceptance rates: National figures generally fall between 40% and 70%, making NP programs comparatively open.
The CRNA Path
Becoming a nurse anesthetist demands a longer, more selective pipeline. Since 2025, all accredited nurse anesthesia programs award a doctoral degree (DNP or DNAP), and the program itself runs three to four years after you meet substantial prerequisites:
- Critical-care experience: A minimum of one year of ICU nursing is required, though admitted students typically have two to four years. At competitive programs such as Wake Forest, the average accepted applicant brings roughly three years of critical-care experience and four years of total RN experience.2
- GPA: The minimum is usually a 3.0, but the average accepted GPA ranges from 3.4 to 3.7.
- GRE: Required by approximately half of programs, with a typical target score of 300 or above.
- Clinical hours: Students complete a minimum of 2,000 clinical anesthesia hours during training, and the national average exceeds 9,300 hours.
- Acceptance rates: Programs admit roughly 20% to 40% of applicants, a significantly tighter window than NP programs.
Is CRNA School Harder to Get Into?
Yes, and the numbers make the gap clear. CRNA acceptance rates (20% to 40%) are roughly half those of many NP programs (40% to 70%). Beyond raw selectivity, CRNA prerequisites are more rigorous: mandatory ICU experience, higher average GPAs among admitted students, and a GRE requirement at about half of all programs. The combination of a demanding prerequisite period and limited seats means the CRNA admissions process is substantially more competitive.
Online vs. On-Campus Options
NP students benefit from a wide selection of online and hybrid programs, one reason the pathway is so popular among nurses who need scheduling flexibility. CRNA programs, by contrast, are almost entirely on-campus. The heavy simulation lab requirements and high-volume clinical rotations make remote delivery impractical for the vast majority of anesthesia curricula. If you decide to pursue the NP route, knowing how to prepare for NP school can set you up for success from day one.
Can a Nurse Practitioner Switch to Become a CRNA?
Yes, but the transition is not a shortcut. A practicing NP who wants to become a CRNA must meet the same ICU hour requirements (at least one year, ideally two or more) and complete a full doctoral nurse anesthesia program from the start. Your NP coursework will not substitute for anesthesia-specific didactic and clinical training. That said, the clinical maturity and advanced pharmacology background you bring as an NP can strengthen your application. If you are considering this pivot, start accumulating critical-care hours early and connect with a CRNA program advisor to map out a realistic timeline.
Questions to Ask Yourself
NP vs CRNA Salary Comparison by State
Salary gaps between nurse practitioners and CRNAs vary widely depending on where you practice. In states where both roles are well represented, CRNAs consistently out-earn NPs by $80,000 to $100,000 or more per year. The table below highlights states where Bureau of Labor Statistics data is available for both occupations, along with select top-paying states for each role individually.
| State | NP Median Salary | CRNA Median Salary | Approximate Difference |
|---|---|---|---|
| Arizona | $133,790 | $228,690 | +$94,900 |
| Connecticut | $138,960 | $227,930 | +$88,970 |
| California | $166,610 | N/A | N/A |
| New Jersey | $149,620 | N/A | N/A |
| New York | $145,390 | N/A | N/A |
| Oregon | $144,600 | N/A | N/A |
| Alaska | $145,450 | N/A | N/A |
| Washington | $140,220 | N/A | N/A |
| Massachusetts | $138,890 | N/A | N/A |
| Michigan | N/A | $234,520 | N/A |
| Indiana | N/A | $233,200 | N/A |
| North Dakota | N/A | $232,420 | N/A |
| Nebraska | N/A | $231,020 | N/A |
| Iowa | N/A | $229,950 | N/A |
| Texas | N/A | $227,580 | N/A |
| North Carolina | N/A | $226,460 | N/A |
| South Carolina | N/A | $225,800 | N/A |
| Louisiana | N/A | $225,440 | N/A |
| Maine | N/A | $229,900 | N/A |
Related Articles
NP vs CRNA Salary by Metro Area
Metro-level salary data highlights how location influences the pay gap between nurse practitioners and nurse anesthetists. In every metro where both roles are reported, CRNAs earn substantially more, though the size of the premium varies. The figures below come from the most recent Bureau of Labor Statistics Occupational Employment and Wage Statistics release.
