Most important takeaways…
- A 7.2% national faculty vacancy rate turns away thousands of qualified NP applicants yearly.
- New federal loan limits effective July 2026 threaten NP enrollment and faculty supply.
- Unpaid clinical preceptor models create a hidden bottleneck restricting NP program capacity.
Employment of advanced-degree nurses is projected to increase by 35% from 2024 to 2034,1 yet thousands of qualified applicants are turned away from nurse practitioner programs each year. The constraint is not demand. It is educational capacity: not enough faculty, not enough clinical preceptors, and not enough seats in the classroom.
Nursing schools rejected more than 80,000 qualified applicants in recent cycles, even as primary care nurse practitioner shortages worsen across the country. The result is a growing workforce gap driven not by a lack of interest in the profession, but by structural limits on how many students schools can admit and train.
Those limits stem from a 7.2% national faculty vacancy rate,1 widespread clinical site shortages, and a federal student loan cap that took effect in July 2026. Together, they form a bottleneck that begins long before you step into a clinic as a licensed NP.
Why the NP Workforce Shortage Begins in the Classroom
The nurse practitioner shortage is not simply a clinical staffing problem: it begins in the classroom, where limited educational capacity silently restricts how many new NPs can enter the pipeline each year. Despite widespread acknowledgment of the problem, the full scope remains hidden because the organizations that collect nursing education data do not publicly release granular, NP-specific breakdowns.
The Hidden Data Gap in NP Education
National nursing surveys from the American Association of Colleges of Nursing (AACN) and the National Organization of Nurse Practitioner Faculties (NONPF) aggregate many programs together. NP-specific metrics such as the number of qualified applicants turned away, applicant-to-seat ratios for master's and DNP NP tracks, or enrollment trends isolated to adult-gerontology or other specialties are not typically disaggregated in public reports. This makes it difficult for prospective students, policymakers, and the profession to pinpoint exactly where classroom bottlenecks are tightest.
To find comparable information, you often have to go directly to the source:
- Contact individual NP programs: Admissions offices can sometimes share recent applicant and enrollment figures, though they may not track turnaway counts consistently.
- Review accreditation reports: Documents from the Commission on Collegiate Nursing Education (CCNE) or the Accreditation Commission for Education in Nursing (ACEN) may contain snapshot enrollment data for specific programs.
Where to Look for Workforce and Capacity Indicators
Even without a single dashboard, several public resources offer clues about the education-to-workforce pipeline. The nurse practitioner shortage is already acute in many states, and understanding the educational data behind it can help you make smarter decisions about where and when to apply.
- U.S. Bureau of Labor Statistics (BLS) Occupational Outlook Handbook: Provides broad employment projections for nurse practitioners, showing strong growth rates that signal sustained demand. While it does not reveal program capacity, it confirms the high demand that unmet seats should be filling.
- University websites and institutional research pages: Searching for "nurse practitioner program applicant statistics" or browsing enrollment dashboards on university sites can uncover local data points.
- Professional associations: The American Association of Nurse Practitioners (AANP) sometimes publishes state-level workforce reports that reference graduation trends.
- State nursing boards: Annual reports on advanced practice registered nurse licensure often include total graduates from in-state programs, giving a rough sense of educational output relative to population needs.
Why This Matters for Your Career Path
When classroom capacity is opaque, prospective NP students may apply to programs without a clear picture of how competitive admission is or which specialties have the longest waitlists. This information asymmetry can lead to misaligned expectations and missed opportunities, ultimately dampening the pipeline at the very point where it should be expanding. Understanding advanced practice nursing trends can also reveal which specialties face the steepest supply gaps, helping you prioritize applications strategically. By knowing where to look, you can make more informed decisions about where to apply and what specialty to pursue, while also advocating for greater transparency from nursing education leaders.
The Nursing Faculty Shortage and Its Outsized Impact on NP Programs
Clinical practice versus academic teaching: for a doctorally prepared nurse practitioner, this choice carries real financial consequences, and that gap sits at the heart of why nursing programs are struggling to fill their own faculty rosters.
