Most important takeaways…
- Nurse practitioners can make over 200 clinical decisions per shift, and judgment quality declines steadily with each one.
- Decision fatigue is not the same as burnout: it is a cognitive depletion that can exist independently of emotional exhaustion.
- Evidence-based shift strategies such as batching low-stakes decisions and front-loading complex cases measurably protect patient safety.
- Organizational solutions like standardized protocols and optimized clinical decision-support tools reduce NP cognitive load more effectively than individual coping alone.
A primary care nurse practitioner may make 150 to 200 patient-facing clinical decisions in a single shift; an emergency or urgent care NP can push past 300. Each one, from antibiotic selection to disposition, carries real weight for patient outcomes and your own liability.
Decision fatigue is not the same as feeling tired at the end of a long day. It is a measurable decline in judgment quality, documented in studies of physicians, judges, and surgeons, that worsens with each successive choice regardless of how rested you feel at 7 a.m.
The practical tension for NPs in 2026 is sharp: patient volumes and documentation demands keep climbing, while the cognitive bandwidth required to practice safely has not expanded to match. In the sections ahead, we'll unpack what decision fatigue actually is, how it differs from burnout, how it affects patient safety, and what evidence-based strategies you can use to protect your clinical judgment across every shift.
What Is Decision Fatigue and Why Are NPs Especially Vulnerable?
Decision fatigue is the measurable decline in the quality of your choices and clinical judgment after you've made a large number of decisions in a short period. Psychologist Roy Baumeister's ego-depletion framework introduced this idea: willpower and self-control act like a muscle that tires with use. More recent self-regulation research refines the model, showing that while the exact mechanism remains debated, the phenomenon is real and repeatable across contexts. After hours of diagnostic reasoning, prescription decisions, and care-planning conversations, your mental reserves deplete. You start opting for default choices, deferring harder calls, or making judgment errors you'd never make at the start of your shift.
The NP Decision Load: Unique and Constant
Nurse practitioners carry an exceptionally dense decision load. You hold autonomous prescribing authority in most states, conduct differential diagnoses without a supervising physician's real-time input, make referral and discharge decisions independently, and deliver patient education that shapes adherence and outcomes. Unlike physicians who often work within team-based models with built-in consult layers (hospitalists conferring with specialists, residents escalating to attendings), many NPs function as the sole provider in their clinical moment, especially those serving as a primary care nurse practitioner. You're the first and last decision-maker on the front line.
A 2024 study examining nursing work environments found that nearly one-third of nurses reported significant decision fatigue, and the phenomenon was tightly linked to job stress and environmental demands.1 While that study focused on the broader nursing workforce, advanced practice providers face an amplified version of this load. A 2025 systematic review on healthcare decision fatigue reported that 45 percent of included studies documented statistically significant performance declines tied to cumulative decision demands.2 Although the review didn't isolate NPs, the findings align closely with APP workflows.
Why NP Practice Models Amplify Vulnerability
Several structural factors make nurse practitioners especially prone to decision fatigue:
- Independent practice authority: In full practice authority states, you carry the entire diagnostic and therapeutic decision chain without mandatory physician oversight.
- High patient panels: Primary care and urgent care NPs routinely see 20 to 30 patients per shift, each encounter requiring multiple discrete clinical decisions.
- Multi-site coverage: Many NPs rotate across clinics, hospitals, or telehealth platforms within a single week, losing the cognitive efficiency that comes from environmental familiarity.
- Fewer institutional buffers: Compared to physicians in large hospital systems, NPs in independent or rural practices often lack immediate peer consultation, decision-support staff, or administrative backup.
These conditions converge to create a sustained, high-volume decision environment with limited recovery windows. Recognizing your vulnerability isn't about questioning your competence. It's about understanding the cognitive cost of the autonomy and scope you've earned.
Decision Fatigue Vs. Burnout: Understanding the Difference
The conversation around clinician well-being has matured considerably in recent years, yet many nurse practitioners still conflate two distinct challenges: decision fatigue and burnout. Untangling these concepts is more than an academic exercise. Knowing which one you are experiencing right now shapes the kind of help that will actually work.