| Metro Area | NP Median Salary | NP Mean Salary | CRNA Median Salary | CRNA Mean Salary |
|---|---|---|---|---|
| New York, Newark, Jersey City (NY, NJ) | $152,790 | $151,510 | N/A | $263,220 |
| Minneapolis, St. Paul, Bloomington (MN, WI) | $128,570 | $128,740 | $233,030 | $243,390 |
| Nashville, Davidson, Murfreesboro, Franklin (TN) | $116,160 | $112,610 | $203,400 | $198,430 |
| Los Angeles, Long Beach, Anaheim (CA) | $164,510 | $165,030 | N/A | N/A |
| Miami, Fort Lauderdale, West Palm Beach (FL) | $135,450 | $132,730 | N/A | N/A |
| Chicago, Naperville, Elgin (IL, IN) | $131,690 | $131,580 | N/A | N/A |
| Boston, Cambridge, Newton (MA, NH) | $138,890 | $146,850 | N/A | N/A |
| Atlanta, Sandy Springs, Roswell (GA) | $128,640 | $129,710 | N/A | N/A |
| Phoenix, Mesa, Chandler (AZ) | $134,630 | $132,670 | N/A | N/A |
| Philadelphia, Camden, Wilmington (PA, NJ, DE, MD) | $131,590 | $133,360 | N/A | N/A |
| Dallas, Fort Worth, Arlington (TX) | N/A | N/A | $204,020 | $233,050 |
| Detroit, Warren, Dearborn (MI) | N/A | N/A | $230,450 | $226,560 |
| Tampa, St. Petersburg, Clearwater (FL) | N/A | N/A | $197,660 | $187,140 |
| Charlotte, Concord, Gastonia (NC, SC) | N/A | N/A | $238,780 | $239,390 |
| Houston, Pasadena, The Woodlands (TX) | N/A | N/A | $235,490 | $236,150 |
| Kansas City (MO, KS) | N/A | N/A | $189,740 | $207,220 |
Tuition, Debt & Return on Investment
The financial decision between becoming a nurse practitioner or a nurse anesthetist often comes down to a classic tradeoff: a higher upfront investment in CRNA education can unlock substantially higher earnings, while NP school typically costs less and allows many students to work part-time, reducing the immediate financial strain.
The Upfront Cost vs. Long-Term Payoff
CRNA programs are rigorous, full-time, and typically last three years, with total tuition often ranging from $80,000 to $120,000 at public universities and up to $150,000 or more at private ones. Add living expenses and the inability to work during clinical rotations, and average student loan debt for new CRNAs routinely lands in the six figures. In contrast, NP programs vary more: a Master's or DNP can be completed in two to three years, with total tuition somewhere between $30,000 and $70,000, depending on the specialty and school. Many NP students continue working as RNs, defraying costs and borrowing less. When comparing online MSN NP programs, tuition differences across schools can be dramatic, making it well worth shopping around. Recent surveys from the American Association of Nurse Anesthetists (AANA) and the Council on Accreditation (COA) paint a clear picture of CRNA debt loads, while the American Association of Nurse Practitioners (AANP) and American Association of Colleges of Nursing (AACN) offer comparable NP figures. Be aware that these broad averages mask wide variation, so personal research matters.
Step 1: Start with Salary Data from BLS.gov
Before you can calculate return on investment, you need a baseline earning expectation. Visit www.bls.gov and search for "Nurse Anesthetists" and "Nurse Practitioners." The Occupational Outlook Handbook will show median annual wages and projected job growth for each role. This is your starting point for assessing how quickly a higher salary could offset higher debt. Keep in mind these numbers are national; state and metro area wages can differ significantly, so drill down for your intended region of practice.
Step 2: Research Actual Tuition Costs from School Websites
Tuition rates are not uniform. Pick two or three programs you are seriously considering and pull the most recent per-credit or per-semester rates directly from their financial aid or program pages. Note whether the school charges in-state versus out-of-state rates, and look for hidden fees like clinical placement or lab costs. Confirming that a school holds proper nursing program accreditation is also essential before committing financially. If a program publishes an estimated total cost of attendance including living expenses, that number is gold for your ROI analysis.
