Most important takeaways…
- DNP-prepared NPs earn roughly $7,000 more per year than MSN-prepared NPs, with wider gaps in leadership and CRNA roles.
- Post-master's DNP programs typically cost $30,000 to $60,000, while BSN-to-DNP pathways can exceed $100,000 in total expenses.
- Break-even timelines range from under five years for CRNAs and executives to over a decade for NPs who stay in general clinical roles.
- No state requires the DNP for advanced practice licensure in 2026, but employer preferences and academic hiring standards increasingly favor it.
More than 400 post-master's and BSN-to-DNP programs now enroll students across the United States, yet the median salary gap between DNP-prepared and MSN-prepared nurse practitioners sits at roughly $7,000 a year. For a degree that can cost anywhere from $25,000 to over $100,000 depending on pathway and institution, that number alone gives many working NPs pause.
Four concerns surface repeatedly: the upfront cost of tuition and lost clinical hours, confusion over what the "doctor" title actually changes at the bedside, limited evidence that the DNP unlocks new clinical scope beyond the MSN, and skepticism about whether the salary premium justifies years of additional study. Each of these deserves a closer look grounded in current compensation data, real tuition figures, and break-even modeling rather than aspirational talking points. The AACN's long-delayed push to make the DNP a standard entry degree has not yet materialized in any state's licensing requirements, which only sharpens the cost-benefit question for nurses weighing the commitment today.
DNP Vs. MSN: How Much More Do DNP-Prepared Nurses Earn?
Nurse practitioners with a DNP earned a median of $114,000 compared to $107,000 for MSN-prepared NPs according to national compensation surveys, a premium of roughly $7,000 annually.1 That figure provides a baseline, but the full picture requires looking at multiple roles, specialty areas, and how the DNP shapes career trajectories over time.
What BLS Data Tells Us (and What It Doesn't)
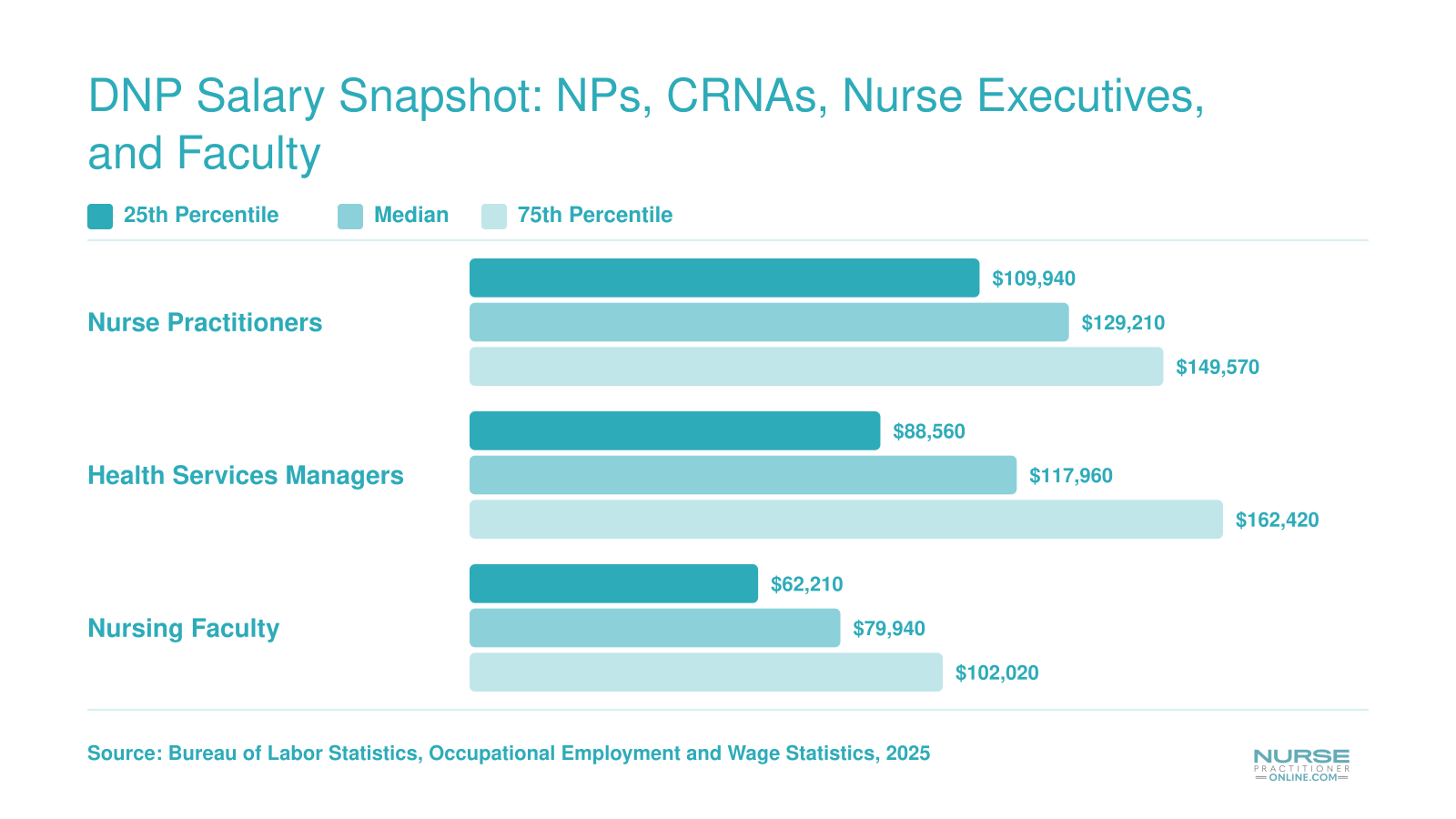
The Bureau of Labor Statistics reports that nurse practitioners nationally earn a median salary of $129,210, with those at the 75th percentile reaching $149,570.2 Medical and health services managers, a common path for DNP graduates moving into leadership, show a median of $117,960 and a 75th-percentile wage of $162,420. Nursing instructors and postsecondary teachers earn a median of $79,940, climbing to $102,020 at the upper quartile.