A Vacancy Problem with a Doctoral Twist
According to the American Association of Colleges of Nursing, nursing programs across the country reported roughly 1,588 faculty vacancies in 2025, with an overall vacancy rate approaching 7.8 percent.1 What makes this especially difficult for NP programs is the credential requirement attached to those empty seats. More than 80 percent of nursing faculty vacancies require or prefer a doctoral degree.2 For bachelor's-level nursing programs, an experienced master's-prepared nurse can sometimes fill a gap. For NP programs, that flexibility largely disappears. You need faculty who hold advanced clinical expertise and, in most cases, a DNP or PhD in nursing to qualify.
The Salary Gap That Drives Clinicians Away from Teaching
The financial math does not favor academia. Doctorally prepared nursing faculty earn a national average of around $155,312 per year, while master's-prepared faculty average closer to $104,520.2 At first glance, the doctoral faculty figure sounds reasonable, but consider the alternative. The national median annual wage for advanced practice registered nurses in 2024 sits at approximately $129,480, and many clinical NPs in high-demand specialties or urban markets earn well above that.2 When a doctorally prepared NP weighs a faculty position against a clinical role, the academic path often means accepting lower pay in exchange for greater job demands, grant obligations, and administrative work. That trade-off is hard to sell, and the vacancy data shows it. If you are weighing those options yourself, a closer look at whether a DNP is worth it may help frame the decision.
A Bottleneck That Compounds Itself
The average age of doctorally prepared nursing faculty is 61.2 years, and earlier projections estimated that roughly a third of the nursing faculty workforce would reach retirement age within roughly a decade.2 That wave is arriving now. As experienced faculty retire, programs need doctoral-prepared replacements, but the pipeline of NPs willing to pursue academic careers is constrained by the very salary disparity described above. Fewer faculty means fewer seats for NP students. Fewer NP graduates means fewer candidates who might eventually return to teach. The cycle reinforces itself at every turn.
Recruiting and retaining qualified NP faculty is reported as a barrier to filling vacancies at nearly 70 percent of nursing schools surveyed. The shortage is not simply about numbers. It reflects a structural misalignment between what academic institutions can offer and what the clinical market demands.
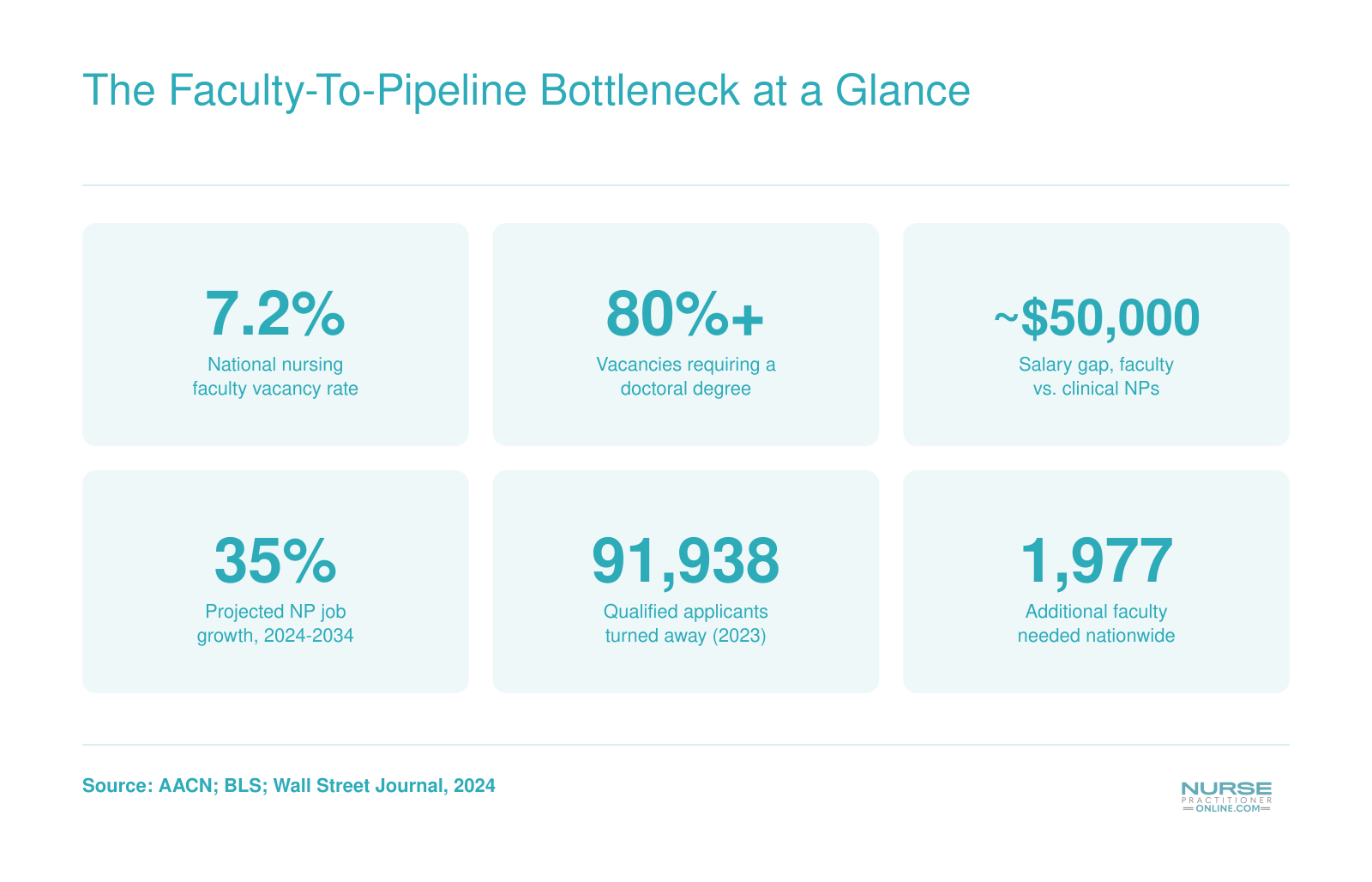
The Faculty-To-Pipeline Bottleneck at a Glance
A handful of figures tell the story of why thousands of qualified applicants never make it into NP programs each year. The bottleneck is not a lack of interest or talent. It is a shortage of faculty, clinical sites, and now potentially the financial support that keeps the education pipeline moving.
