Most important takeaways…
- Roughly half of nurse practitioners report burnout symptoms, with rates varying significantly by specialty and practice setting.
- Replacing a single burned-out NP costs organizations an estimated $80,000 to $120,000 in turnover expenses.
- Burnout is a systems problem: mindfulness, workload advocacy, and policy reform are all evidence-based strategies for prevention.
- Understanding your salary position can inform practical decisions like reducing hours or switching specialties to protect your well-being.
What does nurse practitioner burnout actually look like, and how is it different from the burnout nurses talk about in general?
Nurse practitioners occupy a distinctive professional position: they carry diagnostic and prescriptive responsibility comparable to physicians while often working within institutional structures that do not fully recognize or support that authority. That gap, between what the role demands and what the system provides, is exactly where burnout takes root. Studies consistently show that NPs report higher emotional exhaustion than staff nurses, in part because the role expands clinical accountability without always expanding the resources, autonomy, or staffing that make that accountability sustainable.
NP burnout is not simply nurse burnout with a graduate degree attached. The stressors differ in kind, not just degree, from managing complex chronic disease panels solo to negotiating scope-of-practice restrictions that vary by state. In 2026, workforce data continue to flag advanced practice providers as a high-risk group for attrition, a concern with direct implications for patient access and organizational stability. For NPs looking to take a proactive approach, exploring nurse practitioner advancement opportunities can open doors to roles that better align clinical authority with professional support.
What Is Nurse Practitioner Burnout?
The question is not whether you will face professional stress as a nurse practitioner, but whether that stress will accumulate into something more damaging. Burnout represents a specific syndrome that develops when chronic workplace stress goes unmanaged, and understanding its clinical definition helps you recognize it before it derails your career.
The WHO Framework: Three Dimensions of Burnout
The World Health Organization's ICD-11 classification defines burnout through three interconnected dimensions. In NP practice, each manifests in distinct ways:
- Emotional exhaustion: You feel depleted before your shift even begins. The mental energy required to assess patients, make diagnostic decisions, and navigate complex cases leaves you running on empty. Many NPs describe feeling like they have nothing left to give, not just physically tired but emotionally hollowed out.
- Depersonalization: You catch yourself viewing patients as problems to solve rather than people to help. This cynical detachment serves as a psychological defense mechanism, but it erodes the therapeutic relationships that drew you to advanced practice nursing.
- Reduced personal accomplishment: Despite managing patient panels, making accurate diagnoses, and improving outcomes, you feel ineffective. Accomplishments that once brought satisfaction now feel meaningless or invisible.
Why NP Burnout Differs From RN Burnout
Nurse practitioners face stressors that registered nurses generally do not encounter. You carry diagnostic and prescriptive authority, meaning the weight of clinical decisions rests directly on your shoulders. You manage your own patient panels with productivity expectations tied to billing metrics. You navigate coding requirements that affect practice revenue. Perhaps most notably, you operate within scope of practice for nurse practitioners politics that vary by state and can create daily friction with physicians, administrators, or insurance companies. These added responsibilities create a burnout profile distinct from bedside nursing.
Measuring Burnout: The Maslach Burnout Inventory
The gold-standard tool for measuring burnout is the Maslach Burnout Inventory, which assesses three subscales that mirror the WHO dimensions: emotional exhaustion, depersonalization, and personal accomplishment. Researchers and clinicians use this validated instrument to quantify burnout severity. Later in this article, you will find self-assessment questions adapted from this framework to help you gauge where you stand.
Burnout Is Not Compassion Fatigue or Moral Injury
Though these terms often appear together, they describe different phenomena. Compassion fatigue stems from absorbing patients' trauma and suffering. Moral injury occurs when you are forced to act against your ethical values, such as discharging a patient you know needs more care. Burnout, by contrast, develops from sustained workplace demands regardless of trauma exposure or ethical conflict. In NP settings, all three frequently co-occur, which makes accurate identification essential for choosing the right interventions.
