Most important takeaways…
- NPs start earning a full salary five to eight years before physicians, significantly narrowing the lifetime income gap.
- Twenty-eight states and D.C. now grant nurse practitioners full practice authority with no physician oversight requirement.
- BLS projects NP employment to grow 40 percent from 2024 to 2034, far outpacing physician job growth.
- Research in JAMA Internal Medicine found NP patient outcomes comparable to or better than physician outcomes across 11 measures.
Nurse practitioners now deliver more than one billion patient visits each year in the United States, most of them in primary care settings where patients once expected to see a physician. That shift has made "what's the difference between a nurse practitioner and a doctor?" one of the most frequently asked questions among working nurses considering career advancement and patients trying to understand who's treating them.
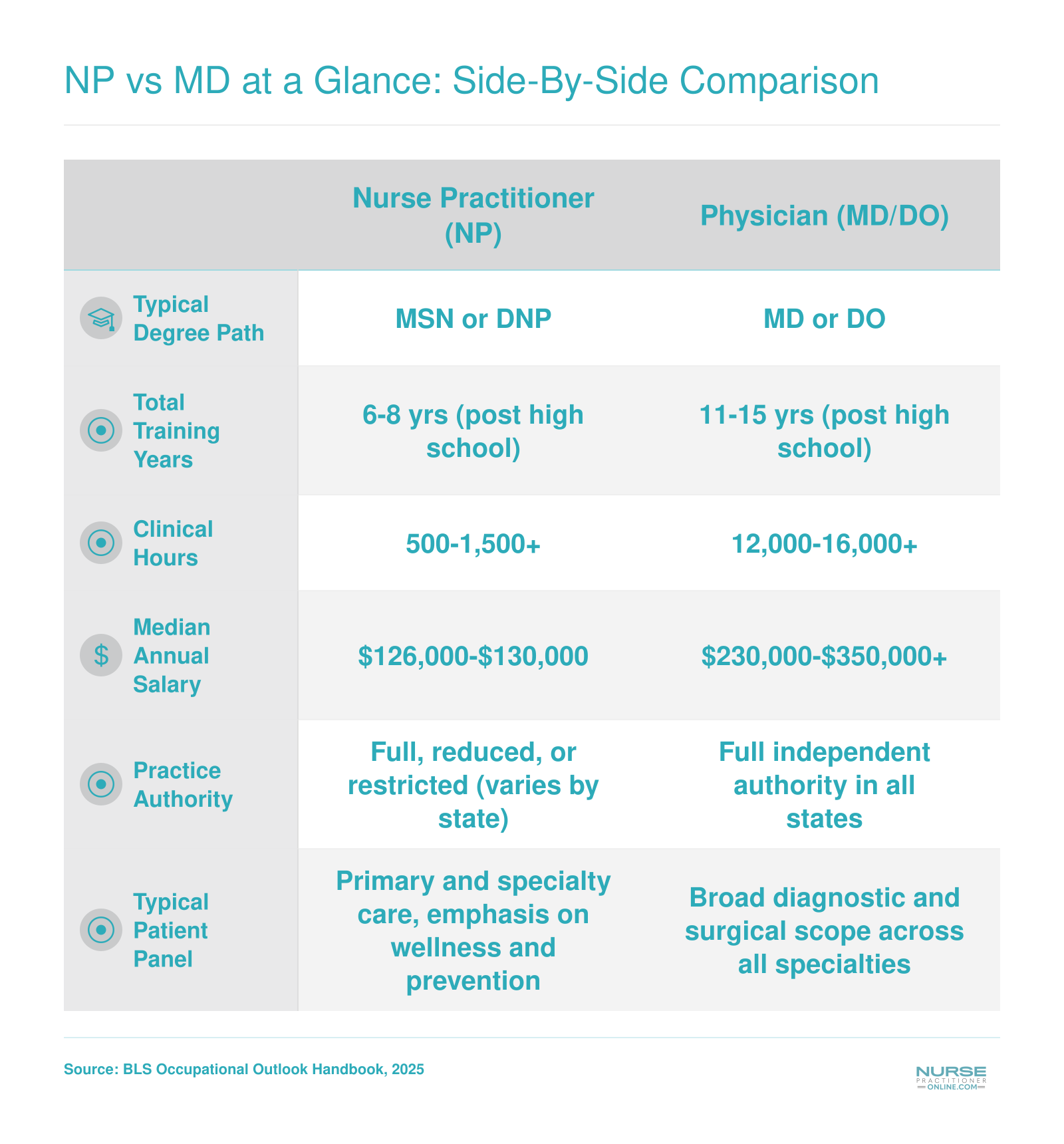
The gap separates at every decision point: education length, clinical training hours, prescriptive authority, salary, debt load, and practice independence. Nurse practitioners complete MSN or DNP programs in two to four years after their BSN, accumulate around 700 supervised clinical hours, and start earning full salaries in their early thirties. Physicians spend four years in medical school, three to seven years in residency, log 15,000 to 20,000 clinical hours, and often don't finish training until their mid-thirties, carrying six-figure debt.