A Clear Framework for Each
Decision fatigue is a state-like, situation-dependent decline in decision quality that emerges after sustained cognitive, emotional, and moral load during a single shift.1 It is acute and reversible. After a demanding stretch of complex patient encounters, you may notice yourself defaulting to shortcuts, deferring choices, or feeling mentally unable to weigh one more set of options. A practical way to recognize it: "I am too mentally spent to make one more good decision today."
Burnout, as defined by the Maslach Burnout Inventory, is a chronic occupational syndrome with three dimensions: emotional exhaustion, depersonalization or cynicism, and reduced personal accomplishment.1 It builds over weeks and months from a sustained imbalance between job demands and resources. Its hallmark feeling sounds different: "I feel emotionally exhausted, detached, and ineffective most days." Research from Stanford Medicine has linked burnout with higher odds of self-reported medical errors, while studies indexed by the National Institutes of Health associate decision fatigue specifically with impaired judgment and reduced diagnostic accuracy within the workday.3
Where They Overlap and Where They Don't
Decision fatigue can act as a precursor or accelerant of burnout. When the cognitive drain of making hundreds of clinical decisions repeats day after day without adequate recovery, it feeds the exhaustion and reduced efficacy that define burnout.1 However, the reverse is not always true. A nurse practitioner experiencing burnout may feel emotionally depleted without necessarily showing the shift-level decline in decisional consistency that characterizes decision fatigue. The two conditions share terrain, but they occupy different timescales and respond to different levers. The intensity of decision-making varies by practice setting; for example, acute care vs primary care roles carry very different cognitive loads across a typical shift.
Related Conditions Worth Knowing
NPs commonly encounter two additional forms of occupational distress that overlap with, but are distinct from, both decision fatigue and burnout:
- Compassion fatigue: Gradual, empathy-driven distress from repeated exposure to patients' suffering, marked by emotional withdrawal and reduced compassionate capacity. You might notice a numbing response after caring for one critically ill patient after another.
- Moral injury: Distress that arises when you are exposed to, participate in, or cannot prevent actions that violate your deeply held professional or ethical values. It often surfaces as a persistent sense that you were unable to do the right thing for a patient, not because of your own shortcomings, but because of systemic constraints.
Being able to name which of these experiences you are having is the first step toward choosing the right response.
Why the Distinction Matters for Interventions
Decision fatigue responds to same-day tactical changes. Restructuring your schedule so that the most cognitively demanding encounters happen earlier, batching similar decisions, sharing the decision load with colleagues, and building in brief cognitive recovery breaks can all restore decisional quality within a shift.
Burnout requires a fundamentally different set of interventions. Addressing burnout means tackling workload distribution, staffing levels, role clarity, values alignment, autonomy, and sustained recovery time. These are systemic and psychological changes that no single scheduling hack can resolve.
If you find yourself reaching for burnout-level solutions when the real problem is acute cognitive depletion, you may miss simple fixes that could improve your decision quality today. Conversely, if you keep treating a deepening sense of exhaustion and detachment with shift-level tactics alone, you risk ignoring a problem that demands broader organizational and personal change. Accurately diagnosing which challenge you face is, fittingly, one of the most important decisions you can make for your own practice and well-being.