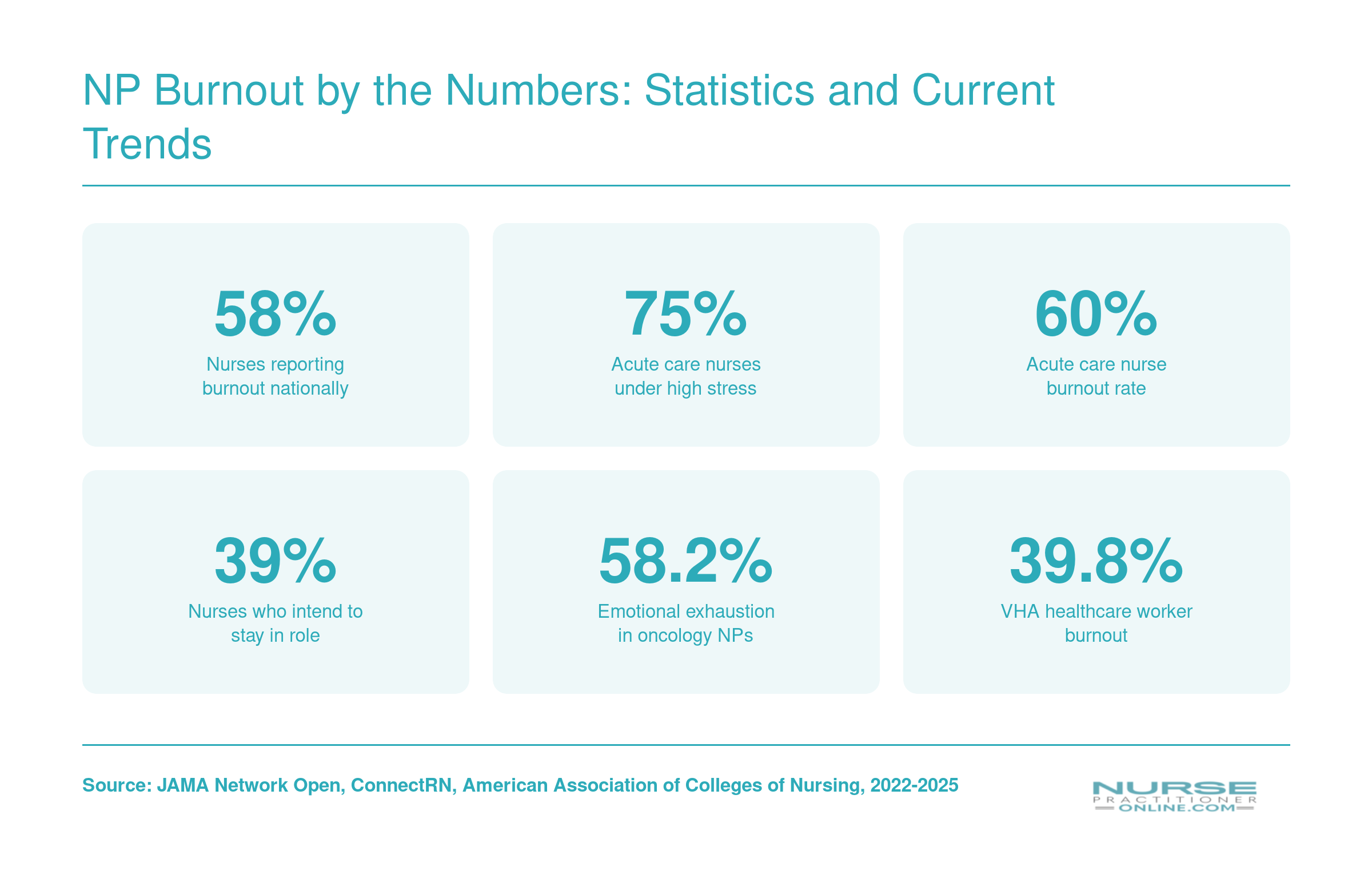
NP Burnout by the Numbers: Statistics and Current Trends
Burnout among nurse practitioners is part of a broader crisis sweeping the nursing profession. These figures, drawn from national surveys and peer-reviewed research, paint a sobering picture of where things stand. If any of these numbers feel personal, you are far from alone.
What Causes Burnout in Nurse Practitioners?
Burnout in nurse practitioners rarely traces back to a single cause. It builds from a stack of structural, administrative, and interpersonal pressures unique to the NP role. Understanding these drivers matters because the fix is almost never "try harder." The fix usually lives at the system level, and recognizing that protects you from blaming yourself for problems your workplace created.
Scope-of-Practice Restrictions and Supervision Requirements
In states that require physician collaboration or supervision, NPs often describe a frustrating gap between their training and what they are legally permitted to do. Position statements from the American Association of Nurse Practitioners (AANP) have long argued that restrictive practice environments correlate with lower job satisfaction. When you are credentialed to manage a patient panel independently but must route routine decisions through a collaborating physician, the friction adds up: delayed care, redundant chart reviews, and the quiet exhaustion of working under someone else's signature. These restrictions also limit opportunities for NPs to serve as primary care nurse practitioners, compounding frustration for those trained to lead patient panels.
