Most important takeaways…
- As of 2026, 29 states plus D.C. and two U.S. territories grant nurse practitioners full practice authority.
- More than a dozen states have adopted or expanded FPA legislation since 2021, with several new bills still pending.
- Research links FPA states to measurable improvements in primary care access, especially in rural and underserved communities.
- NP salaries vary more by cost of living, specialty, and employer type than by practice authority level alone.
Twenty-nine states, the District of Columbia, and two U.S. territories now grant full practice authority to nurse practitioners in 2026, meaning NPs in those jurisdictions can evaluate patients, order diagnostics, and prescribe medication without a required physician oversight agreement. That figure has climbed steadily over the past five years, reflecting bipartisan momentum to expand access to primary care and ease regulatory burdens on advanced practice nurses.
The shift is happening fast. Since 2024 alone, multiple state legislatures have debated or enacted FPA bills, while others are amending transition-to-practice rules that once required thousands of supervised hours. For working nurses weighing a move to NP school, practice authority is no longer a static credential issue. It is a variable that shapes where you can practice, how quickly you can open your own clinic, and, in some markets, what you can negotiate in nurse practitioner salary by state and specialty.
Restricted-practice states still outnumber FPA states in certain regions, and transition requirements remain a maze of hour minimums, supervisor credentials, and documentation burdens. Understanding where the lines are drawn, and which states are poised to move, matters before you choose a clinical site or commit to a post-graduation relocation.
What Is Full Practice Authority for Nurse Practitioners?
Full practice authority (FPA) is the legal framework that lets nurse practitioners work to the top of their license without a mandated physician relationship. The American Association of Nurse Practitioners (AANP) defines it as the authority for NPs to evaluate patients, diagnose conditions, order and interpret diagnostic tests, and initiate and manage treatments, including prescribing medications and controlled substances, under the exclusive licensure authority of the state board of nursing.
In practice, FPA means you can open your own clinic, sign death certificates, certify disability paperwork, and prescribe Schedule II medications without paying a physician for a collaborative or supervisory agreement. It does not mean working in isolation. Most NPs in FPA states still consult colleagues, but the choice of when and with whom to collaborate is yours.
The Three Tiers of Practice Authority
The AANP classifies every state and territory into one of three categories. Before you scan the state lists later in this guide, hold this mental model:
- Full practice: State law permits NPs to evaluate, diagnose, prescribe, and manage care independently under the board of nursing.
- Reduced practice: State law reduces NPs' ability to engage in at least one element of practice, typically requiring a career-long collaborative agreement with a physician for prescribing or another function.
- Restricted practice: State law restricts NPs' ability to engage in at least one element of practice, requiring career-long supervision, delegation, or team management by an outside health discipline.
For a detailed breakdown of where each state falls, see our guide to nurse practitioner practice authority by state.
State Law vs. Federal Requirements
FPA is a state-level designation. It governs what your nursing license allows you to do within that state's borders. It is separate from the federal layers that apply to every NP regardless of location: DEA registration to prescribe controlled substances, Medicare and Medicaid enrollment to bill federal payers, and National Provider Identifier (NPI) numbers. Moving to an FPA state does not change those federal requirements, and being in a restricted state does not eliminate them.
The De Facto Fourth Category
A growing number of states grant FPA only after a transition-to-practice period, often 1,000 to 9,000 supervised clinical hours or two to three years working under a collaborative agreement. New graduates in these states function under reduced practice early in their careers and earn independence later, creating what is effectively a fourth tier you will see mapped out in a later section. If you are still exploring whether the NP path is right for you, our overview of how to become a nurse practitioner walks through each milestone from RN to independent practice.