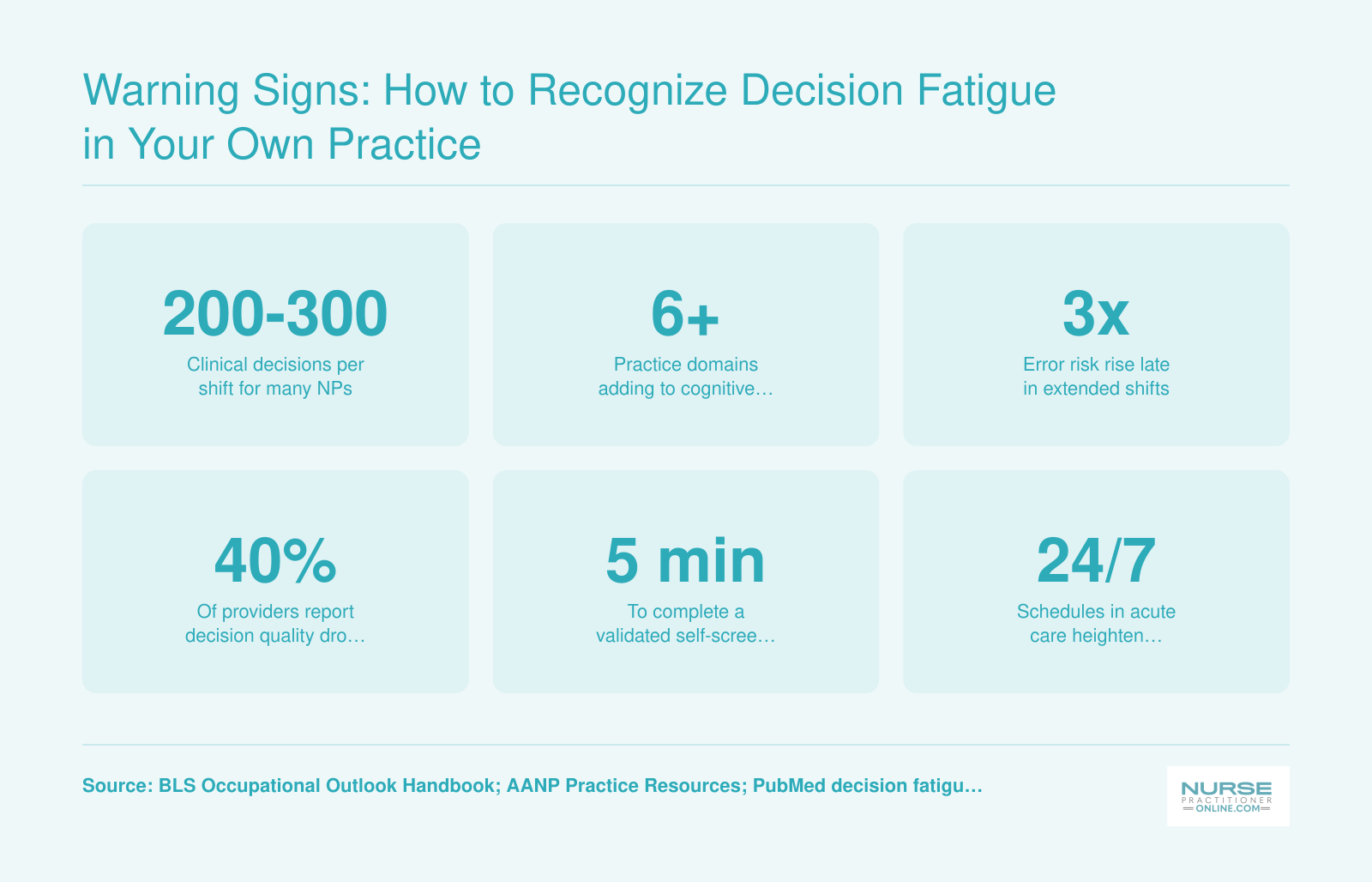
Warning Signs: How to Recognize Decision Fatigue in Your Own Practice
Decision fatigue often builds gradually, making it hard to spot in yourself. Validated instruments such as the NASA Task Load Index and the Cognitive Failures Questionnaire can help you measure cognitive load objectively. Search PubMed for 'decision fatigue assessment' filtered to 2022 through 2026 for the latest validation studies, and check AANP or your NP program's evidence-based practice databases for self-screening toolkits.
How Decision Fatigue Affects Patient Safety and Clinical Outcomes
When your cognitive reserves run low after hours of continuous clinical decision-making, the consequences extend well beyond personal discomfort. A growing body of research suggests that decision fatigue contributes to measurable declines in the quality and safety of patient care, and nurse practitioners should understand exactly what is at stake.
Prescribing Errors and Diagnostic Drift
Studies in primary care and emergency settings have found that clinicians become more likely to choose the path of least resistance as their shifts progress. Research on antibiotic prescribing, for example, has shown that clinicians are more likely to prescribe antibiotics inappropriately later in a clinic session compared to the beginning, even when clinical indications have not changed. Similar patterns have been observed with opioid prescribing and with reduced adherence to recommended cancer screening protocols as appointment slots wear on. While much of this research focuses on physicians, the underlying cognitive mechanism applies equally to NPs making the same types of decisions in the same environments.