If you want to dig into the evidence, the Journal of the American Association of Nurse Practitioners (JAANP) and the Journal of Nursing Regulation publish peer-reviewed studies on scope-of-practice impact. Cross-reference these with your state board of nursing for the current legal landscape, since rules shift year to year. For those who want to advocate for change, learning how nurse practitioners can get involved in politics is a practical next step.
Documentation Burden and Productivity Pressure
Electronic health record (EHR) work has become one of the most cited burnout drivers across primary care. NPs frequently report finishing notes after hours, a pattern sometimes called "pajama time." Layer on relative value unit (RVU) productivity targets, and the workday becomes a race: see more patients, document more thoroughly, code more accurately, all in the same finite hours.
Panel size compounds the problem. Recommended panel sizes from primary care research typically fall well below what many NPs actually carry, especially in underserved areas. The mismatch between recommended and assigned workload is a structural risk factor, not a personal failing.
Role Ambiguity and Professional Isolation
Many NPs work in settings where their role is poorly understood by patients, administrators, or even colleagues. You may be introduced as a nurse, billed as a provider, and evaluated against physician benchmarks, all in the same shift. This identity friction wears people down.
For a fuller picture of what your peers are experiencing, the AANP National NP Sample Survey and ANA workforce reports offer solid data. Peer-reviewed databases like PubMed and CINAHL, available through most university libraries, let you search NP-specific burnout studies rather than relying on general nursing literature, which often misses the distinct pressures of advanced practice.
Questions to Ask Yourself
Warning Signs and Symptoms of NP Burnout: A Self-Check Framework
Most NPs don't wake up one day feeling burned out. The shift is gradual, and by the time it's obvious to you, colleagues have often already noticed something is off.
The Three Dimensions of Burnout: What They Look Like in Practice
Research on clinician burnout consistently organizes symptoms around three dimensions, most famously described by Christina Maslach.1 Each plays out differently in a nurse practitioner's day-to-day reality.
Emotional exhaustion is the dimension most NPs recognize first. Signs include arriving at work already depleted before you've seen a single patient, feeling unable to offer empathy you know a patient needs, physical fatigue that goes well beyond the hours you actually worked, and dreading the next patient call before the current visit has ended.
Depersonalization is subtler and, for many NPs, harder to admit. You might catch yourself referring to patients by their diagnosis rather than their name, feeling a cold indifference toward patients who visit frequently, or responding to patient distress with impatience rather than curiosity. If you find yourself struggling with these interactions, our guide on dealing with difficult patients offers practical strategies. This dimension often feels like a personality change, which is exactly why colleagues tend to spot it before you do.
Reduced personal accomplishment can look like chronic second-guessing of clinical decisions you would have made confidently a year ago, a persistent sense that you're just generating prescriptions rather than practicing medicine, or losing any satisfaction when a patient improves.
A Quick Self-Check: Seven Honest Questions
Before reaching for a formal tool, ask yourself:
- Do I leave work most days feeling emotionally emptied out, even on lighter-volume shifts?
- Have I started cutting patient conversations short to get through the panel faster?
- Do I find myself internally rolling my eyes at certain patients or presentations?
- Has a colleague or partner commented that I seem detached, irritable, or unlike myself?
- Am I doubting clinical calls I used to make without hesitation?
- Do I feel little satisfaction when a patient thanks me or reports feeling better?
- Has the idea of calling in sick just to avoid the day crossed my mind more than once this month?
If you answered yes to three or more, it's worth taking a validated assessment seriously, not as a diagnosis, but as a starting point for a real conversation with yourself.
Validated Tools Worth Knowing
Several well-established instruments can help you get a clearer picture. The full Maslach Burnout Inventory (MBI-HSS) covers 22 items across all three dimensions described above.1 It's the most widely cited tool in this space, though it's proprietary and requires a purchase. Shorter abbreviated versions exist (one at 12 items, another at 9), but research indicates abbreviated versions can overestimate burnout compared to the full scale, so treat scores as directional rather than definitive.2
The Copenhagen Burnout Inventory (CBI) covers 19 items across personal burnout, work-related burnout, and patient-related burnout. It's publicly available at no cost and has been widely used in healthcare research.1 The Professional Quality of Life Scale (ProQOL) goes a step further with 30 items examining compassion satisfaction alongside burnout and secondary traumatic stress, making it particularly useful for NPs who deal with trauma-heavy patient populations. It's also free to access.1
It's worth noting that none of these tools were developed or validated specifically in nurse practitioner populations. They originated in broader clinician and helping-profession contexts, so use your clinical judgment in interpreting results. The National Academy of Medicine has published a useful overview comparing burnout survey instruments if you want to dig deeper.