Twenty-eight states now grant NPs full practice authority. In those markets, the scope question matters less than specialty, setting, and whether you want to own your timeline or maximize clinical depth.
NP vs MD at a Glance: Side-By-Side Comparison
Before diving into the details, here is a quick-scan summary of how nurse practitioners and physicians compare across the attributes that matter most to working nurses weighing their next career move.
Education and Training: Timeline, Hours, and Cost
The gap between becoming a nurse practitioner and becoming a physician is not just a matter of years. It involves fundamentally different training philosophies, financial commitments, and clinical hour requirements that shape how each provider practices.
How Long Each Path Takes
Most registered nurses complete an MSN-level NP program in two to three years of post-bachelor's study, or three to four years if they pursue a DNP. Nurses considering the doctoral route should review DNP prerequisites early so they can plan accordingly. Add the time to earn a BSN and you are typically looking at six to eight years of education in total. The physician path is longer by a substantial margin. A four-year medical school degree is followed by residency training that runs three years at minimum for primary care specialties and up to seven or more years for surgical fields. Many physicians also complete fellowships after residency. From the first day of college to independent practice, the timeline commonly reaches eleven to fifteen years.
Clinical Hours: What the Numbers Mean
NP programs accredited through the CCNE or ACEN typically require somewhere between 500 and 750 supervised clinical hours for MSN graduates, while DNP programs generally push that figure above 1,000 hours. Those numbers are program-specific, so contacting admissions offices directly is the most reliable way to confirm what a particular school requires. For a closer look at what those hours actually involve, our guide to nurse practitioner clinical rotations walks through the student experience in detail.
Physician residency hours are a different order of magnitude. The ACGME caps residents at 80 hours per week, and a three-year residency alone accounts for roughly 12,000 to 15,000 clinical hours. Surgeons and specialists who train for five to seven years accumulate far more. The comparison is worth understanding clearly: NPs and physicians are trained for overlapping but distinct scopes of practice, and the hour difference reflects that design rather than a deficiency on either side.
The Cost Difference
The financial picture diverges sharply here. Medical school graduates carry median debt well above $200,000 according to AAMC annual reports, with many graduates exceeding $300,000 when living expenses are factored in. NP graduates face a much lighter burden. AACN surveys and Education Data Initiative data consistently place median graduate nursing program debt in a range far below that of medical school, often under $50,000 for MSN completers, though DNP costs can run higher depending on the program and whether the student attends part-time while working.
That debt gap has real implications for long-term financial wellbeing, especially when you weigh it against the salary differential between NPs and physicians. The lifetime earnings comparison later in this article addresses that tradeoff directly.
Questions to Ask Yourself
Scope of Practice and Prescriptive Authority
Twenty-eight states and the District of Columbia now grant nurse practitioners full practice authority, allowing them to evaluate patients, diagnose conditions, initiate treatment plans, and prescribe medications, including controlled substances, without physician oversight. Understanding what each role is authorized to do, and where those boundaries shift, is essential if you are weighing the NP path against the MD route.
What NPs Are Authorized to Do
Nurse practitioners hold a broad clinical scope that includes:
- Diagnosing and treating: NPs assess patients, order and interpret labs, imaging, and other diagnostics, and manage acute and chronic conditions across the lifespan.