Here is the limitation: BLS data groups all NPs together regardless of terminal degree. The agency does not separate MSN-prepared practitioners from those holding a DNP. This means you cannot rely on federal occupational data alone to calculate the exact return on your doctoral investment.
Survey Data on the DNP Premium
Professional association surveys help fill that gap. Compensation studies from organizations tracking advanced practice nurses have documented a salary premium ranging from $5,000 to $8,000 for DNP holders compared to MSN peers in similar clinical roles, representing roughly a four to seven percent difference.1 For nurse practitioners specifically, that premium has hovered around $7,000 annually.
CRNAs show a similar pattern. MSN-prepared nurse anesthetists reported median earnings of $188,000, while DNP-prepared CRNAs earned approximately $195,000.1 Clinical nurse specialists and nurse-midwives saw smaller differentials, often in the $2,000 range, suggesting the degree's financial impact varies considerably by specialty.
Do NPs or DNPs Make More Money?
The honest answer: role and setting matter more than the letters after your name. A DNP-prepared NP working in primary care may earn comparably to an MSN peer in the same clinic. The salary gap widens when the DNP opens doors that remain closed to MSN-only nurses. If you are weighing the pros and cons of a DNP degree, compensation is just one variable in a broader equation.
Administrative titles such as chief nursing officer, vice president of patient services, or director of nursing frequently list the DNP as preferred or required. Academic positions at research universities increasingly expect doctoral preparation for tenure-track faculty lines. These roles push compensation well above clinical practice norms. Health services managers at the 75th percentile earn over $162,000, and executive nursing leadership can exceed that substantially.
The degree itself does not automatically generate higher pay. Instead, it expands your eligibility for positions where advanced compensation is built into the role. If your career goals include leadership, policy influence, or academic appointments, the DNP becomes a credential that unlocks those pathways rather than simply adding a premium to your current paycheck. Understanding the DNP admission requirements early can help you plan a realistic timeline for that investment.