Step 3: Cross-Reference with Professional Association Debt Surveys
While school websites give sticker prices, real student debt often includes living expenses, interest accrual, and fees. For CRNAs, check the AANA's biennial Member Compensation and Debt Survey or the COA's Annual Report for the most accurate median debt at graduation. For NPs, the AANP National NP Sample Survey or AACN's data reports are reliable. These sources can tell you, for example, that median CRNA debt is $X, while median NP debt is $Y. Contact the financial aid office of your target programs to ask for their own average graduate indebtedness; this figure is often the most tailored to your specific situation.
Crunching the ROI: A Personalized Calculation
Once you have your expected salary (from BLS) and your likely total debt (from your schools and the surveys), a rough ROI becomes clear. Subtract the average NP salary from the average CRNA salary. Multiply that annual premium by the years you plan to work. Subtract the additional debt you would take on. For many, the CRNA premium pays for itself within three to five years, even when factoring in lost RN wages during school. But ROI isn't just dollars: flexibility, job satisfaction, and burnout rates matter too. The right choice balances your financial goals with the life you want to lead.
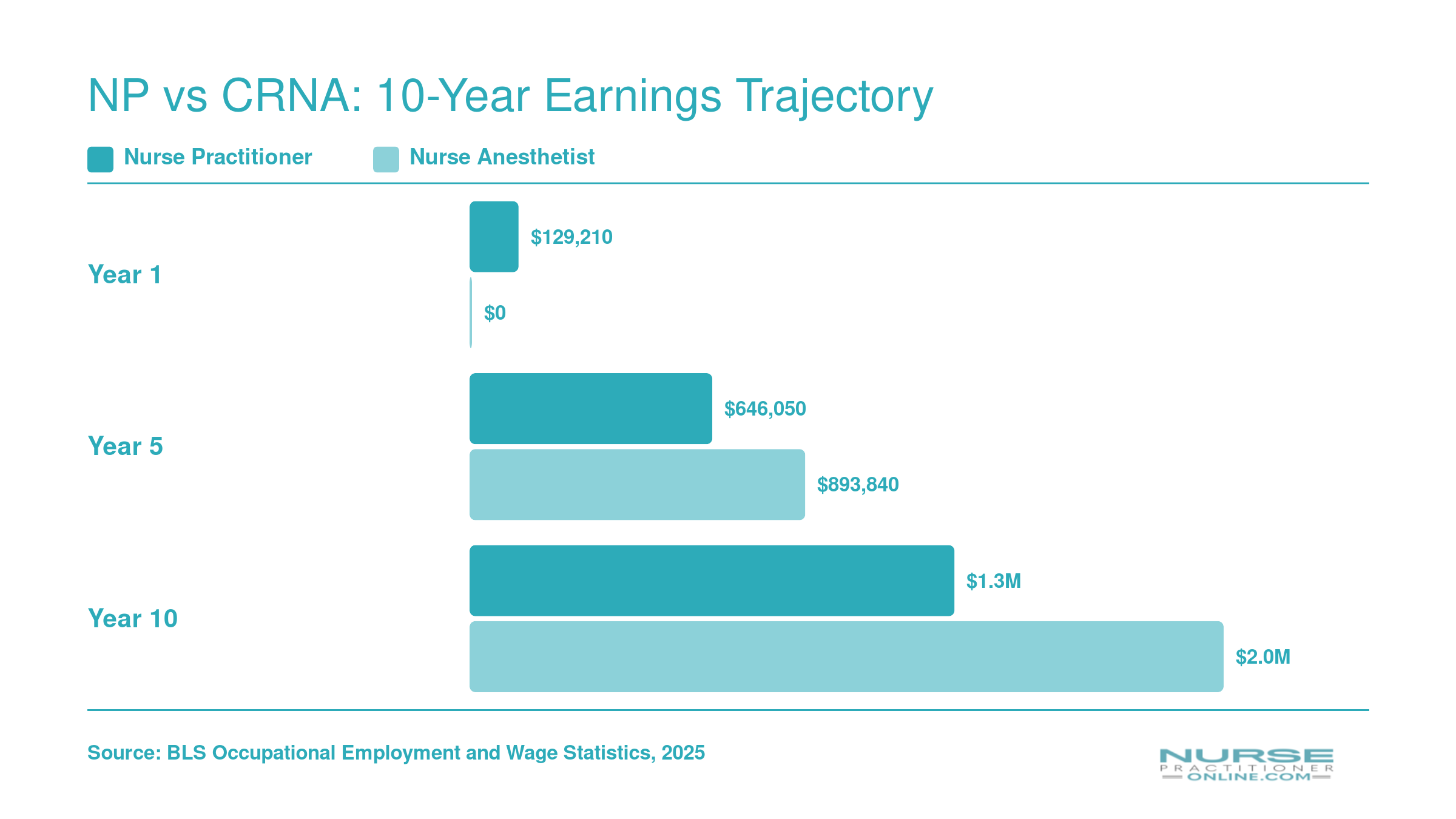
NP vs CRNA: 10-Year Earnings Trajectory
Because CRNA programs typically require one to two additional years of training compared to NP programs, nurse practitioners begin earning sooner. However, the CRNA salary premium closes that gap quickly. The projections below use BLS median salaries ($129,210 for NPs, $223,210 for CRNAs) applied over a 10-year window, with CRNAs assumed to start earning one year later due to longer training. These are approximate projections, not exact forecasts.