- Prescribing medications: In the vast majority of states, NPs prescribe Schedule II through V controlled substances. A handful of states still require a collaborative or supervisory agreement with a physician before an NP can prescribe certain drug classes.
- Specialty-specific care: Scope also depends on an NP's population focus and certification. A family nurse practitioner manages different clinical situations than a psychiatric-mental health NP or an acute care NP, and each certification carries its own practice boundaries.
In full practice authority states, an NP working in primary care handles day-to-day patient encounters in much the same way a physician does: conducting physicals, managing diabetes or hypertension, adjusting medications, and referring to specialists when needed.
Where MD Authority Differs
Physicians hold unrestricted clinical privileges in every state. That means no collaborative agreement is ever required, and their scope of practice extends to areas NPs generally do not enter:
- Independent performance of complex surgical procedures
- Certain invasive interventions such as cardiac catheterizations or neurosurgical operations
- Unrestricted prescriptive authority nationwide, regardless of state-level practice environment laws
These distinctions matter most in acute, high-acuity, or surgical settings. In outpatient primary care and many specialty clinics, the practical overlap between what an NP does and what a physician does is substantial.
Can a Nurse Practitioner Do Everything a Doctor Can?
The honest answer is: it depends on the setting, the state, and the clinical situation. In a full practice authority state, a primary care NP and a primary care physician may manage virtually identical patient panels with similar outcomes. Research consistently supports comparable quality of care for the conditions NPs are trained to treat.
However, there are clear limits. NPs are not trained or licensed to perform independent surgical procedures, and in reduced or restricted practice states, they may need a physician co-signature on treatment plans or prescriptions. The distinction is not about capability alone; it reflects differences in training depth, legal frameworks, and the complexity of the clinical scenario.
For nurses considering an NP career, this nuance is actually good news. The scope is wide enough to offer genuine clinical autonomy in most practice environments, especially in primary care, while the collaborative structures in some states can serve as a built-in safety net early in your career. If you are just starting out, you may also find practical wisdom in advice from those who have walked the path before, such as insights on being a new nurse practitioner.
NP Practice Authority by State: Full, Reduced, and Restricted
Where you practice as a nurse practitioner matters just as much as what you practice. State laws determine how independently you can evaluate patients, diagnose conditions, and prescribe medications, and those laws vary widely across the country. Understanding these differences is essential if you are weighing an NP career against a medical degree, because practice authority shapes your day-to-day autonomy, earning potential, and job satisfaction.
As of May 2026, every U.S. state falls into one of three categories defined by the American Association of Nurse Practitioners.1
Full Practice Authority (23 States)
In full practice authority states, NPs can evaluate patients, diagnose, order and interpret diagnostic tests, and prescribe medications (including controlled substances) without any physician oversight.2 This is the closest an NP's clinical autonomy comes to that of a physician.
Examples include Alaska, Arizona, Colorado, Connecticut, and Delaware.3 Over the past decade the trend has moved steadily in this direction, with several states upgrading their practice environments in response to primary care shortages and pandemic-era workforce demands.
If independent practice is a top priority for you, targeting your job search or even your state of residence toward these states can make a significant difference in how you experience the NP role.
Reduced Practice Authority (16 States)
Reduced practice states require some form of collaborative agreement with a physician, though NPs still carry substantial clinical responsibility. The specifics vary: some states mandate a written agreement on file, while others require periodic chart reviews or co-signatures on certain prescriptions.
Representative states in this category include Alabama, Arkansas, Illinois, Indiana, and Kentucky. Collaborative agreements add an administrative layer but rarely prevent NPs from caring for patients effectively. Many NPs in these states describe the arrangement as more of a formality than a true clinical limitation.
Restricted Practice Authority (11 States)
In restricted states, NPs must work under direct physician supervision for at least one element of their practice, whether that involves prescribing, diagnosing, or both. California, Florida, Georgia, Michigan, and Missouri are among the states in this tier.5
Restricted environments can limit where and how you practice, particularly in rural or underserved areas where supervising physicians may be hard to find. That said, legislative efforts in several of these states are actively pushing toward expanded authority, so the landscape continues to evolve. For a deeper look at those legislative trends, see our guide on the evolving role of nurse practitioners.