DNP Salary Snapshot: NPs, CRNAs, Nurse Executives, and Faculty
How do salaries compare across the most common DNP career tracks? The grouped bar chart below lines up median pay alongside the 25th and 75th percentile ranges for nurse practitioners, medical and health services managers (a common path for nurse executives), and nursing faculty. The spread between the lower and upper quartiles reveals how much room each role offers for earnings growth.
DNP Salary by Role and Specialty
How much does a DNP-prepared nurse earn by specialty, and which roles or practice settings can realistically reach the $300,000 income level?
Salaries for DNP-prepared nurses can vary dramatically depending on clinical focus, geographic region, and employment model. While federal data from the Bureau of Labor Statistics groups all nurse practitioners together, specialty-specific surveys from professional associations and compensation reports provide the granular detail needed for career planning.
Salaries by Clinical Specialty
- Family Nurse Practitioner (FNP): According to the 2024 AANP National NP Compensation Survey, FNPs with a DNP report median annual earnings of approximately $115,000, with top-earning quintiles exceeding $150,000. The DNP often provides a slight increase over MSN-prepared colleagues, particularly in leadership or teaching roles.
- Psychiatric-Mental Health Nurse Practitioner (PMHNP): Medscape's 2025 NP Compensation Report highlights PMHNPs as among the highest-earning non-anesthesia specialties, with a median of $130,000 and high-end earnings above $160,000. DNP-level PMHNPs in private practice or tele-psychiatry may see even higher numbers due to growing mental health demand.
- Certified Registered Nurse Anesthetist (CRNA): The AANA's 2024 compensation survey reports a national average of $195,000 for CRNAs, but many with DNPs step into chief CRNA or director roles, often pushing total compensation beyond $250,000. In independent practice states, experienced DNP CRNAs can bill directly and may reach $275,000 or more.
- Clinical Nurse Specialist (CNS): While fewer in number, CNSs with a DNP hold advanced system-level roles; salaries typically range from $105,000 to $140,000, with those in academic health centers or consulting earning at the higher end, according to PayScale data filtered for the DNP credential.
For a broader look at how these figures compare across the profession, see our breakdown of highest paid nurse practitioner specialties.
Salaries in Executive and Leadership Roles
Nurse executives who earn a DNP to bolster their credentials for CNO, VP of Patient Care, or health system COO roles often see total compensation packages from $180,000 to $250,000, not including bonuses. These figures are drawn from executive compensation reports and self-reported data on Glassdoor and Indeed, specifically filtered for DNP-holding leaders.
The $300K Question: Practice Ownership and Entrepreneurship
The high-end income that captures attention online, commonly $300,000 or more, almost always reflects entrepreneurial NPs, not traditional clinical employment. The AANP's practice ownership resources note that independent clinic owners in cash-pay aesthetics, functional medicine, or direct primary care in affluent markets can net between $250,000 and $400,000 annually. This income level requires business acumen, regulatory expertise, and often a significant start-up investment. While online aggregators like Indeed and PayScale do show outliers at this level for DNP-qualified self-employed individuals, these figures are far from the norm and should not be expected in typical W-2 staff positions.
Tracking the Latest Salary Data
Because compensation can shift quickly with healthcare policy and local demand, rely on multiple sources. Visit the AANP, AANA, and AACN websites for member-accessible salary surveys and reports. If you are still exploring family nurse practitioner programs, many school program pages publish graduate placement salary ranges for their DNP completers. Filter PayScale, Glassdoor, or Medscape's annual reports by the DNP degree and your desired specialty to spot trends; just remember that these tools often lag and can reflect a mix of MSN and DNP data. Cross-referencing ensures you build a realistic expectation for your own DNP return on investment.