A study examining telephone triage nurses found that the likelihood of making a more conservative (and potentially unnecessary) clinical decision increased by roughly 5.5 percent with each successive call handled.1 Over the course of a full shift, that incremental drift adds up, translating into more unnecessary referrals, more emergency department visits, and higher costs for patients and health systems alike.
The Autonomy Factor for NPs
What makes decision fatigue especially concerning for nurse practitioners is the degree of clinical autonomy many hold. In the majority of states, NPs practice independently or with minimal physician oversight. You can review how scope of practice varies across the country in this breakdown of nurse practitioner practice authority by state. This means that a fatigued prescribing decision or a missed diagnostic cue may not pass through a second set of eyes before it reaches the patient. Unlike settings with built-in peer review or co-signature requirements, the autonomous NP is often the sole decision-maker from assessment through treatment. That independence is a strength of the profession, but it also means there is less of a safety net when cognitive resources are depleted.
Downstream Costs You Cannot Ignore
The ripple effects of decision fatigue go beyond individual patient encounters:
- Patient harm: Missed diagnoses, unnecessary procedures, and inappropriate prescriptions can lead to adverse outcomes ranging from mild to life-threatening.
- Malpractice exposure: Patterns of late-shift errors or deviation from clinical guidelines can become focal points in malpractice claims, particularly when documentation shows a consistent decline in decision quality over the course of a shift.
- Institutional liability: Employers and health systems share legal and financial exposure when staffing models or scheduling practices contribute to clinician fatigue, making this an organizational concern as much as a personal one.
It is worth noting that research in this area is still evolving, and most studies have examined physicians or nurses in specific settings rather than NPs directly. However, the cognitive science underlying decision fatigue is well established and not role-dependent. The mental resources required to evaluate symptoms, weigh differential diagnoses, and choose treatment plans deplete in predictable ways regardless of your clinical title. Understanding this reality is the first step toward protecting both your patients and your career.
Common Causes and Triggers by NP Practice Setting
Decision fatigue manifests differently depending on where you practice, and understanding your setting's unique stressors can help you build targeted defenses against cognitive overload.
Emergency and Urgent Care Settings
Nurse practitioners in emergency departments and urgent care clinics face relentless decision velocity. You might evaluate 20 to 30 patients per shift, each requiring rapid triage, diagnostic reasoning, and treatment decisions under time pressure. The constant interruptions, frequent diagnostic uncertainty, and limited patient history compound the cognitive load. One minute you're managing chest pain in a 65-year-old, the next you're evaluating a pediatric rash, then pivoting to a possible stroke. This constant context-switching drains your mental reserves faster than almost any other practice setting.
Primary Care and Family Practice
Primary care NPs confront a different challenge: decision complexity rather than velocity. You manage panels of 15 to 25 patients daily, each with multiple chronic conditions, polypharmacy concerns, and psychosocial factors. A single visit might require you to adjust diabetes medications, screen for depression, address preventive care gaps, navigate insurance formularies, and coordinate with specialists. Research on chronic condition management shows that NPs in states with full practice authority demonstrate readmission rates for high blood pressure at 0.9758 compared to 0.9834 in restricted-authority states, suggesting that practice autonomy may actually improve decision quality rather than compromise it.1 Yet the sheer volume of clinical variables you must weigh, visit after visit, steadily depletes your decision-making stamina.
Specialty and Procedure-Based Practices
Specialty NPs, including those in highest paid NP specialties, often face fewer but higher-stakes decisions. Whether you're in cardiology, oncology, or a procedural setting, each clinical choice carries significant weight. The liability exposure adds psychological pressure. According to data on scope-of-practice expansion, office-based NPs face particular vulnerability to state board licensure complaints, which can create a subtle but persistent background anxiety that increases the mental effort required for each clinical decision.2
Regulatory Environment as a Hidden Trigger
Your state's practice authority significantly affects decision fatigue. In restricted-authority states, the requirement to consult or obtain physician approval for certain decisions adds cognitive steps and interrupts your clinical flow. Research from 2014 identified limited practice control as the primary driver of NP turnover.3 When you cannot execute decisions you're trained and competent to make, the resulting friction creates unnecessary mental wear. With roughly 300,000 nurse practitioners currently practicing nationwide and 45 percent job growth projected through 2032, understanding how regulatory constraints affect your cognitive load becomes essential for long-term career sustainability.4 If you're feeling the weight of these regulatory barriers, exploring nurse practitioner advancement opportunities or learning how nurse practitioners can get involved in politics may help you channel that frustration into meaningful change.