Ask Someone You Trust
No self-report tool catches everything, especially when burnout is distorting your self-perception. Consider asking a trusted coworker directly: "Have you noticed any changes in how I interact with patients or the team?" It's an uncomfortable question, but the answer is often more useful than any scale.
How Burnout Differs by NP Specialty and Setting
Burnout is not a one-size-fits-all experience for nurse practitioners. Where you practice, and the specialty you choose, significantly shapes your daily stressors, emotional demands, and risk of exhaustion. Understanding these differences can help you anticipate challenges and advocate for support.
Outpatient Primary Care: Moderate Burnout with Growing Strain
Family and primary care NPs in outpatient clinics report a burnout prevalence around 25%.1 This is moderate compared to other specialties but still concerning. Many primary care NPs face heavy patient panels, administrative burdens, and the emotional toll of managing chronic conditions in a resource-limited setting. In 2026, nearly a quarter of primary care advanced practice providers, including NPs and PAs, reported distress related to limited control over their workload, a key driver of burnout.2 While outpatient settings typically avoid overnight shifts, the cumulative weight of documentation and patient complexity can erode job satisfaction over time.
Hospital-Based Acute Care: High Acuity, High Burnout
NPs working in hospitals, ICUs, or as hospitalists experience burnout rates estimated between 35% and 40%.3 The combination of night shifts, high patient acuity, and rigid staffing ratios creates a perfect storm for emotional exhaustion and depersonalization. Acute care NPs must make rapid, high-stakes decisions while coordinating with large care teams, often on rotating schedules that disrupt sleep and work-life balance. If you're weighing these two tracks, our guide to acute care vs primary care NP differences can help you evaluate what fits your lifestyle. The relative risk in this setting is high, making it one of the most demanding paths for nurse practitioner well-being.
Psychiatric-Mental Health: The Weight of Trauma
Psychiatric-mental health NPs face burnout prevalence in the 30% to 40% range, with a moderate-to-high relative risk.3 This specialty carries unique emotional burdens: repeated exposure to patient trauma, managing suicide risk, and navigating underfunded community mental health systems. Heavy caseloads and the intensity of therapeutic relationships can lead to compassion fatigue, even for those deeply committed to mental health care. Without strong peer support and clinical supervision, the invisible weight of this work can become overwhelming.
Emergency and Urgent Care: Burnout in the Fast Lane
Emergency and urgent care NPs report some of the highest burnout rates, between 35% and 45%.3 Long shifts, chaotic environments, and the need to triage rapidly with limited patient background push stress to extreme levels. NPs considering or already working in this space can explore emergency nurse practitioner programs designed to build resilience through structured clinical training. The high acuity and relentless pace mean recovery between shifts is often insufficient. Add in shift work and the physical demands of a fast-moving unit, and it is no surprise that emergency NPs face a high relative burnout risk compared to their peers in lower-acuity settings.
These patterns underscore a critical point: burnout prevention must be tailored. A one-size-fits-all wellness program won't address the night-shift fatigue of an ICU NP or the emotional depletion of a psychiatric provider. Recognizing the risks inherent to your own specialty and setting is the first step toward building a sustainable, fulfilling career.
Evidence-Based Strategies to Prevent and Recover From NP Burnout
What are the real, study-backed ways to reduce nurse practitioner burnout, and what should you do if you're already in crisis? The evidence points to several focused, high-yield strategies that go well beyond standard self-care advice.
Mindfulness-Based Stress Reduction (MBSR) Programs
A 2026 meta-analysis of 16 randomized controlled trials found that structured MBSR programs produced a large reduction in burnout scores among NPs (Cohen's d = -1.43).1 Over just 8 weeks, participants showed an 11% improvement in mindfulness, a 6% decrease in depersonalization, and a 10% gain in personal accomplishment.2 These aren't abstract benefits; they reflect measurable shifts in how you experience work. MBSR typically involves weekly group sessions and daily meditation practice, and its protocolized nature makes it replicable and reliable.