Work-Life Balance, Schedules & Burnout Rates
A Tale of Two Schedules: Clinic vs. OR
On the surface, a 40-hour week is typical for both nurse practitioners and CRNAs, but the rhythm of those hours couldn't be more different.1 Nurse practitioners in primary care, specialty offices, or retail clinics often work a Monday-through-Friday schedule with predictable daytime shifts, though those in urgent care or hospitalist roles should expect some evenings, weekends, and rotating coverage. By contrast, a CRNA's day is anchored to the operating room schedule, which can mean early-morning starts, occasional late finishes, and 24-hour call obligations in hospitals. In ambulatory surgery centers, CRNAs may enjoy a no-call, 40-hour schedule that more closely mirrors a typical clinic week, but that's not the norm across all practice settings.1
- NP schedule: Standard 9-to-5 in many outpatient roles; weekend or evening shifts common in acute care and retail clinics.
- CRNA schedule: Variable start times tied to first surgical case; call shifts often required (averaging a few nights or weekends per month depending on facility).
Burnout: Stressors on Both Sides
Burnout in advanced practice nursing looks different depending on the role. Data from the most recent Medscape APRN Burnout Report indicates that nurse practitioners commonly cite patient volume, administrative documentation, and feeling undervalued as key drivers. National surveys show that 53% of NPs feel underpaid, which amplifies dissatisfaction.2 In some states, burnout rates among NPs are hovering around 24 to 25%, a signal that the primary care pipeline is under strain.3 You can learn more about the causes and strategies for preventing nurse practitioner burnout. CRNAs, meanwhile, report the highest salary satisfaction among APRNs on wellness surveys, despite the high-stakes nature of anesthesia delivery.4 The operating room environment demands intense focus, but many CRNAs describe a deep professional fulfillment that buffers against emotional exhaustion.
- NP burnout triggers: Documentation overload, short appointment windows, and compassion fatigue.
- CRNA burnout triggers: Production pressure in busy ORs, call burden, and limited patient follow-up.
Part-Time, Locum, and Telehealth Options
Flexibility can make or break work-life balance, and here the two paths diverge. Nurse practitioners have a wider array of part-time and telehealth roles, making it easier to dial hours up or down as life demands. Many NPs now work hybrid schedules with some virtual visits, reducing commute stress. CRNAs can also find part-time or per-diem work, and locum tenens nurse practitioner positions (and their CRNA equivalents) command premium rates, often 20 to 30% above staff salaries, but those assignments usually require travel and irregular scheduling. If you need a predictable, family-friendly routine, NP roles (especially in outpatient specialties) tend to offer more control.
- NP part-time flexibility: Strong; telehealth and low-acuity clinics are especially accommodating.
- CRNA part-time flexibility: Possible through locums or surgery center per-diem, but less common and often less predictable.
So, Do CRNAs Have Better Work-Life Balance?