Related Articles
Evidence-Based Strategies to Manage Decision Fatigue During Shifts
The core challenge is straightforward but tricky in practice: you cannot reduce the total number of decisions your shift demands, but you can restructure when and how you make them to preserve the quality of each one. Research on clinical decision fatigue in hospital settings is still growing, with a 2024 scoping review identifying 17 empirical studies on the topic, so some of these strategies carry stronger evidence than others.1 Here is what the current literature and clinical experience suggest.
Front-Load Your Hardest Decisions
Shift structuring, which has moderate evidence behind it, centers on a simple principle: your cognitive resources are highest at the start of a shift, so that is when you should tackle diagnostic workups, medication changes, and new patient intakes.1 If you have any scheduling flexibility, resist the temptation to ease into the day with inbox cleanup. Save those low-stakes tasks for the afternoon or the final hours of a 12-hour stretch, when your decision quality naturally dips. Even small adjustments, like seeing your most complex patient first instead of third, can pay dividends over the course of a shift.
Take Micro-Recovery Breaks (Even Tiny Ones Count)
Pushing through without a pause feels productive, but evidence from a 2025 review in clinical settings suggests that breaks as short as one to five minutes can help restore attention.2 The overall evidence quality for micro-breaks is still considered low, meaning more rigorous studies are needed, yet the practical signal is consistent: a brief walk down the hallway, a few sips of water, or a short breathing exercise appears to reset focus better than powering through.1 If you can carve out five to ten minutes between patient encounters, even better. The key is frequency over duration.
Use Checklists and Decision Protocols
Checklist use and cognitive offloading both carry strong evidence for reducing unnecessary mental effort.1 Standardized screening algorithms, prescribing pathways, and order sets exist precisely so you do not have to rebuild a decision from scratch every time you encounter a routine case. Clinical decision support systems can also help by sorting alerts into tiers (critical, moderate, minor) and types (active vs. passive), reducing the cognitive load of low-priority notifications.3 Using these tools is not a sign of inexperience. It is a deliberate strategy that reserves your cognitive energy for the atypical presentations that genuinely require clinical reasoning. Certain nurse practitioner apps can further support cognitive offloading by putting evidence-based references at your fingertips during a shift. Think of every protocol-driven decision as one fewer withdrawal from a limited daily account.
Batch Similar Tasks Together
Rather than toggling between a patient encounter, three refill requests, a lab result, and two inbox messages, group similar decisions into dedicated time blocks. Refill requests in one pass. Lab reviews in another. Message responses in a third. The evidence base for decision batching in clinical environments is still insufficient to draw firm conclusions, but the cognitive science behind task-switching costs is well established outside healthcare.1 Every context switch carries a small penalty. Batching minimizes those penalties and helps you maintain a consistent decision-making rhythm.
Protect Basic Physiological Needs
You may have encountered the idea that willpower runs on glucose. The simplified version of that model has been debated in psychology research, and it is not settled science. What is far less controversial is this: skipping meals, running on caffeine alone, and staying dehydrated directly impair sustained attention and working memory.2 You do not need a peer-reviewed trial to know that hunger and dehydration make complex thinking harder. Keep a water bottle within reach, eat something substantial before or during your shift, and treat these basics as clinical tools rather than luxuries.
Putting It All Together
No single strategy eliminates decision fatigue on its own. The strongest approach combines several of these practices into a personal shift routine:
- Complex cases first: Schedule your most demanding clinical work for early in the shift.
- Micro-breaks every 90 to 120 minutes: Even one to five minutes of stepping away can help.
- Protocol-driven routine decisions: Lean on checklists and algorithms for standard presentations.
- Batched administrative tasks: Group refills, labs, and messages into set windows.
- Nourishment and hydration: Treat eating and drinking as non-negotiable parts of your workflow.
Adopting even two or three of these habits consistently can make a noticeable difference in how sharp your clinical judgment feels at hour ten compared to hour two. The goal is not perfection. It is building a sustainable rhythm that protects your patients and your own well-being across every shift.