Complete List of Full Practice Authority States in 2026
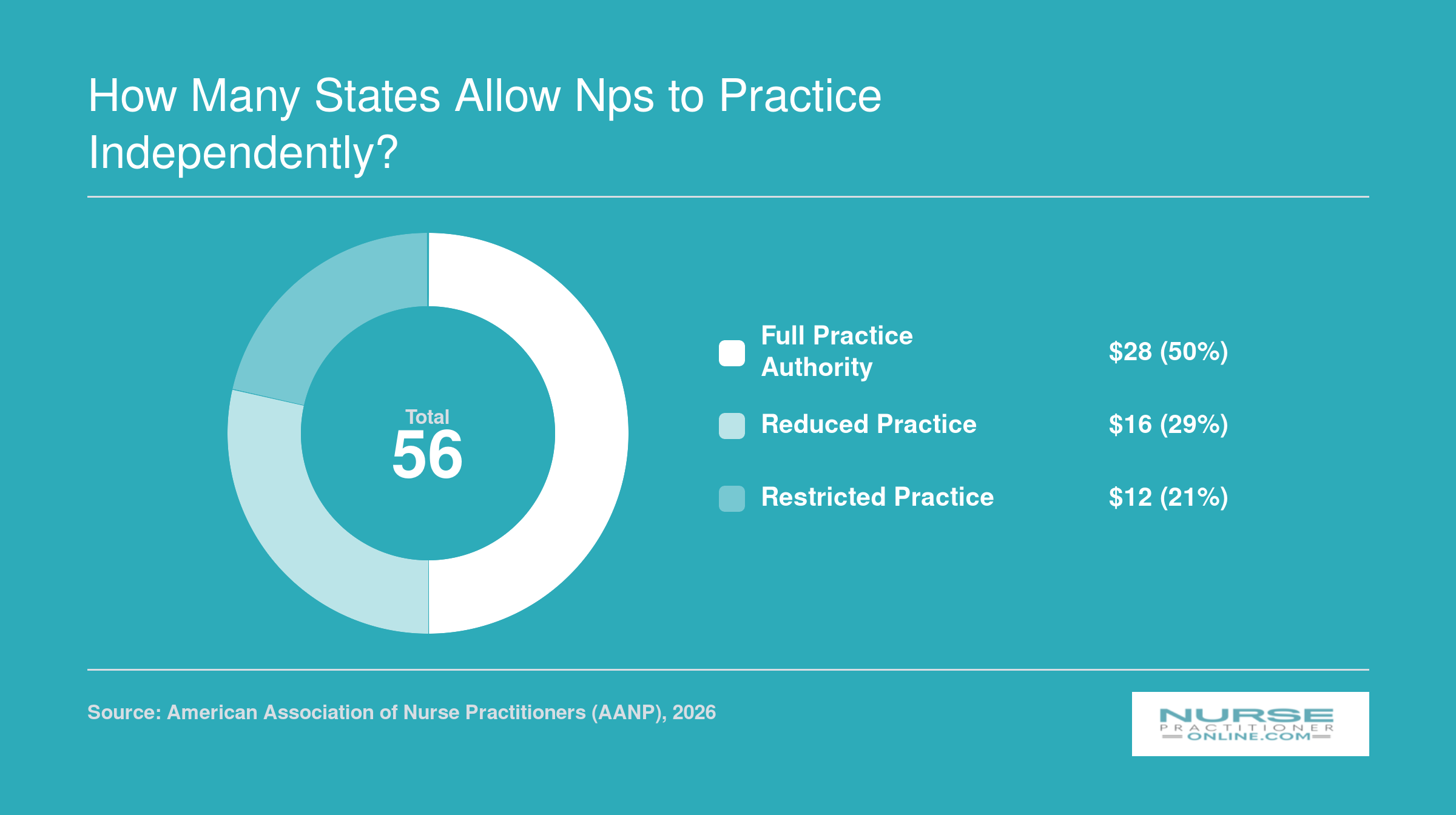
Which states allow nurse practitioners to practice independently in 2026?
As of 2026, 29 states plus the District of Columbia and two U.S. territories grant full practice authority to nurse practitioners.1 That means NPs in these jurisdictions can evaluate patients, diagnose conditions, order and interpret diagnostic tests, and prescribe medications, including controlled substances, without a required physician collaboration or supervision agreement.2 The American Association of Nurse Practitioners tracks this landscape through its State Practice Environment resources, and the growth since 2020 has been substantial.
The Full Practice Authority States
The following states currently grant full practice authority to NPs, along with authorization to prescribe controlled substances:
- Alaska: Full practice authority with controlled substance prescribing authorized.