Highest-Paying States for DNP-Prepared Nurses
Where you practice can have a dramatic effect on your earning potential as a DNP-prepared nurse practitioner. The table below ranks the top 10 states by median NP salary, based on the latest Bureau of Labor Statistics data. Keep in mind that high nominal salaries in states like California and New York come with a significantly higher cost of living. States such as Oregon, New Mexico, and Arizona may deliver stronger real purchasing power. It is also worth noting that several of the highest-paying states, including California, Oregon, Washington, Connecticut, New Mexico, Montana, and Arizona, grant NPs full practice authority, which tends to correlate with both higher earnings and greater professional autonomy, making a DNP especially valuable in those markets.
| Rank | State | Median NP Salary | Full Practice Authority | Cost of Living Context |
|---|---|---|---|---|
| 1 | California | $166,610 | Yes | Very high cost of living offsets the top salary; real purchasing power may be lower than it appears |
| 2 | New Jersey | $149,620 | No (reduced practice) | Above-average cost of living, particularly in northern counties near New York City |
| 3 | Alaska | $145,450 | Yes | High cost of living due to remote geography, though some employers offer housing or relocation benefits |
| 4 | New York | $145,390 | No (reduced practice) | Very high cost of living, especially in the New York City metro area |
| 5 | Oregon | $144,600 | Yes | Moderate cost of living outside Portland; strong real purchasing power relative to salary |
| 6 | Washington | $140,220 | Yes | Higher cost of living in the Seattle metro, more moderate elsewhere in the state |
| 7 | Connecticut | $138,960 | Yes | Above-average cost of living, though lower than neighboring New York |
| 8 | Massachusetts | $138,890 | No (reduced practice) | High cost of living in the Boston metro; competitive NP job market |
| 9 | New Mexico | $138,440 | Yes | Below-average cost of living statewide, making this one of the best states for real NP earnings |
| 10 | Arizona | $133,790 | Yes | Moderate cost of living, especially outside the Phoenix metro, offering solid purchasing power |
How Much Does a DNP Cost? Tuition and Hidden Expenses
The total price of a Doctor of Nursing Practice degree is the sum of tuition, per-semester fees, books and software, clinical placement costs, and the income you give up while completing clinical hours. Sticker prices vary widely by pathway and school type, so before deciding whether the DNP is worth the investment, it helps to map the real numbers.
Tuition by Pathway
National averages from recent program surveys give a useful starting point.1 A post-master's DNP typically requires 32 to 40 credits at roughly $561 per credit, putting average total tuition near $21,000. The BSN-to-DNP pathway is a much larger undertaking at 65 to 82 credits, with average total tuition closer to $41,000.
Individual programs can sit well above those averages, especially at research universities. The University of Illinois Chicago DNP program, for example, charges around $1,129 per credit.2 Meanwhile, Herzing University's post-MSN DNP runs about $770 per credit.3 Multiply by total credits and you can see how published ranges of $30,000 to $120,000 across the market are realistic, particularly for BSN-to-DNP students at private or out-of-state institutions.
The Hidden Costs
Tuition is only part of the bill. Most nurses underestimate the extras:
- Fees: Technology, library, and registration fees often add $300 to $400 per semester.1
- Books and software: Plan on $2,000 to $3,000 across the program.1
- Clinical placement: Some schools charge preceptor or placement fees, and travel to clinical sites adds up.
- DNP project expenses: Data tools, printing, and conference travel for dissemination.
- Lost income: Clinical hours are unpaid, and many students cut back on shifts during the project year.
Financial Aid and Employer Support
The good news: DNP students have more funding options than they often realize. Federal Direct Unsubsidized and Grad PLUS loans cover most cost-of-attendance gaps. Hospital systems frequently offer tuition reimbursement, often $5,000 to $10,000 per year, especially for staff who commit to stay post-graduation. The HRSA Nurse Faculty Loan Program forgives up to 85 percent of the loan balance for graduates who teach in nursing programs, and many states fund scholarships for nurses who agree to work in underserved areas.