Questions to Ask Yourself
Organizational and Team-Based Solutions for NP Decision Load
Individual coping strategies versus systemic workplace change: both matter, but research consistently shows that organizational-level solutions carry more weight in protecting clinician cognitive capacity over the long term. As a nurse practitioner, you can only do so much on your own. When the structure around you generates excessive decision volume, adjusting your diet or meditation practice will not close that gap.
Reducing Administrative Burden at the Source
One of the clearest contributors to NP decision fatigue is administrative load: the documentation, prior authorizations, referral coordination, and inbox management that pile on top of direct patient care. Healthcare systems that have introduced medical scribes report measurable gains in clinician focus and satisfaction. When someone else handles real-time documentation, the NP's attention stays on the clinical problem rather than splitting between the patient and the chart. If your organization has not explored scribe programs or ambient documentation tools, making the case to your leadership is a reasonable starting point.
Professional organizations including the AANP and the AMA have published practice resources and policy briefs addressing clinician workload and administrative burden. Their recommendations often include concrete benchmarks that administrators can act on, and bringing those materials into a conversation with your practice manager adds credibility to the ask. If you want to take that advocacy further, learning how nurse practitioners can get involved in health policy gives you additional leverage.
Patient Panel Size and Scheduling Models
Panel caps, meaning limits on the number of patients assigned to a single clinician, directly influence how many decisions an NP must make in a day. Some health systems have piloted adjusted scheduling models that build in buffer time between complex patients or designate certain appointment slots for straightforward concerns. The Bureau of Labor Statistics and state nursing boards publish data on staffing ratios and workload trends that can inform these conversations at the policy level.
Searching PubMed or Google Scholar using terms like "clinician decision fatigue" and "organizational interventions" will surface recent case studies from health systems that have tested and measured these approaches.
Delegation and Team-Based Care Protocols
Clear delegation protocols are another underused lever. When medical assistants, licensed practical nurses, or care coordinators are empowered to handle tasks within their scope, the NP's decision queue shortens considerably. Academic nursing and medical programs have published research on effective delegation frameworks, often available through faculty blogs or institutional repositories.
The goal is not to push work onto colleagues who are also stretched thin, but to design team workflows where each role operates at the top of its scope. That structural alignment protects everyone's cognitive resources, which ultimately protects patients.
Technology and Decision-Support Tools: Help or Hindrance?
Clinical decision-support tools are software features built into your electronic medical record or added as standalone applications that prompt you with alerts, diagnostic suggestions, drug interaction warnings, and order recommendations while you work. In theory, they lighten your cognitive load by surfacing the right information at the right moment. In practice, the relationship between these tools and decision fatigue is more complicated than most vendors admit.
When Decision Support Helps
Well-designed clinical decision-support systems (CDSS) can genuinely reduce cognitive burden. Tools that auto-populate evidence-based order sets, flag dangerous drug interactions before you sign a prescription, or surface relevant screening reminders can spare you from holding every guideline in working memory. AI-assisted triage platforms entering primary care and urgent care settings promise to pre-sort patient acuity so you spend less mental energy on low-yield decisions. When these systems are tightly curated and context-sensitive, they free up the decisional bandwidth you need for complex cases.
When Decision Support Hurts
The same technology becomes a source of fatigue when it generates a relentless stream of low-value alerts. Research consistently shows that clinicians override the vast majority of electronic alerts, often because the warnings are irrelevant, redundant, or poorly timed. Every dismissed pop-up still costs you a micro-decision, and hundreds of those micro-decisions per shift erode the same cognitive reserves you need for genuine clinical judgment. This phenomenon, often called alert fatigue, can paradoxically make you more likely to miss a truly critical warning buried among dozens of trivial ones.
Evaluating Tools for Your Own Practice
Before adopting or advocating for a new decision-support tool, take a practical, investigative approach:
- Check the evidence base: Look for peer-reviewed studies on PubMed or through your professional association (such as AANP or ANCC) that evaluate whether the tool actually improves outcomes in settings similar to yours.
- Review override and alert rates: Ask your IT team or vendor how frequently alerts are dismissed. High override rates signal noise rather than help.
- Consult government and industry sources: The Agency for Healthcare Research and Quality (AHRQ) publishes guidance on CDSS design and effectiveness. The Office of the National Coordinator for Health IT (ONC) maintains resources on health technology standards. These are solid starting points for separating marketing claims from evidence.