- Arizona: Full practice authority with controlled substance prescribing authorized.
- Colorado: Full practice authority with controlled substance prescribing authorized.
- Connecticut: Full practice authority with controlled substance prescribing authorized.
- Delaware: Full practice authority with controlled substance prescribing authorized.
- Hawaii: Full practice authority with controlled substance prescribing authorized.
- Idaho: Full practice authority with controlled substance prescribing authorized.
- Iowa: Full practice authority with controlled substance prescribing authorized.
- Kansas: Full practice authority with controlled substance prescribing authorized.
- Maine: Full practice authority with controlled substance prescribing authorized.
- Maryland: Full practice authority with controlled substance prescribing authorized.
- Massachusetts: Full practice authority with controlled substance prescribing authorized.
- Minnesota: Full practice authority with controlled substance prescribing authorized.
- Montana: Full practice authority with controlled substance prescribing authorized.
- Nebraska: Full practice authority with controlled substance prescribing authorized.
- Nevada: Full practice authority with controlled substance prescribing authorized.
- New Hampshire: Full practice authority with controlled substance prescribing authorized.
- New Mexico: Full practice authority with controlled substance prescribing authorized.
- New York: Full practice authority with controlled substance prescribing authorized.
- North Dakota: Full practice authority with controlled substance prescribing authorized.
- Oregon: Full practice authority with controlled substance prescribing authorized.
- Rhode Island: Full practice authority with controlled substance prescribing authorized.
- South Dakota: Full practice authority with controlled substance prescribing authorized.
- Utah: Full practice authority with controlled substance prescribing authorized.
- Vermont: Full practice authority with controlled substance prescribing authorized.
- Washington: Full practice authority with controlled substance prescribing authorized.
- Wyoming: Full practice authority with controlled substance prescribing authorized.
Territories With Full Practice Authority
Two U.S. territories and the nation's capital also belong in this column:
- District of Columbia: Full practice authority with controlled substance prescribing authorized.
- Guam: Full practice authority with controlled substance prescribing authorized.
- Northern Mariana Islands: Full practice authority with controlled substance prescribing authorized.
A Note on Transition-to-Practice Requirements
Full practice authority does not always mean day-one independence. Some states in this group require NPs to complete a transition-to-practice period, typically ranging from one to two years of supervised or collaborative practice, before they can operate fully autonomously. The specifics vary by state, so checking directly with the relevant Board of Nursing is the most reliable step before relocating or opening an independent practice. You can also review nurse practitioner licensing requirements for additional guidance. State-level requirements are covered in more detail in the transition-to-practice section of this guide.
For NPs considering a move or planning to open their own clinic, this list narrows the geography considerably. More than half of U.S. states still place some form of restriction on NP practice, which makes understanding where you land on the map a practical first step in any career planning conversation.
How Many States Allow NPs to Practice Independently?
As of 2026, the majority of U.S. states and territories grant nurse practitioners full practice authority, a notable shift from just five years ago when fewer than half did. The map has changed quickly: since 2021, roughly a dozen additional states have moved to FPA or enacted transition-to-practice pathways that lead to independent practice, reflecting growing recognition that NPs can safely deliver primary and specialty care without physician oversight.
Reduced and Restricted Practice Authority States
Not every state has embraced full practice authority for nurse practitioners. In 2026, more than 20 states still maintain either reduced or restricted practice environments.1 These two categories describe how much mandatory oversight from a physician is required for an NP to perform core clinical duties.
Reduced Practice Authority States
Reduced practice states require a career-long collaborative agreement with a physician. This agreement outlines the scope of practice for nurse practitioners, prescribing authority, and other protocols. The NP cannot practice without this formal partnership in place, and the arrangement does not expire after a set number of practice hours.
As of June 2026, the following states are classified as reduced practice: Alabama, Arkansas, Illinois, Indiana, Kentucky, Louisiana, Mississippi, New Jersey, Ohio, Pennsylvania, West Virginia, and Wisconsin.1 In these states, NPs must maintain a collaborative agreement throughout their career. The specific requirements vary. Some states mandate regular chart reviews, while others require the physician to be available by phone. The core feature, however, is a permanent, legally required link to a collaborating physician.