Clinical Preceptor Shortages: The Hidden Bottleneck for NP Students
Even if you secure a seat in an NP program with enough faculty to teach your courses, you may still face a less visible barrier: finding a qualified preceptor willing to supervise your clinical hours. For many students, this hidden bottleneck determines whether they graduate on time, delay their careers, or leave their program altogether.
What Preceptors Do and Why They Matter
Nurse practitioner education requires extensive hands-on training under the supervision of an experienced clinician. Depending on your specialty and state requirements, you will need to complete anywhere from 500 to over 1,000 supervised nurse practitioner clinical hours before you can graduate and sit for certification. Each of those hours requires a qualified preceptor at a clinical site who agrees to mentor you, review your patient encounters, and sign off on your competency.
Unlike your classroom instructors, most preceptors are practicing clinicians who volunteer their time. They receive little or no compensation for the extra work of teaching, evaluating, and documenting your progress. This creates a fundamental misalignment: the demand for preceptors keeps rising as NP programs expand enrollment, but the incentives for clinicians to take on students have not kept pace.
The Numbers Behind the Shortage
Recent data illustrates how tight the preceptor pipeline has become. In 2026, over 18,314 clinicians applied to serve as preceptors through major placement networks, yet only about 2,435 were actively matched with students, an acceptance rate of roughly 13.3 percent.2 That gap reflects both the administrative burden of vetting and placing preceptors and the limited capacity of clinical sites to absorb more learners.
The consequences are real for students. An estimated 28,000 NP students struggle each year to secure clinical placements,1 and nearly 4,856 program seats went unfilled in 2026 specifically because schools could not guarantee clinical rotations.2 A 2020 survey found that about 14 percent of NP students had to find their own preceptors, a stressful process that can add months to an already demanding program.3
Why Preceptor Shortages Differ from Faculty Shortages
Faculty shortages and preceptor shortages both constrain NP program capacity, but they stem from different root causes. Faculty positions are paid, tenure-track, or contract roles within academic institutions. Preceptorships, by contrast, are typically unpaid volunteer arrangements. A busy primary care NP or physician may want to give back through teaching, but the time required to supervise a student competes directly with patient care and productivity metrics. Without financial incentives or protected time, many clinicians simply cannot say yes. Understanding how much NP preceptors get paid helps explain why so few practicing clinicians volunteer for this role.