Pathway Comparison
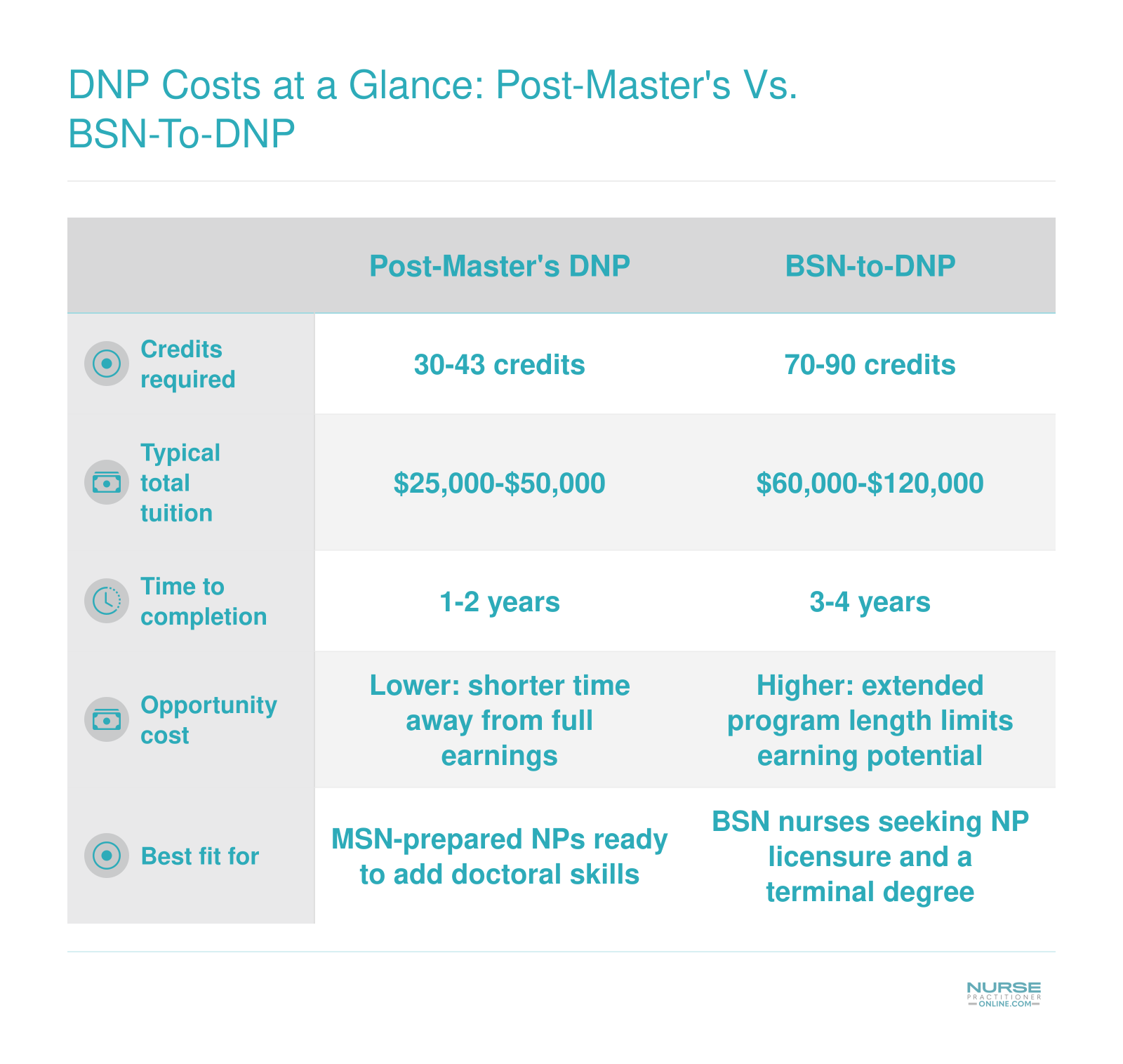
If you already hold an MSN, the post-master's route is meaningfully cheaper and faster, typically two years and less than half the credits of a BSN-to-DNP. The BSN-to-DNP costs more up front but consolidates two degrees into one continuous program.
DNP Costs at a Glance: Post-Master's Vs. BSN-To-DNP
The two main DNP pathways differ significantly in scope, cost, and time commitment. The table below puts them side by side so you can weigh each option against your current credentials, budget, and timeline.
DNP Return on Investment: How Long to Break Even
The core tension every nurse considering a DNP faces is simple: you are being asked to spend real money now in exchange for higher earnings later. The question is whether that tradeoff actually pencils out, and the honest answer is that it depends heavily on which path you take and what you plan to do with the degree.