Restricted Practice Authority States
Restricted practice states go further by mandating ongoing supervision, delegation, or team management by a physician. In these states, NPs cannot independently assess, diagnose, or treat patients without a physician's direct involvement to some degree.
The states with the most stringent oversight, classified as restricted practice, are: California, Florida, Georgia, Michigan, Missouri, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, and Virginia.1 Here, state law requires physician supervision, delegation, or team management for NPs to carry out many functions that full practice authority states allow independently. For example, an NP in these states may need a physician to co-sign orders, be physically present a certain percentage of time, or approve treatment plans.
Practical Effects of These Restrictions
Even within these categories, the day-to-day experience can differ. Some restricted states allow NPs to own their own practices, provided they have a supervising physician on contract. Others limit prescribing authority or require additional continuing education for certain controlled substances. Always check your state board of nursing for the most current rules.
These limitations can affect not only where you practice but also your earning potential and the services you can offer. That is why many NPs consider practice authority when choosing a state to work in or pursue an online NP program. States with fewer restrictions often mean more professional autonomy and, in some cases, higher pay.
Questions to Ask Yourself
Transition-to-Practice Requirements by State
Securing full practice authority in many states means first completing a supervised transition period, yet no single, centralized database tracks every state's specific requirements for hours, duration, or supervisor qualifications. Navigating this patchwork of rules demands a bit of detective work, but knowing where to look saves both time and surprises mid-career.
Start with Your State's Board of Nursing
The official source for any transition-to-practice requirement is your state's Board of Nursing website and the accompanying nurse practice act. These documents spell out whether newly licensed NPs must complete supervised clinical hours before gaining full autonomy, how many hours are required, and whether supervision must come from a physician or can be provided by an experienced NP. For example, Virginia requires new NPs to complete a transition period with a practice agreement, while Kansas has a transition-to-practice requirement before independent practice. Delaware's rules may differ again. Because these regulations change through legislative sessions and administrative rule updates, always verify the current version of your state's nurse practice act rather than relying on older summaries.
Leverage Professional Organization Resources
The American Association of Nurse Practitioners maintains state-by-state practice environment profiles that summarize key regulatory points and often link directly to Board of Nursing pages. The National Council of State Boards of Nursing offers similar compilations. These resources serve as excellent starting points: they distill complex statutes into plain language and flag states with conditional full practice authority pathways. Use them to identify which states impose transition periods, then drill down into the official BON materials for precise hour counts, supervision types, and any additional conditions like continuing education or attestation forms. If you want to get more involved in shaping these policies, our nurse practitioner health policy toolkit outlines practical steps for engaging in the legislative process.
Consult Your Academic Program's Clinical Team
Your NP program's clinical placement office or faculty advisors track active state requirements as part of placing students in preceptorships. They know which states require physician oversight versus experienced-NP mentorship, typical durations (one year, two years, a set number of hours), and whether your clinical hours as a student can count toward the post-licensure transition period. Make sure the program you choose holds proper nursing program accreditation, as accredited programs are more likely to keep current with regulatory changes across states. An email or phone call to your program can clarify nuances that aren't obvious from statute text alone, especially helpful if you're planning to relocate after graduation.
Cross-Reference State Health and Labor Departments
While the Bureau of Labor Statistics focuses on career outlook and wage data, some state labor or health department websites publish workforce development guides that reference NP regulatory pathways. Cross-referencing these with your state's nurse practice act confirms details and sometimes surfaces FAQs or flowcharts that make the process clearer. This dual-source approach catches discrepancies early and ensures you're working from the most current rules before committing to a job offer or relocation.
Recent Legislative Changes and Pending FPA Bills (2024–2026)
Which states have made the biggest moves toward full practice authority in 2024, 2026, and what bills are on the horizon? The legislative landscape remains active, as more than half of U.S. states now grant NPs full practice authority.1 Several key battlegrounds, however, are seeing high-stakes debates and sunset deadlines.