State-Level Variation in Preceptor Incentives
A handful of states have recognized this problem and created incentive programs to encourage more clinicians to precept. Virginia, for example, operates a Nursing Preceptor Incentive Program that offers stipends ranging from $500 to $5,000 per preceptor depending on hours contributed and program type.4 Other states have enacted tax credits for preceptors or allowed continuing education credits in exchange for clinical teaching.
However, most states still have no formal preceptor incentive programs. This creates geographic disparities: students in states with robust incentives may find placements more easily, while those in states without support face longer searches and fewer options. If you are evaluating NP programs, it is worth researching whether your state or your program offers any preceptor support, as this can directly affect your time to graduation.
NP Program Capacity by Specialty: Where the Squeeze Is Tightest
Not every nurse practitioner specialty faces the same enrollment crunch. Some tracks, like family nurse practitioner (FNP), have a large number of programs and seats, while highly specialized areas such as neonatal (NNP) or psychiatric mental health (PMHNP) may have far fewer slots and stiffer competition. Understanding where the squeeze is tightest helps you set realistic expectations and target programs where you actually have a shot.
Accessing National Enrollment Reports
The most reliable starting point for macro-level data is the American Association of Colleges of Nursing (AACN) annual enrollment and graduation reports. These break down NP programs by specialty track and degree level, giving you a bird's-eye view of how many students are entering and completing each specialty. Similarly, the National Organization of Nurse Practitioner Faculties (NONPF) conducts periodic surveys that capture program counts, faculty vacancies, and enrollment trends. Keep in mind that these reports often lag by a year or more, so they reflect the landscape rather than this year's real-time availability.
Finding Program-Level Capacity Information
Aggregate applicant-to-seat ratios and waitlist data are rarely published in one neat spreadsheet. To gauge the actual competitiveness of a specialty track, you'll need to dig into individual school websites or, better yet, contact admissions offices directly. Many programs openly state if they have a waitlist for certain specialties, but they may not advertise the number of qualified applicants turned away each cycle. A brief phone call or email can reveal whether a program is accepting only a handful of students into the PMHNP track or if their AGNP cohort is consistently under-enrolled. Faculty shortages and clinical placement constraints often force schools to cap enrollment at levels well below applicant demand, making this direct inquiry essential.
Tapping Specialty Organizations for Insights
Professional associations often have their finger on the pulse of workforce capacity. For neonatal NP programs, the National Association of Pediatric Nurse Practitioners (NAPNAP) may publish member surveys or white papers that touch on educational bottlenecks. Similarly, the International Society of Psychiatric-Mental Health Nurses (ISPN) is a resource for understanding PMHNP training constraints. These groups sometimes produce policy briefs that highlight faculty shortages, preceptor scarcity, or the uneven geographic distribution of programs, all of which affect how many students can be trained in a given year.
Comparing Demand with Graduation Rates
A useful, though rough, way to estimate specialty-specific supply gaps is to compare the Bureau of Labor Statistics (BLS) projected job growth for NPs with the number of graduates reported by AACN. If a specialty's demand is rising faster than the number of newly minted NPs, capacity constraints are likely at play. For example, if mental health care demand is surging but PMHNP graduation numbers are stagnant, you can infer that classroom and NP clinical rotations are limiting the pipeline. This exercise won't give you a precise seat count, but it can confirm whether your chosen specialty is among those where program capacity is stretched thinnest.
Related Articles
Proposed Federal Loan Limits: A New Threat to NP Education Access
Access versus affordability: that is the tension at the heart of a federal policy change that took effect July 1, 2026,1 and could reshape who gets to become a nurse practitioner in the years ahead.
What Changed and When
For the 2026-2027 academic year, graduate nursing students relying on federal Direct Unsubsidized loans and Grad PLUS loans now face a hard ceiling: $20,500 per year in Direct Unsubsidized borrowing, with an aggregate cap of $100,000 across a degree program.2 That sounds like a large number until you compare it to the treatment graduate nursing programs are receiving relative to other professional degrees. Programs classified as professional degrees carry a much higher annual cap of $50,000 and an aggregate ceiling of $200,000.2 Graduate nursing programs were explicitly excluded from that professional degree classification,3 leaving NP students with roughly 40 cents of federal borrowing capacity for every dollar available to students in other health professions programs of comparable cost and complexity.