The Post-Master's Breakeven Scenario
For nurses who already hold an MSN and are returning for a post-master's DNP, total program costs typically land in the $40,000 to $60,000 range depending on the school and credit load. Using $50,000 as a working figure, the math is straightforward. Survey data from AMN Healthcare and CompHealth consistently show DNP-prepared nurses earning a salary premium in the range of 8 to 12 percent over similarly experienced MSN-prepared counterparts.12 On a base salary of $110,000 to $120,000, that translates to roughly $10,000 to $15,000 per year in additional earnings.
At a $12,000 annual premium, you recover $50,000 in just over four years. At a more modest $10,000 premium, you are looking at five years. Continue working during the program and the clock starts ticking before you even graduate, which can shave a year or more off that timeline.
The BSN-to-DNP Scenario
Students entering directly from a BSN face higher total costs, often $80,000 to $120,000 across a longer program. The silver lining is that they reach the DNP without paying two separate rounds of graduate tuition. They skip the MSN-then-DNP sequence entirely, which matters if you know early on how long it takes to become a nurse practitioner and are certain you want to practice at the doctoral level. Breakeven for this group is longer on paper, but lifetime earnings over a full career can still favor the direct path when you account for the years of MSN-level tuition that were never spent.
When the ROI Is Strongest and Weakest
The numbers shift considerably based on specialty and setting. The return on investment tends to be strongest for:
- CRNAs: who command some of the highest compensation in nursing regardless of degree level, and for whom the DNP is increasingly expected
- Nurse executives: moving into C-suite or administrative roles where the credential carries institutional weight
- Faculty pursuing academic positions: where some institutions offer loan repayment assistance and the DNP is becoming a baseline hiring requirement
The ROI is weakest for family nurse practitioners in saturated metropolitan markets where the salary premium over MSN-prepared peers is modest and competition for positions is high. In those cases, the breakeven timeline can stretch to seven years or beyond, and the financial case alone is harder to make.
The Honest Range
Across pathways and specialties, a realistic breakeven range sits between three and seven years. Indeed salary data shows DNP-prepared nurses averaging around $110,912 nationally, while nurse practitioners overall average approximately $122,054, reflecting how specialty choice and experience shape the calculus.3 Nurses who continue working during a part-time online program, enter a high-demand specialty, or move into leadership or academia after graduating tend to land at the shorter end. Those entering saturated markets or taking time away from clinical work to complete the degree full-time will typically fall toward the longer end. Neither outcome is a failure. It just means the numbers should be part of the conversation, not the whole conversation.
Career Benefits and Common Concerns About the DNP
The DNP opens doors that the MSN simply cannot, but only if you walk through the right ones.
Where the DNP Earns Real Respect
The question of whether the DNP degree is respected has a clear answer in 2026: yes, increasingly so, and in places that matter for career trajectory. Health systems have spent the last decade elevating DNP-prepared nurses into director-level and C-suite positions that once defaulted almost exclusively to candidates with MHA or MBA credentials. Executives who oversee quality improvement, population health, or nursing operations are now frequently DNP-prepared, and many job postings for those roles list the degree as preferred or required. If your goal is clinical leadership or health system administration, the DNP carries genuine weight.
The academic path is equally compelling. Nursing faculty shortages remain severe, and the DNP qualifies you for clinical faculty appointments at a time when schools are actively competing for qualified instructors. HRSA loan forgiveness programs have expanded incentives for nurses who move into faculty roles, which can materially change the financial calculus on what you spend for the degree. As momentum grows, some observers argue the degree may eventually become standard, a trend explored in discussions about DNP entry-to-practice.
Practice Authority: Credibility Beyond the License
In full-practice-authority states, the DNP is not a legal requirement for independent practice. An MSN-prepared NP and a DNP-prepared NP hold the same prescriptive authority. Where the DNP adds value is in credibility: during negotiations with hospital credentialing committees, in policy conversations, and when NPs are asked to defend their scope of practice to administrators or legislators.
In restricted-practice states, that credibility matters even more. DNP-prepared NPs are consistently better positioned to participate in scope-of-practice advocacy, serve on state boards, and engage in the legislative work that moves those states toward greater autonomy. If you want a practical roadmap for that kind of engagement, the nurse practitioner health policy toolkit is a useful starting point.