Why This Matters for the NP vs MD Decision
If you are comparing the NP and physician paths, practice authority is one of the most practical differences to weigh. In a full practice authority state, an NP functions with a level of independence that narrows the gap considerably. In a restricted state, the day-to-day experience looks more like a physician-dependent model. Our ranking of the best states for nurse practitioners can help you identify where these advantages are strongest.
- Career flexibility: Full practice authority states offer more options for opening your own clinic or working in telehealth across state lines.
- Rural impact: States with shortages often grant broader NP authority, creating opportunities to serve communities that need care most.
- Legislation trends: The number of full practice authority states has grown steadily, suggesting that NP autonomy will continue to expand nationwide.
Before choosing a program or committing to a state, check the latest practice environment map from the American Association of Nurse Practitioners.1 Laws can change between legislative sessions, and staying current ensures you make an informed decision about where your NP career will take you.
Related Articles
Salary Comparison: NP vs MD by Specialty and State
Compensation is one of the most frequently discussed differences between nurse practitioners and physicians. The table below draws on the latest national wage estimates to show how NP earnings compare with those of physicians across several occupational categories. Keep in mind that physician salary data at the upper end is often suppressed because it exceeds reportable thresholds, so the figures shown here represent conservative benchmarks.
| Occupation | Total Employed | Mean Annual Salary | 25th Percentile | Median Salary | 75th Percentile |
|---|---|---|---|---|---|
| Nurse Practitioners | 307,390 | $132,000 | $109,940 | $129,210 | $149,570 |
| General Internal Medicine Physicians | 66,640 | $262,710 | $135,240 | $236,350 | N/A |
| Physicians, All Other | 315,360 | $253,470 | $95,080 | N/A | N/A |
| Physicians (All Categories) | 727,050 | $272,320 | $138,460 | N/A | N/A |
NP vs Physician Salary: Highest-Paying States
Geography plays a major role in how much nurse practitioners and physicians earn. The table below compares median annual wages for NPs and physicians across states where both occupations report high compensation. NP figures reflect all specialties combined, while physician figures draw from general internal medicine and other physician categories, based on the latest federal occupational wage data.