- Assess workflow fit: A tool that works well in a large hospital system may add friction in a small primary care office. Request a trial period and track whether the technology reduces or increases the number of decisions you make per patient encounter.
A Balanced Perspective
Technology is neither a guaranteed solution nor an inherent problem. The key is whether a given tool reduces the total number of meaningful decisions you face or simply replaces one form of cognitive load with another. Advocate within your organization for regular audits of alert relevance, customizable notification settings, and NP input during system configuration. You are the end user, and your feedback shapes whether these tools protect decision quality or quietly erode it.
NP Salary and Career Outlook: Why Protecting Your Decision Capacity Matters
Nurse practitioners represent one of the highest-earning and fastest-growing segments of the healthcare workforce, with more than 307,000 NPs employed nationally. The financial stakes of career longevity are significant: an NP earning at or above the national median has a compelling reason to invest in cognitive sustainability strategies rather than grinding through shifts until a preventable error or burnout forces a career exit. Protecting your decision capacity is not just a wellness goal, it is a career preservation strategy that safeguards both your patients and your earning potential.
| Salary Percentile | Annual Earnings |
|---|---|
| 25th Percentile | $109,940 |
| National Median | $129,210 |
| National Mean | $132,000 |
| 75th Percentile | $149,570 |
Frequently Asked Questions About NP Decision Fatigue
Decision fatigue is a growing concern for nurse practitioners who face hundreds of clinical choices every shift. Below are answers to the most common questions NPs ask about recognizing, understanding, and managing this cognitive challenge.
- What is decision fatigue in nursing?
- Decision fatigue is the gradual decline in decision quality that occurs after making a large number of choices over a sustained period. In nursing and NP practice, this means that the mental energy required to assess patients, order diagnostics, prescribe treatments, and triage urgent concerns accumulates throughout a shift. As cognitive resources deplete, practitioners may default to the easiest option or avoid making decisions altogether.
- How does decision fatigue affect patient safety in NP practice?
- When decision fatigue sets in, nurse practitioners are more likely to take cognitive shortcuts, miss subtle clinical findings, or delay critical orders. Research links depleted cognitive capacity to increased diagnostic errors, less thorough medication reconciliation, and inconsistent adherence to evidence-based protocols. Over time, these lapses can contribute to adverse patient events, making decision fatigue a genuine patient safety concern rather than just a personal comfort issue.
- What is the difference between decision fatigue and burnout for nurse practitioners?
- Although they often overlap, decision fatigue and burnout are distinct. Decision fatigue is a temporary cognitive depletion tied specifically to the volume and complexity of choices made during a shift; it can improve with rest and strategic scheduling. Burnout is a chronic emotional and physical exhaustion that develops over weeks or months, involving depersonalization and reduced professional fulfillment. Unmanaged decision fatigue, however, can accelerate the path toward burnout.
- How can nurse practitioners reduce decision fatigue during shifts?
- Evidence-based strategies include batching similar decisions together, using clinical protocols and standardized order sets to reduce repetitive low-stakes choices, scheduling the most complex cases earlier in the shift, and taking brief cognitive breaks. Meal timing matters too: maintaining stable blood glucose supports sustained mental performance. Delegating appropriate tasks to support staff and establishing personal decision routines for common scenarios also preserve cognitive energy for high-stakes clinical moments.
- What are the warning signs of decision fatigue in clinical practice?
- Common warning signs include increased indecisiveness, a tendency to defer or delay non-urgent decisions, choosing the default or "safe" option without fully analyzing alternatives, irritability during patient encounters, and difficulty concentrating on complex cases late in a shift. Some NPs also notice they spend disproportionate mental energy on trivial choices (like charting wording) while rushing through more consequential clinical reasoning.
- Can technology and AI help reduce decision fatigue for NPs?
- Yes, when implemented thoughtfully. Clinical decision support systems, smart order sets, and AI-driven differential diagnosis tools can reduce the cognitive load of routine decisions by surfacing relevant data and evidence at the point of care. However, poorly designed alerts, excessive pop-up notifications, and redundant documentation requirements can actually increase cognitive burden. The key is selecting tools that streamline workflows rather than adding new decision points to an already demanding shift.