Three Concerns Worth Taking Seriously
Not every reservation about the DNP is unfounded. Three come up repeatedly, and each deserves a straight answer.
- Title friction: The "Doctor" title creates real friction in clinical settings. Some physicians push back; some patients are confused. The standard navigation strategy is straightforward: introduce yourself by name and role, clarify your credentials when asked, and let your clinical competence carry the conversation. The friction is manageable, but pretending it does not exist sets you up for awkward moments.
- No new clinical skills: The DNP does not teach new clinical techniques or expand your scope of practice on its own. NPs who earn the degree hoping for greater autonomy at the bedside are often disappointed. The degree develops systems thinking, research application, and leadership capacity. If clinical skill-building is what you need, additional certification or fellowship training is the relevant path.
- Modest salary bump in the same role: If you earn a DNP and stay in the same clinical position, the salary premium is real but modest. The return on investment concentrates in role changes, not automatic raises. NPs who leverage the degree to move into leadership, academia, or specialized practice see the financial payoff. Those who do not change roles may wait years to recover tuition costs through incremental pay increases alone.
Pros and Cons of Getting a DNP
Deciding whether the DNP is worth it comes down to your career goals, financial situation, and tolerance for a multi-year commitment. The degree opens real doors, but it is not a universal upgrade for every nurse practitioner. Here is a balanced summary of the strongest arguments on each side.
Pros
- Higher earning ceiling, especially for CRNAs, nurse executives, and NPs in administrative or specialized roles
- Eligibility for senior leadership positions in health systems that increasingly require a doctoral credential
- Access to full-time faculty appointments at universities that prefer or mandate a terminal nursing degree
- Future-proofing your career ahead of the AACN's push to make the DNP the standard entry credential for advanced practice
- Greater professional credibility and influence in interdisciplinary settings, policy work, and evidence-based practice initiatives
Cons
- Significant tuition costs, often ranging from $30,000 to over $100,000 depending on program type and institution
- Modest salary bump for bedside clinical NPs, where the DNP alone may not meaningfully increase take-home pay
- Time commitment of one to three additional years of study on top of an already demanding work schedule
- Potential title confusion or friction in clinical settings where patients and colleagues may not understand the doctoral role
- No guaranteed expansion of scope of practice, since licensure and prescriptive authority are governed by state law, not degree level
The Future of the DNP: Is It Becoming the Standard?
The American Association of Colleges of Nursing (AACN) first recommended in 2004 that the DNP become the entry-level degree for advanced practice nursing by 2015. More than a decade past that initial target, as of 2026, no state board of nursing requires the DNP for nurse practitioner licensure, and no NP certifying body requires it for certification. The recommendation remains just that: a recommendation, not a mandate.
Current Policy Landscape
The National Organization of Nurse Practitioner Faculties (NONPF) endorsed the DNP as the entry-level degree by 2025, but enforcement mechanisms do not exist. Meanwhile, the National Association of Neonatal Nurse Practitioners (NANNP) reaffirmed its opposition to a mandatory DNP in 2022, citing concerns about workforce supply and educational accessibility.2 MSN NP programs remain fully operational in 2026, and graduates sit for the same certification exams and hold the same licensure as DNP-prepared nurses. No accrediting body or state has announced plans to phase out the MSN pathway in the coming years.
Will the DNP Become Required for Nurse Practitioners?
The short answer: not yet, and likely not soon. For a deeper look at where things stand, see our overview of the current status of the DNP requirement for nurse practitioners in 2026. The trend line suggests a slow drift toward preference rather than requirement. Employer hiring data from 2025 and 2026 show that most health systems treat MSN and DNP credentials as equivalent for clinical NP roles. Where the DNP does confer an advantage is in leadership positions and academic faculty appointments, where doctoral preparation is often preferred or required for senior roles.
No large-scale surveys from the American Association of Nurse Practitioners (AANP) or hospital HR departments indicate widespread DNP requirements for clinical practice. If your goal is direct patient care, the MSN remains fully competitive for the foreseeable future.