The answer is nuanced. A CRNA in an outpatient surgery center with no call and a 40-hour cap may feel less burned out than an NP drowning in 25-patient primary care days. Conversely, an NP who works four 10-hour telehealth shifts may enjoy far more flexibility than a hospital-based CRNA pulling 24-hour call every third night. Neither role guarantees a perfect balance; both require you to choose a practice setting that aligns with your personal priorities. Turnover data echo this: nurse practitioners leaving primary care is a well-documented trend often tied to unsustainable workflows, while CRNA turnover is less studied but can spike in facilities with heavy call demands.
A CRNA's higher upfront tuition can pay for itself within three to five years of practice, thanks to a median salary premium that exceeds $60,000 annually.
Job Outlook and Career Flexibility
Both advanced practice nursing roles are riding one of the strongest growth waves in all of healthcare, and there are no signs of that slowing down.
According to the Bureau of Labor Statistics, nurse practitioners are projected to grow by 40 percent between 2024 and 2034, adding roughly 128,400 new positions to a field that already employed about 320,400 practitioners in 2024.1 That growth rate is nearly five times the national average for all occupations. CRNAs, nurse midwives, and nurse practitioners are tracked together in a broader BLS grouping, which projects 35 percent growth and roughly 32,700 annual openings across those roles through 2034.2 Either way you slice the numbers, both career paths offer exceptional job security.
NP Flexibility: Wide Open by Design
One of the most underappreciated advantages of the NP path is how much room it gives you to pivot. An FNP who starts out in primary care can shift into urgent care, cardiology, or dermatology without returning to school in many states. Adding a psychiatric-mental health nurse practitioner certification opens yet another door, one that is especially valuable given the ongoing national shortage of mental health providers. Over a career spanning 25 to 30 years, that kind of lateral mobility lets you follow your interests, chase better pay, or simply avoid burnout by changing your clinical environment.
Beyond the exam room, NPs also have a natural on-ramp into non-clinical nurse practitioner jobs. Health policy, pharmaceutical consulting, academic faculty positions, and hospital administration all actively recruit NPs who want to step back from direct patient care or blend it with leadership work.
CRNA Flexibility: Narrower Specialty, Broader Reach
CRNAs work within a more defined clinical lane, but that does not mean career options are limited. Pain management, regional anesthesia, and military or federal practice are popular lateral moves. On the non-clinical side, simulation education, healthcare administration, and expert witness consulting are well-established paths for experienced CRNAs ready for a new challenge.
Switching Lanes Later
If you are wondering whether you can change direction mid-career, the honest answer is: it depends on which way you want to go. An NP who decides to become a CRNA will need to meet ICU experience requirements and complete a full CRNA program, a serious but achievable undertaking. Going the other direction, from CRNA to NP, is theoretically possible but uncommon in practice and still requires completing a separate NP program. Neither switch is a quick detour, so it is worth getting the original decision as right as you can from the start.
How to Decide: NP or CRNA?
There is no universal "better" between NP and CRNA. The right decision hinges entirely on your personal priorities, and this framework will help you self-sort. Nurses who thrive in one role often feel miscast in the other, so honest self-assessment is your most powerful tool.
A Four-Dimensional Decision Framework
Assess yourself across four dimensions: clinical personality, financial goals, lifestyle priorities, and timeline willingness. Where you land on each will point you toward the more natural fit.
Clinical Personality: Procedural vs. Relational
- Procedural focus: If you enjoy high-stakes, hands-on technical work and prefer brief, intense patient interactions, CRNA may suit you better.
- Relational focus: If you value building long-term patient relationships, educating, and managing care over time, NP practice is likely more fulfilling.
Financial Goals and Debt Tolerance
- Earning ceiling: CRNAs earn substantially more, often $200,000+, but face higher tuition and longer training. NPs earn strong but typically lower salaries with less debt.
- Return on investment: CRNA programs often cost $120,000 to $180,000 and take three years; NP programs can be completed in two to three years for $30,000 to $80,000. The CRNA salary premium can offset the higher upfront investment within a few years if you prioritize maximum lifetime earnings. For those considering the doctoral route on the NP side, weigh whether a DNP degree is worth it before committing.
Lifestyle and Schedule Preferences
- Predictability: Many NP roles offer regular clinic hours and less on-call duty, ideal for those with family commitments or burnout concerns.
- Compressed schedules: CRNAs often work 12- or 24-hour shifts with more days off, but may also have overnight, weekend, and holiday obligations. The trade-off is higher pay for less predictable hours.