The policy is currently subject to ongoing litigation,4 so its long-term shape remains uncertain. But as of this writing, the caps are in force, and students enrolling now are planning budgets around them.
Who Bears the Cost
The gap between what federal loans now cover and what many NP programs actually cost falls hardest on students who have no other source of funding to bridge it. Nurses from lower-income backgrounds, career changers without significant savings, and working clinicians who cannot take on private loans at unfavorable terms face a real enrollment barrier that did not exist before. A WSJ opinion piece on this issue made the point plainly: the author began her career as a registered nurse, advanced to NP practice, and eventually moved into nursing education, all made possible by federal student loans. Restrict that pipeline and you do not just reduce the number of future NPs; you reduce the number of people who will one day staff nursing school faculty positions. If you are weighing your options for how to pay for NP school, the current landscape makes it worth exploring every scholarship, employer reimbursement, and loan repayment avenue available.
The Faculty Ripple Effect
The connection to faculty supply is direct and underappreciated. With more than 80% of nursing faculty vacancies requiring or preferring a doctoral degree, the pathway from bedside nurse to NP to educator depends on sustained access to graduate-level financing. Understanding nurse practitioner loan forgiveness programs matters more than ever for anyone trying to close the gap between program costs and federal borrowing limits. A policy that makes the NP step harder to reach also makes the educator step harder to reach. The downstream result is fewer faculty to train the next cohort, compounding a shortage that is already limiting how many qualified NP applicants programs can admit each year.
The Counterargument, Taken Seriously
Proponents of loan caps argue that unlimited federal borrowing has allowed graduate programs to raise tuition without accountability, and there is real evidence supporting that concern across higher education broadly. Controlling costs in graduate professional programs is a legitimate policy goal. The problem is that nursing sits in a different position than, say, an MBA program. NP graduates move into primary care roles in underserved communities, rural health systems, and public health settings where salaries, while solid, do not reflect the earnings trajectory of law or finance. Policies designed to discipline high-cost, high-return degrees apply blunt pressure to a field where the return is measured in patient access as much as personal income. The AACN and other nursing organizations have published guidance and public statements raising precisely this concern,3 and federal court proceedings around the rule suggest the legal and policy debate is far from settled.4
Questions to Ask Yourself
Online Vs. On-Campus NP Programs: Does Format Solve the Capacity Problem?
On-campus study offers face-to-face mentorship and built-in clinical networks, while online NP programs promise flexibility and the ability to keep working. Many nurses assume that shifting a program online automatically expands capacity, but the reality is more complex.
How Online Programs Expand Access
Online and hybrid formats have been a game-changer for geographic reach and scheduling. A nurse in a rural community can enroll in a top-tier program hundreds of miles away without relocating, continuing to work full-time while completing didactic coursework asynchronously. Schools can accept larger cohorts because they are not limited by physical classroom seats. This model has significantly boosted total NP enrollment over the past decade and opened doors for nurses who could never have paused their lives for a traditional on-campus program.
The Clinical Preceptor Bottleneck Remains
Didactic capacity is only half the picture. Every NP student must complete hundreds of clinical hours under a qualified preceptor, and those hours happen in real clinical settings, not online. An online program's geographic flexibility does not create new preceptors in the student's local area. The same shortage of willing clinical sites and preceptors, especially in primary care and rural settings, applies regardless of how the lecture content is delivered. In practice, many online students face long delays securing nurse practitioner clinical placements, and some programs put the burden of finding a preceptor entirely on the student.
Accreditation Standards Keep Ratios Tight
Accrediting bodies such as CCNE and ACEN apply the same quality standards to every delivery format.1 A key constraint is the maximum faculty-to-student ratio, often set at 1:8 for clinical supervision.2 This cap is not relaxed for online programs. While no numeric preceptor-to-student ratio is mandated universally,2 the practical limit of how many students one preceptor can responsibly mentor creates a natural ceiling. Schools that rapidly scale online enrollment without a proportional increase in clinical faculty or preceptor partnerships quickly run into compliance risk.