| State | NP Median Salary | Physician Median Salary (Internal Medicine) | Physician Median Salary (All Other) |
|---|---|---|---|
| California | $166,610 | N/A | N/A |
| New Jersey | $149,620 | $155,570 | $238,870 |
| New York | $145,390 | $173,340 | $237,710 |
| Alaska | $145,450 | N/A | N/A |
| Oregon | $144,600 | N/A | N/A |
| Washington | $140,220 | N/A | N/A |
| Connecticut | $138,960 | $214,190 | $227,720 |
| Massachusetts | $138,890 | N/A | $216,170 |
| New Mexico | $138,440 | N/A | N/A |
| Arizona | $133,790 | N/A | $223,680 |
| Rhode Island | $130,710 | $223,340 | $229,340 |
| District of Columbia | $131,380 | $209,250 | N/A |
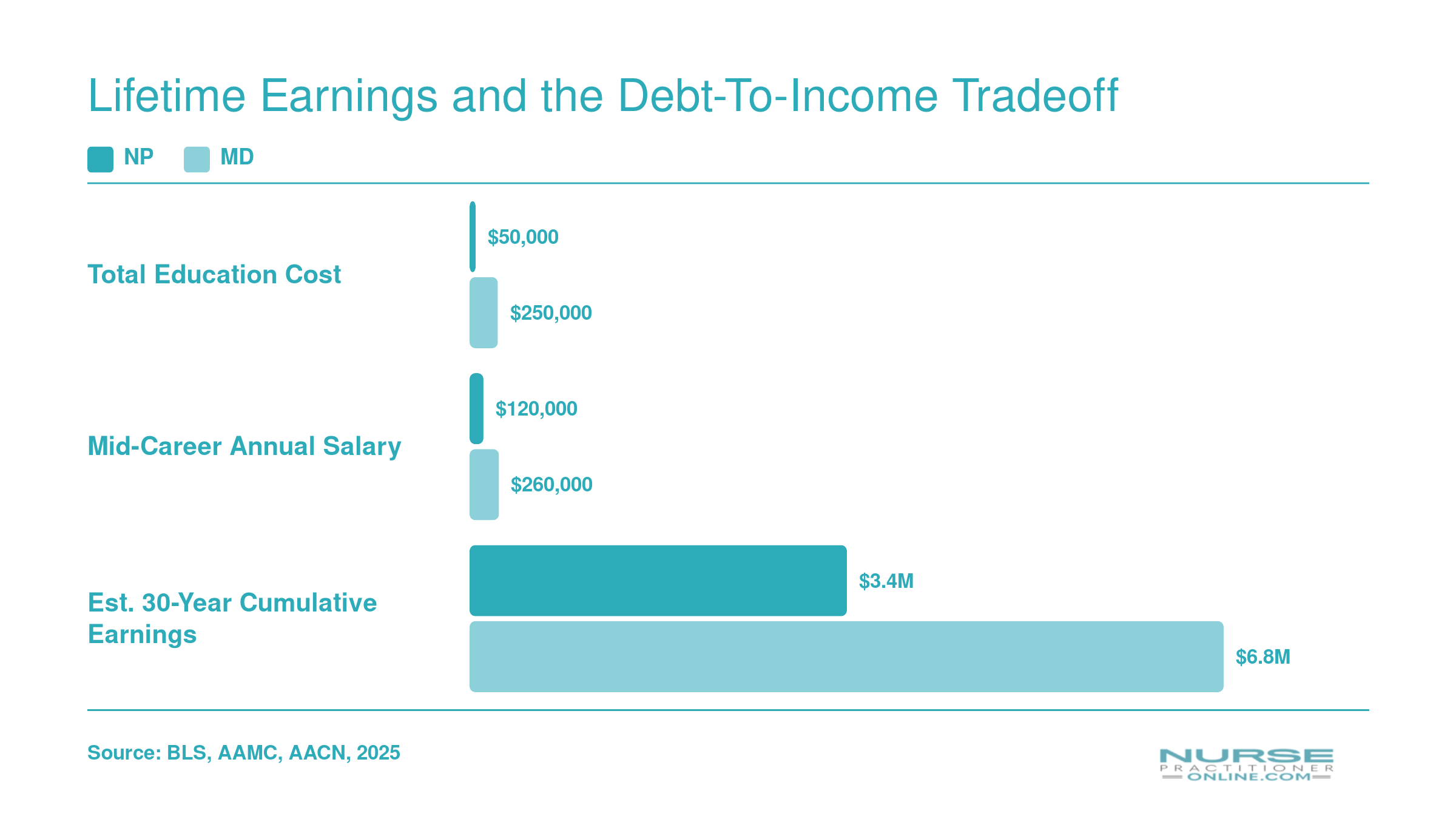
Lifetime Earnings and the Debt-To-Income Tradeoff
Higher physician salaries come with a steep upfront cost: longer training, delayed earning years, and significantly more debt. When you map out a full 30-year career, the financial picture is more nuanced than annual salary alone suggests. The gap between NPs and MDs narrows considerably in primary care specialties, while it widens in surgical and procedural fields where physician reimbursement is highest.
Career Outlook, Job Growth, and Demand
Nurse practitioner is one of the fastest-growing careers in the United States, and the gap between NP and physician demand has never been wider. The Bureau of Labor Statistics projects employment of nurse practitioners to grow 40% from 2024 to 2034, compared with just 3% growth for physicians and surgeons over the same period.12 For context, the average growth rate across all occupations sits around 4%, which means NP job creation is outpacing the broader labor market roughly tenfold.
Why Demand Is Surging
Several forces are converging to fuel NP hiring. The Association of American Medical Colleges has been warning for years about a worsening physician shortage, particularly in primary care, with rural and underserved communities feeling it first. At the same time, the U.S. population over age 65 keeps expanding, driving more chronic disease management, more medication reviews, and more routine visits than the physician pipeline can absorb.
State policy is the third lever. As more states grant full practice authority, NPs can independently open clinics, run telehealth practices, and staff retail and urgent care sites that physicians alone cannot cover. Health systems have responded by building care teams around NPs rather than waiting on a shrinking physician supply. The shortage is especially acute in rural settings, where nurse practitioners in rural healthcare are increasingly the primary point of access for patients.