Timeline Willingness
- Years to practice: NPs typically need two to three years of post-BSN education; CRNAs require one to two years of ICU experience plus a three-year doctorate, often totaling five to seven years before independent practice. If you want to understand how long it takes to become a nurse practitioner, the NP timeline may align better with your goals.
The Power of Shadowing
The single most common piece of advice from both NPs and CRNAs: shadow a practitioner in each role for at least one full shift. You cannot fully grasp the day-to-day until you witness the work environment, pace, and emotional demands firsthand. Contact local hospitals, private practices, or professional organizations to arrange observation hours.
Which Is Better? A Direct Answer
Neither role is objectively better. NP and CRNA careers are both rewarding, high-impact, and respected. The right choice is the one that aligns with your strengths, values, and life goals. What feels like a perfect fit for your colleague may leave you drained or disengaged.
Self-Assessment: Mapping Your Answers
If you answered the earlier "Ask Yourself" prompts with a strong preference for direct, intensive procedural care and maximizing income, the CRNA path likely merits deeper exploration. If you prioritized continuous patient relationships, broad practice settings, and a faster entry into advanced practice, the NP route may be your better match. Honesty about your debt tolerance and schedule flexibility is critical.
Next Steps
Research accredited programs on the American Association of Nurse Practitioners (AANP) and American Association of Nurse Anesthetists (AANA) websites. Connect with current students and recent graduates through these organizations' online communities. Their unfiltered perspectives will complement what you learn from shadowing and help you make a confident, informed decision.
Frequently Asked Questions: NP vs CRNA
Choosing between an NP and a CRNA path raises a lot of practical questions. Below are quick, data-grounded answers to the ones working nurses ask most often. For deeper dives, refer to the relevant sections earlier in this article.
- Who makes more money, CRNA or NP?
- CRNAs earn significantly more on average. According to the Bureau of Labor Statistics, the median annual salary for nurse anesthetists is roughly $212,000, while nurse practitioners earn a median of about $126,000. That gap of more than $60,000 per year holds across most states, though exact figures vary by region, specialty, and practice setting, as detailed in the salary comparison tables above.
- Can you make $300K as a nurse practitioner?
- It is uncommon but possible. NPs who reach $300,000 or more typically work in high-paying specialties such as psychiatric mental health or acute care, take on administrative or ownership roles, practice in underserved or high-cost-of-living areas, or combine clinical income with overtime and side work. For most NPs, however, compensation falls well below that threshold. CRNAs reach the $300K mark more frequently, especially in rural or independent-practice states.
- How long does it take to become a CRNA vs an NP?
- From BSN to practice, the NP route generally takes two to three years for a master's degree or three to four years for a DNP. The CRNA path typically requires at least one year of critical care ICU experience before applying, then three to four years in a doctoral nurse anesthesia program. In total, expect roughly five to six years from BSN to CRNA practice compared to two to four years for an NP.
- Is CRNA school harder to get into than NP school?
- Yes, CRNA programs are generally more competitive. Most require a minimum GPA of 3.3 or higher, strong GRE scores, and at least one year (often two) of adult critical care nursing experience. NP programs also have prerequisites, but acceptance rates tend to be higher, and clinical experience requirements are usually broader. The admissions and training section earlier in this article breaks down the specific benchmarks for each path.
- Can a nurse practitioner switch to become a CRNA?
- Yes, but it is not a direct lateral move. A practicing NP would need to gain the required ICU experience (typically one to two years in an adult critical care unit), meet CRNA program prerequisites, and complete a full doctoral nurse anesthesia program. Prior graduate coursework may transfer for some didactic credits, but most clinical and anesthesia-specific training must be completed from scratch. The total transition timeline is usually four to six years.
- Do CRNAs have a better work-life balance than NPs?
- It depends on the setting. CRNAs often work scheduled shifts in operating rooms and surgical centers, which can offer predictability but may include nights, weekends, and on-call hours. NPs, particularly in primary care or outpatient clinics, frequently enjoy more traditional weekday schedules. However, NPs in emergency or hospital settings may face similar irregular hours. Burnout rates differ by specialty and employer. The work-life balance section above explores these trade-offs in detail.