The Nuance: Growth Without Solving the Core Problem
Online education has undeniably expanded access to NP coursework, but it shifts the bottleneck rather than removing it. Instead of a classroom seat shortage, the constraint becomes a clinical placement shortage, one that is harder to solve with technology. Some states have tightened oversight of online vs. on-campus NP programs precisely because of concerns about clinical quality and faculty workload, adding another layer of friction. For aspiring NPs, the program format matters less than whether the school can guarantee a high-quality clinical rotation in your area.
Solutions: How Schools, Policymakers, and Students Can Expand NP Capacity
Expanding NP capacity means addressing three separate bottlenecks (faculty, clinical placements, and funding) at three different levels: what Washington and state legislatures do, what schools do internally, and what you as a prospective student can control. No single fix solves the pipeline problem, but each tier has levers worth pulling.
Policy Levers: What Needs to Happen at the Federal and State Level
The most direct policy fix is sustained investment in nursing workforce programs. Title VIII of the Public Health Service Act funds advanced nursing education, faculty loan repayment, and workforce diversity initiatives, and consistent increases to that appropriation would meaningfully expand the doctoral-prepared faculty pool that NP programs depend on.
- Preceptor incentives: Federal or state tax credits and stipends for practicing NPs and physicians who precept students would ease the placement crunch. A handful of states (Georgia, Maryland, Colorado) already offer preceptor tax credits, and expanding the model nationally would help.
- Faculty loan forgiveness: Targeted loan forgiveness for NPs who commit to a defined number of teaching years addresses the pay gap that currently pushes doctoral-prepared nurses away from academia.
- Protecting graduate loan access: Proposed caps on federal graduate borrowing would hit advanced nursing degrees hard. Advocacy through professional organizations matters here, and understanding how to pay for NP school is increasingly important for prospective students weighing their options.
Institutional Innovations: What Schools Can Do Now
Schools do not have to wait for policy to change. Joint clinical-academic appointments let experienced NPs teach part-time while continuing to see patients, preserving their income and keeping their clinical skills sharp. Smaller programs are increasingly forming shared faculty consortia, pooling specialty instructors across institutions so one adult-gerontology expert can teach across three schools.
High-fidelity simulation is the other lever. Well-designed simulation hours (validated in recent research to be interchangeable with a portion of traditional clinical hours) reduce the raw preceptor demand per student without compromising competency. Whether paid NP preceptors or volunteer clinical supervisors fill remaining slots, reducing the total hours required per student makes both models more sustainable.
Student Strategies: What You Can Control
You cannot fix the faculty shortage, but you can navigate around it.
- Consider less-saturated specialties: Adult-gerontology primary care and psychiatric-mental health programs often have shorter waitlists than family NP tracks.
- Look outside coastal metros: Programs in the Midwest, Mountain West, and rural Southeast frequently have more open seats and established regional preceptor networks.
- Time your application: Many programs run one or two cohorts per year. Applying 9 to 12 months out gives you room to compare offers instead of accepting the first available seat.
- Ask about preceptor support: Programs that place students (rather than requiring you to find your own) dramatically reduce your risk of a delayed graduation.
Every qualified nurse practitioner faculty member turned away from the classroom today means dozens of NP students who cannot enroll tomorrow, and hundreds of patients left without primary care providers for years to come.
What NP Program Capacity Constraints Mean for Your Career Path
The same bottleneck that makes getting into an NP program so frustrating also creates powerful leverage once you graduate. When qualified applicants are turned away year after year, the supply of new nurse practitioners stays below what the labor market actually needs, and that imbalance translates directly into stronger job offers, better negotiating power, and rising compensation for those who do earn their credentials.
A Bottleneck That Rewards Those Who Get Through
With employment of advanced-degree nurses projected to increase 35 percent from 2024 to 2034,1 demand for NPs is not softening anytime soon. Every year that programs cannot expand fast enough to meet that demand, the gap between supply and need widens further. For graduates entering practice, this means shorter job searches, signing bonuses in underserved areas, and salaries that continue to climb. The constraint is real, but it cuts both ways.
How to Evaluate a Program Before You Commit
Not every NP program manages its capacity responsibly. Before you enroll, ask pointed questions so you are not stuck scrambling for a clinical placement that the school cannot deliver. how to evaluate FNP programs is a useful starting point for building your checklist.