New York's Time-Limited FPA and the Push for a Permanent Fix
New York granted NPs a form of independent practice authority as part of its COVID-19 response, but the measure was codified with a sunset date of July 2026.2 With that deadline approaching, lawmakers introduced S2360 to remove the expiration and make full practice authority permanent.2 As of mid-2026, the bill sits in the Senate Higher Education Committee, and its passage is far from certain. The current law requires NPs to complete 3,600 hours of supervised practice before they can practice independently, a threshold that has already shaped workforce patterns.2 If S2360 does not pass before the sunset, New York NPs would revert to a collaborative agreement requirement, disrupting care delivery and potentially reducing access in underserved areas.
Pennsylvania's SB 717: One Chamber Down, One to Go
Pennsylvania remains one of the most closely watched states because it has long required physician collaboration. In the 2024, 2026 legislative session, SB 717 advanced through the Senate and now awaits action in the House.3 The bill would eliminate the collaborative agreement mandate for experienced NPs, aligning the state with the growing number of full practice authority states. Advocacy groups note strong support from rural health organizations, but physician opposition remains entrenched. If passed, Pennsylvania would become the latest state to modernize its NP practice environment.
Other States with Active FPA Legislation
Several other states have active bills that could reshape practice authority in the coming year:
- Massachusetts: Legislation to grant full practice authority has been reintroduced and is under committee review. Proponents cite the state's shortage of primary care providers in western and central regions.
- Michigan: A bipartisan package of bills would remove mandatory collaboration for NPs and certified nurse midwives after a transition-to-practice period. Committee hearings have been held, but a floor vote has not yet been scheduled.
- Florida: Multiple bills to reduce or eliminate collaboration requirements have been filed, but they face strong headwinds in the legislature, where past attempts have stalled.
These states join a handful of others where bills are pending in various stages, but the political climate and lobbying efforts make their fates unpredictable.
Partial Advances: Prescriptive Authority and Reduced Collaboration
Not all scope-of-practice changes amount to full FPA. Some states have opted for incremental reforms that expand prescriptive authority or loosen collaboration requirements without fully removing them. For example:
- Texas has considered measures to reduce the administrative burden of collaboration for NPs in certain settings, though the core requirement remains in place.
- South Carolina recently enacted legislation that simplifies the prescriptive authority process for NPs without granting independent practice.
These partial steps often serve as testing grounds for broader reforms later.
Federal Momentum: The ICAN Act and VA Autonomy
At the federal level, the ICAN Act (Improving Care and Access to Nurses Act) was reintroduced in Congress in 2023 and remains pending.4 If passed, it would authorize NPs and other advanced practice registered nurses to practice independently under Medicare and Medicaid, removing barriers that conflict with state-level FPA. Separately, the Veterans Health Administration has already established full practice authority for NPs within VA facilities regardless of state law, a policy that has withstood legal challenges and is often cited as a model for broader reform. Though the ICAN Act has not yet advanced out of committee, its provisions continue to attract bipartisan support as a way to address healthcare workforce shortages. If you want to make your voice heard on these issues, consider exploring how nurse practitioners can get involved in politics.
Related Articles
NP Salaries by Practice Authority Level: Do FPA States Pay More?
One of the most common questions working nurses ask is whether practicing in a full practice authority (FPA) state translates to higher pay. The answer is nuanced. While several of the highest-paying states do grant FPA, factors like cost of living, employer demand, and specialty mix also play major roles. Below is a snapshot of median NP salaries across states with different practice authority levels, drawn from the latest Bureau of Labor Statistics data.