Where the Jobs Are Concentrated
Demand is not evenly distributed across specialties. The tightest physician shortages, and therefore the strongest NP hiring, cluster in:
- Primary care (family practice, internal medicine)
- Psychiatric and mental health care, where wait times for patients can stretch months
- Geriatrics and long-term care
- Rural and federally designated shortage areas
If you are choosing a specialty with employability in mind, these four categories consistently top employer demand surveys. You can also weigh earning potential by reviewing NP specialties by salary to find the intersection of high demand and strong compensation. For a geographic perspective, our breakdown of states with most need for nurse practitioners highlights where openings are most plentiful.
Hours and Burnout: A Quieter Advantage
Workload differences also shape the long-term picture. NPs typically report working 40 to 45 hours per week, while physicians, especially in hospital-based and surgical specialties, often log 50 to 60 hours or more. Medscape's annual burnout reporting consistently finds physician burnout rates near or above 50%, with NPs reporting meaningfully lower rates. Combine that with a hiring market projected to add hundreds of thousands of NP roles this decade, and the career outlook side of the NP vs MD comparison tilts noticeably toward the NP path.
Patient Outcomes and Quality of Care: What the Research Shows
Skeptics often frame the NP vs MD question as a quality tradeoff, while two decades of outcomes research frame it as a question of care model fit. The evidence, when you actually pull it up, lands much closer to equivalence than most patients (or hiring committees) assume.
What the Systematic Reviews Found
A systematic review published by the American College of Physicians examined NP-led primary care across multiple outcome categories and found care quality comparable to physician-led care, with patient satisfaction equal to or higher for NP patients.1 A separate systematic review in a Wiley nursing journal compared experiences and outcomes between NPs and physicians for adult primary care patients in the United States and reached similar conclusions: mortality was equivalent, hospital readmission rates were similar, and serious adverse events occurred at equivalent rates between the two provider types.23
The McMaster Health Forum's review, examining NPs through the Quadruple Aim framework, reinforced the pattern.4 NP-led care showed:
- Hospitalizations: Reductions of roughly 35% in some patient populations compared with usual care models.
- Chronic disease management: Outcomes for diabetes, hypertension, and similar conditions were better than or equivalent to physician-led care.
- Guideline adherence: NPs demonstrated greater adherence to evidence-based clinical guidelines in several studies.
- Cost and ED use: Care costs were similar or lower, and emergency department utilization showed no meaningful difference.
Is an NP or MD Better for Primary Care?
For routine primary care and chronic disease management, the honest answer is that the research supports equivalence. Patients seeing an NP as primary care provider report satisfaction levels that match or exceed those reported by patients seeing physicians, particularly on measures of time spent, listening, and education. That is the question most working adults are really asking when they choose a provider, and the data answers it clearly.
Where the Evidence Thins Out
A few honest caveats matter. The bulk of comparative outcomes research focuses on primary care and outpatient chronic disease management. Evidence is thinner for NPs working in acute care, complex surgical comanagement, and high-acuity specialty settings, where physician training depth and procedural volume carry weight the research has not yet fully measured. Patient complexity also varies between practices, and head-to-head studies cannot always control for it perfectly. For nurses weighing the NP path and thinking about how to build an NP-led care team, the outcomes case for your future practice in primary care is already well established.
A 2013 systematic review published in JAMA Internal Medicine found that nurse practitioner care was comparable to or better than physician care across all 11 clinical outcomes examined, with NPs actually achieving better results for patient serum lipid levels. This adds to a growing body of evidence supporting the quality of NP-delivered primary care.
Which Path Is Right for You? NP vs MD Decision Framework
Choosing between the NP and MD path comes down to how you want to balance training time, financial investment, clinical scope, and quality of life. Neither route is universally better. The right answer depends on your career goals, family obligations, and appetite for risk. Use the pros and cons below to frame your decision.
Pros
- NP training typically takes 2 to 4 years after your BSN, letting you start earning sooner and with far less student debt.
- Average NP student debt is significantly lower than the $200K or more that most medical school graduates carry at graduation.
- NPs enjoy strong projected job growth through 2032, driven by primary care shortages and expanding telehealth services.
- In full practice authority states, NPs can diagnose, treat, and prescribe independently, offering meaningful clinical autonomy.