- Preceptor placement rate: Ask what percentage of students secure clinical sites within the expected timeline. Programs that consistently place above 90 percent likely have established site agreements rather than leaving students to find their own.
- Faculty-to-student ratio in clinical courses: A ratio above 1:10 in clinical supervision is a signal worth investigating. Ask whether clinical faculty are full-time or adjunct, and how many sections each instructor oversees.
- Time-to-degree data: If most students take a semester or more beyond the published timeline, overcrowded clinical rotations are often the reason. Request the school's actual completion rate by cohort.
- Red flags: Programs that require you to find your own preceptor with no institutional support, or that admit large cohorts while listing multiple open faculty positions, deserve extra scrutiny.
Navigating the Waitlist Reality
If you are waitlisted, know that typical wait times range from one semester to a full academic year at competitive programs, particularly in specialties like psychiatric-mental health and adult-gerontology primary care. Reapplying to the same program can improve your odds if you strengthen your application in specific ways the admissions committee flags, but do not count on loyalty alone. Applying to two or three programs simultaneously is almost always worth the additional application fees when weighed against the cost of sitting out another year. Reviewing MSN NP program mistakes to avoid before you reapply can sharpen your next submission.
Think of This as a Career Skill, Not a One-Time Hurdle
The faculty shortage, clinical preceptor limitations, and policy threats to student loan access are structural problems that will persist for years. Learning to navigate them, by choosing programs wisely, finding NP clinical preceptors early, and staying informed about policy changes, is not just a task you complete once during admissions season. It is a skill set that will serve you throughout your career as you pursue post-graduate certificates, doctoral education, or faculty roles of your own. The nurses who plan around these constraints, rather than simply waiting for them to resolve, are the ones who move forward.
Frequently Asked Questions About NP Program Capacity
Capacity constraints in nurse practitioner programs affect aspiring NPs at every stage, from application to graduation. Below are answers to the questions we hear most often from working nurses exploring advanced practice education.
- Is there an NP shortage in the United States?
- Yes. Demand for nurse practitioners continues to outpace supply, particularly in primary care and rural settings. The Bureau of Labor Statistics projects employment of advanced degree nurses to increase by 35% from 2024 to 2034. However, NP program capacity has not kept pace with this demand, meaning the pipeline of new graduates falls short of what clinics, hospitals, and communities need.
- How many qualified applicants are turned away from NP programs each year?
- While a single national figure for NP programs specifically is difficult to pin down, nursing schools across all degree levels turn away tens of thousands of qualified applicants annually. The primary reasons are insufficient faculty, limited clinical placement sites, and constrained classroom or lab space. For NP programs in high demand specialties, rejection rates can be especially steep.
- Why is there a nursing faculty shortage and how does it affect NP programs?
- Nursing schools face a 7.2% national faculty vacancy rate, and more than 80% of those openings require or prefer a doctoral degree. Because NP courses demand faculty with advanced clinical expertise, these vacancies hit graduate programs hard. Fewer faculty members means fewer sections offered, smaller cohort sizes, and ultimately fewer NP graduates entering the workforce each year.
- Which NP specialties have the longest waitlists or most limited capacity?
- Psychiatric mental health and adult gerontology primary care NP programs tend to face the tightest capacity constraints. These specialties contend with both high applicant demand and a limited pool of qualified faculty and clinical preceptors. Programs in rural or underserved regions may have even fewer available seats due to a smaller network of clinical training sites.
- How could proposed federal student loan limits affect NP education?
- The Education Department has proposed new limits on federal student loans for advanced nursing degrees. If enacted, these caps could make NP programs financially out of reach for many working nurses, particularly those without employer tuition support. Reduced enrollment would also shrink the future pool of doctorally prepared faculty, compounding the capacity problem for years to come.
- Do online NP programs have more available seats than on campus programs?
- Online programs can often enroll larger didactic cohorts because they are not limited by physical classroom space. However, every NP student still needs hands on clinical hours with a qualified preceptor, and that requirement creates the same bottleneck regardless of program format. Online programs may ease one constraint, but they do not fully solve the capacity shortage on their own.