| State | Practice Authority Level | Median Annual Salary | 25th Percentile | 75th Percentile | Total NPs Employed |
|---|---|---|---|---|---|
| California | Reduced | $166,610 | $140,260 | $205,400 | 20,980 |
| New Jersey | Reduced | $149,620 | $126,030 | $162,250 | 9,590 |
| Alaska | Full | $145,450 | $104,000 | $165,510 | 570 |
| New York | Reduced | $145,390 | $128,190 | $164,670 | 20,430 |
| Oregon | Full | $144,600 | $129,840 | $163,240 | 2,430 |
| Washington | Full | $140,220 | $125,890 | $161,730 | 4,790 |
| Connecticut | Full | $138,960 | $125,910 | $159,680 | 3,680 |
| Massachusetts | Full | $138,890 | $125,590 | $160,310 | 8,920 |
| New Mexico | Full | $138,440 | $113,240 | $156,000 | 1,870 |
| Arizona | Full | $133,790 | $115,290 | $151,650 | 7,540 |
| Montana | Full | $133,640 | $112,180 | $141,050 | 1,050 |
| New Hampshire | Full | $132,440 | $120,270 | $143,010 | 1,790 |
| District of Columbia | Full | $131,380 | $119,240 | $143,960 | 790 |
| Hawaii | Full | $130,940 | $121,410 | $158,100 | 470 |
| Rhode Island | Full | $130,710 | $126,200 | $160,030 | 1,200 |
| Texas | Restricted | $129,880 | $110,570 | $143,860 | 21,690 |
| Colorado | Full | $129,750 | $110,300 | $139,440 | 4,130 |
| Vermont | Full | $129,740 | $115,650 | $139,930 | 680 |
| Iowa | Full | $129,420 | $115,950 | $137,900 | 2,810 |
| Florida | Restricted | $129,010 | $109,670 | $143,670 | 24,690 |
| Idaho | Full | $128,940 | $119,290 | $140,920 | 1,570 |
| Illinois | Reduced | $128,620 | $111,450 | $138,420 | 9,560 |
| Wisconsin | Reduced | $128,580 | $117,630 | $137,150 | 4,950 |
| Minnesota | Full | $128,570 | $103,250 | $139,590 | 8,690 |
| Indiana | Full | $128,280 | $111,210 | $134,840 | 7,470 |
How Full Practice Authority Affects Patient Access and Outcomes
States that grant full practice authority and states that restrict it are, in many ways, running two parallel experiments in how to deliver primary care. The research increasingly suggests that removing barriers to independent NP practice produces measurable gains in access, especially for patients who need it most, without sacrificing quality.
What the Research Shows About Access
A national difference-in-differences study published through the IZA Institute of Labor Economics found that states adopting full practice authority saw increases in the share of nurse practitioners working in health professional shortage areas.1 NPs in those states were also more likely to enter self-employment, effectively opening new practice sites in communities that lacked adequate provider coverage.1 A separate systematic review covering studies from 2000 through 2019 confirmed the pattern: expanded NP practice regulations improved access in rural and underserved areas without decreasing the quality of care delivered.2
Additional research adds another dimension. In states with full practice authority, older adults showed improved self-reported health and fewer functional limitations.3 Those same populations used fewer nursing home and home care services, suggesting that accessible NP-led primary care may help patients maintain independence longer and reduce reliance on costlier care settings.3
The Quality and Safety Question
Physician organizations have long raised concerns that independent NP practice could compromise patient safety. The evidence, however, does not support that claim. A 2023 systematic review examined 37 studies comparing NP-delivered care to physician-delivered care and found outcomes to be comparable across multiple clinical measures.4 These findings echo the conclusions of the National Academies of Sciences, Engineering, and Medicine, which recommended removing scope-of-practice barriers in its landmark Future of Nursing reports. Both the Federal Trade Commission and the National Governors Association have also endorsed reducing practice restrictions as a strategy to address provider shortages, particularly in primary care.
None of this means every NP should practice without mentorship on day one. Many full practice authority states include transition-to-practice periods that allow new NPs to build clinical confidence before working independently. The point is that the regulatory ceiling, not the individual clinician's readiness, should not be the limiting factor.
How Medicaid Reimbursement Fits In
Practice authority on paper means little if payers do not recognize NPs as independent billing providers. In many full practice authority states, NPs can bill Medicaid directly without routing claims through a collaborating physician. This matters enormously for NPs who want to open practices in underserved communities, where Medicaid patients often make up a large share of the population. When an NP cannot bill independently, the business model for a solo or small-group NP practice becomes much harder to sustain, even if state law technically permits independent clinical decision-making.