- NP schedules tend to be more predictable, supporting better work-life balance compared to physician residency and attending schedules.
- MDs have the broadest scope of practice with unrestricted prescriptive and procedural authority in every state.
- Physicians benefit from a higher lifetime earning ceiling, especially in surgical and procedural specialties.
- The MD path provides deeper specialist training through residency and fellowship, opening doors to highly specialized care roles.
- Physician credentials carry wide public recognition and professional prestige that can influence career mobility.
Cons
- NP autonomy varies significantly by state. In restricted practice states, NPs must maintain a collaborative agreement with a physician.
- NPs generally face a lower salary ceiling than physicians, particularly when compared to surgical or subspecialty MDs.
- Some patients and colleagues may question NP qualifications, creating perception challenges in certain practice settings.
- NPs have fewer opportunities to perform complex procedures, which can limit scope in hospital or surgical environments.
- The MD training pipeline spans 11 to 15 years (undergraduate, medical school, residency, and possible fellowship), delaying independent practice.
- Medical school debt frequently exceeds $200,000, and interest accrual during training years can push totals even higher.
- Physicians report higher burnout rates, partly due to longer, less predictable work hours and administrative burden.
- Residency and early attending years often demand 60 to 80 hour workweeks, making work-life balance difficult to sustain.
Frequently Asked Questions: NP vs MD
Choosing between the nurse practitioner and physician paths raises a lot of practical questions. Below are direct answers to the most common ones working nurses ask when weighing NP vs MD career options.
- What is the difference between a nurse practitioner and a doctor?
- A nurse practitioner (NP) is an advanced practice registered nurse who holds a master's or doctoral nursing degree and follows a nursing model of care centered on holistic, patient-focused practice. A doctor (MD or DO) completes medical school and residency training under a biomedical disease model. Both can diagnose, treat, and prescribe, but their educational paths, philosophical frameworks, and regulatory structures differ significantly.
- Can a nurse practitioner do everything a doctor can?
- In many clinical settings, NPs perform the same day-to-day tasks as physicians, including ordering tests, diagnosing conditions, and managing treatment plans. However, certain complex surgical procedures and some subspecialty interventions remain outside NP scope. In states with reduced or restricted practice authority, NPs may also need a collaborating physician agreement, which can limit independent decision-making.
- How many training hours do NPs have compared to MDs?
- NPs typically accumulate around 4,000 to 5,000 total clinical training hours across their RN experience and graduate program. MDs complete roughly 12,000 to 16,000 clinical hours through medical school clerkships and residency. The gap is real, though NPs often enter graduate education with years of hands-on bedside nursing experience that adds meaningful clinical knowledge not always reflected in hour-for-hour comparisons.
- Do nurse practitioners have full practice authority in every state?
- No. As of 2026, roughly half of U.S. states plus the District of Columbia grant NPs full practice authority, allowing them to evaluate, diagnose, prescribe, and manage patients independently. The remaining states impose either reduced authority (requiring a collaborative agreement) or restricted authority (mandating direct physician supervision). Legislation continues to evolve, with several states actively considering expanded NP autonomy.
- Is an NP or MD better for primary care?
- Research consistently shows that NPs deliver primary care outcomes comparable to those of physicians, with high patient satisfaction scores and similar clinical quality metrics. NPs often spend more time on patient education, preventive care, and chronic disease management. For routine primary care needs, both providers are well qualified. The best choice depends on individual health needs and the complexity of the conditions being managed.
- How much more do doctors make than nurse practitioners?
- Physicians generally earn significantly more than NPs. The median annual salary for NPs is approximately $126,000, while primary care physicians earn around $260,000 or more, and specialists can exceed $350,000. That said, NPs enter practice years earlier with far less educational debt, which narrows the lifetime earnings gap more than raw salary figures suggest, especially in primary care roles.
- Can an NP prescribe controlled substances?
- Yes, NPs can prescribe controlled substances in all 50 states, though the specifics vary. In full practice authority states, NPs prescribe independently, including Schedule II through V medications. In reduced or restricted authority states, NPs may need a collaborative agreement with a physician or face limitations on certain drug schedules. NPs must also hold a DEA registration to prescribe any controlled substance.