Practical Advice Based on Career Stage
For nurse practitioners early in their careers, the trajectory suggests the DNP may become the expected credential within 10 to 15 years, especially for those interested in executive, policy, or faculty roles. If you're considering this path, reviewing DNP prerequisites early can help you plan your timeline. Earning the DNP now or within the first decade of practice positions you ahead of a potential shift and opens doors to non-clinical advancement.
For experienced NPs nearing retirement, the investment may not pay off. If you have 5 to 10 years of practice remaining and no interest in leadership or teaching, the MSN credential will serve you well through the end of your clinical career. The return on investment diminishes when the time horizon is short and the salary differential for clinical roles is modest.
The Bottom Line
The DNP is becoming more common but not compulsory. Policy discussions continue, but no evidence suggests a mandate is imminent. If you value flexibility, leadership opportunities, and future-proofing your credentials, the DNP offers those benefits. If you prioritize cost, time, and immediate clinical practice, the MSN remains a strong, viable path in 2026.
Frequently Asked Questions About the DNP
Deciding whether to pursue a DNP raises plenty of practical questions, from salary expectations to timeline and long-term career value. Below are answers to the questions nurses ask most often, grounded in current salary data and program trends.
- Is the DNP degree respected?
- Yes. The DNP is the highest practice-focused degree in nursing, and it is recognized by the AACN, major health systems, and credentialing bodies. Employers increasingly view DNP graduates as leaders in evidence-based practice, quality improvement, and health policy. In academic settings, a DNP qualifies nurses for clinical faculty and administrative roles that may not be open to MSN-prepared candidates.
- How can a nurse practitioner earn $200,000?
- Reaching $200,000 is realistic for NPs who specialize in high-demand fields such as certified registered nurse anesthesiology, acute care, or psychiatric mental health. Working in states with full practice authority, negotiating productivity bonuses, taking on leadership duties, or adding per diem shifts can all push total compensation above that mark. A DNP credential can strengthen your negotiating position for these higher-paying roles.
- Can a nurse practitioner make $300,000?
- While uncommon in salaried positions, some NPs do reach $300,000 through a combination of strategies. CRNAs in high-cost or underserved markets sometimes cross that threshold. NPs who own independent practices, consult, or combine clinical work with academic appointments and speaking engagements can also approach that level. It typically requires years of experience, entrepreneurial effort, and a specialty with strong market demand.
- Do NPs with a DNP make more money than those with an MSN?
- On average, yes. DNP-prepared nurse practitioners tend to earn a modest salary premium over MSN-prepared NPs in similar roles, and the gap widens in leadership, academic, and executive positions. The advantage is most pronounced for CRNAs and nurse executives, where the DNP often unlocks higher-tier compensation. The exact difference varies by specialty, geography, and employer.
- Will the DNP become required for nurse practitioners?
- No state currently mandates a DNP for NP licensure, but the trend is moving in that direction. The AACN has endorsed the DNP as the entry-level degree for advanced practice since 2004, and a growing number of programs are transitioning from MSN to DNP tracks. While a firm deadline has not been set, earning a DNP now may protect your credentials against future regulatory changes.
- How long does it take to break even on a DNP degree?
- Most nurses can expect to recoup their investment within three to seven years, depending on tuition costs and the salary increase they achieve. Post-master's DNP students, who typically spend less on tuition and finish in two to three years, often break even faster. Factoring in loan interest and opportunity costs, a conservative estimate for BSN-to-DNP graduates is closer to the five to seven year range.
- Should I choose a post-master's DNP or a BSN-to-DNP program?
- If you already hold an MSN and are practicing as an NP, a post-master's DNP is usually the faster and more cost-effective path, often requiring only 30 to 40 credits. A BSN-to-DNP program suits nurses who want to earn their advanced practice credential and doctoral degree in one continuous track. Your decision should weigh total credit hours, tuition, clinical requirements, and how soon you want to begin practicing at the NP level.
- Is the DNP worth it for experienced NPs over 50?
- It can be, depending on your goals. If you want to move into teaching, executive leadership, or policy work, a DNP opens doors that experience alone may not. Post-master's programs can be completed in as few as two years, limiting the time and financial commitment. Even with a shorter runway to retirement, the degree can boost your earning power and professional influence during those remaining working years.