States that pair full practice authority with direct Medicaid billing create the strongest conditions for NPs to fill gaps in primary care. States that grant clinical independence but maintain restrictive reimbursement policies can inadvertently undercut the access gains that FPA is designed to produce. Understanding the role of a primary care nurse practitioner helps illustrate why these reimbursement pathways matter so much.
The Bigger Picture
For nurses considering the NP path, these findings carry a practical takeaway. Where you practice can shape not just your salary and autonomy but also the kind of impact you have on your community. If working with underserved populations appeals to you, understanding whether a state offers both full practice authority and favorable reimbursement policies is worth factoring into your career planning alongside program rankings and tuition costs. Exploring nurse practitioner advancement opportunities can help you align your goals with the right practice environment.
More than 290,000 nurse practitioners are now licensed across the United States, according to the American Association of Nurse Practitioners. This rapidly growing workforce plays a critical role in expanding access to primary care, particularly in rural and underserved communities where physician shortages remain acute.
Frequently Asked Questions About NP Practice Authority
Nurse practitioner practice authority rules vary widely across the country and can shift from one legislative session to the next. Below are answers to some of the most common questions working nurses ask when exploring NP career paths and considering where to practice.
- How many states allow nurse practitioners to practice independently in 2026?
- As of 2026, more than half of U.S. states plus the District of Columbia grant full practice authority (FPA) to nurse practitioners. The exact count continues to climb as additional states pass or implement FPA legislation. Because some new laws include phased rollouts or transition periods, it is worth checking individual state board websites for the most current effective dates before making relocation or career decisions.
- Can nurse practitioners prescribe controlled substances in full practice authority states?
- Yes. In FPA states, nurse practitioners can independently prescribe medications, including Schedule II through V controlled substances, without a collaborative agreement or physician co-signature. Prescriptive authority details, such as whether a separate DEA registration or state controlled substance license is required, vary slightly by jurisdiction. NPs should verify their state board's specific prescriptive rules and maintain an active DEA number to prescribe controlled substances lawfully.
- What is the difference between full, reduced, and restricted practice authority?
- Full practice authority allows NPs to evaluate, diagnose, treat, and prescribe without physician oversight. Reduced practice authority requires a collaborative agreement with a physician for at least one element of practice, most often prescribing. Restricted practice authority mandates direct physician supervision, delegation, or team management for NPs to deliver care. The classification system, maintained by the American Association of Nurse Practitioners, helps NPs quickly understand the regulatory landscape in any given state.
- Do NPs in FPA states earn more than NPs in restricted states?
- Salary differences between FPA and restricted states exist, but they are influenced by many factors beyond practice authority, including cost of living, demand, specialty, and practice setting. Some FPA states rank among the highest paying, partly because independent NPs can bill directly and retain a larger share of revenue. However, several restricted states also offer competitive salaries due to high demand or metropolitan market rates, so authority level alone does not determine earnings.
- Which states are most likely to pass FPA legislation next?
- Several states with reduced or restricted authority have had active FPA bills in recent legislative sessions. States where momentum has been building include those with strong APRN advocacy coalitions, growing rural healthcare shortages, or bipartisan legislative support. Because the political landscape changes each session, nurses interested in a specific state should follow updates from the state nurses association and the American Association of Nurse Practitioners for the latest bill status and projected timelines.
- Does full practice authority mean NPs can open their own practice without any physician involvement?
- In most FPA states, yes. Nurse practitioners can legally establish, own, and operate an independent clinical practice, including billing insurers directly, without a supervising or collaborating physician. However, NPs must still comply with state business licensing requirements, malpractice insurance mandates, facility regulations, and any applicable transition to practice periods. Some states also require NPs to complete a set number of supervised clinical hours before practicing independently.
- How do transition-to-practice requirements work for new NPs?
- Some FPA states require newly certified nurse practitioners to complete a supervised or mentored practice period, often ranging from roughly 2,000 to 4,000 hours, before they can practice without oversight. During this transition period, the NP works under a formal agreement with a physician or experienced NP. Once the required hours and any additional documentation are completed, the NP can apply for full, independent practice privileges through their state board of nursing.