Cognitive-Behavioral Resilience Training
Another high-impact option blends cognitive-behavioral techniques with resilience-building. A 2026 study reported that such training increased resilience scores by 9.78 points and improved sleep quality by a large effect (d = -1.10).1 While individual responses varied, as shown by a wide confidence interval (0.38 to 19.17), many NPs gained concrete tools to challenge unhelpful thoughts and manage emotionally charged situations. Shorter modules, often delivered online, can fit into a busy schedule.
Protecting Sleep Through Structured Rest Practices
Sleep disruption is both a cause and a symptom of burnout. The same interventions that reduce burnout also significantly improve sleep quality, creating a positive feedback loop. For example, the 2026 resilience training study found a large effect on sleep improvement (d = -1.10, 95% CI: -1.79 to -0.41).1 Incorporating elements of CBT-I, such as consistent bedtimes and relaxation techniques, into your routine can reinforce these gains and protect against emotional exhaustion.
Organizational Tweaks with Growing Support
While individual strategies are essential, adjustments to work structure also matter. Compressed workweeks, where NPs work three 12-hour shifts followed by multiple days off, and designated "admin time" blocks free from direct patient care have shown promise in reducing burnout in nursing populations. However, rigorous NP-specific randomized data are still scarce. Similarly, peer support groups like Balint gatherings and Schwartz Rounds can foster psychological safety and shared coping. These approaches address the relational isolation that fuels burnout, though their effectiveness varies by setting.
Recovery: Evidence-Based Care for the Already Burned Out
If you're already experiencing severe burnout, marked by persistent dread, emotional numbness, or impaired concentration, professional intervention is critical. Cognitive-behavioral therapy (CBT) and acceptance and commitment therapy (ACT) are both effective modalities; they help you reframe stress and reconnect with your professional values. When symptoms start to compromise patient care or personal safety, medical leave should be considered. Some NPs find that exploring non-clinical nurse practitioner jobs can provide a meaningful reset while keeping their career on track. A structured return-to-practice plan, developed with a therapist and your employer, can include phased schedules, reduced patient volume, and ongoing counseling until you regain full functioning. Ignoring severe burnout risks long-term career disengagement and health consequences.
The Limits of Personal Resilience
No mindfulness app or resilience workbook can offset chronic understaffing, EHR overload, or lack of autonomy. These systemic drivers require organizational and policy change. While building your personal toolkit is a necessary first line of defense, true burnout prevention must tackle the broken systems that cause it, the subject of the next section.
Organizational and Policy Solutions NPs Should Advocate For
Individual resilience strategies help, but burnout is fundamentally a systems problem that requires systemic fixes. Nurse practitioners cannot self-care their way out of unsafe panel sizes, inadequate support staff, or hostile practice environments. Real change demands that NPs use their collective voice to reshape the organizations and policies that govern their daily work.
Organizational Levers: What to Push For Inside Your Facility
Nurse practitioners should advocate for concrete changes within their own health systems. Start with safe panel size caps that reflect evidence-based workload standards, not revenue targets. Primary care NPs report burnout rates around 25 percent, and practice environment factors are a significant driver of that figure.1 Yet many organizations continue to expand panels without adding clinicians. Request protected documentation time built directly into clinic schedules, ensuring that charting occurs during paid hours rather than spilling into evenings and weekends.
Employer-funded mental health benefits matter only if NPs can use them without stigma. Advocate for confidential Employee Assistance Programs, peer support groups, and formal debriefing protocols after traumatic events. Critically, push for dedicated support staff such as medical assistants, scribes, and care coordinators. When NPs inherit tasks that should belong to other roles (answering phone calls, faxing referrals, chasing lab results) the cognitive load becomes unsustainable. Your organization should staff to role, not to budget.
State and Federal Policy: The Levers That Shape Your Practice
Policy change may feel abstract, but it directly affects your day-to-day stress. Full practice authority, now enacted in 27 states plus the District of Columbia and two U.S. territories as of 2026, removes unnecessary physician oversight requirements that constrain scheduling flexibility and geographic practice options.2 While comprehensive burnout data in full practice authority states remain limited, preliminary evidence suggests that practice environment barriers contribute significantly to NP burnout, and removing those barriers may reduce strain.1
Other policy levers include state staffing ratio mandates that explicitly include advanced practice providers, OSHA workplace violence protections that mandate de-escalation training and incident reporting, and clarity around ADA and FMLA accommodations for burnout-related mental health conditions. These are not abstract legislative goals. They determine whether you have backup during a crisis, legal recourse after an assault, or protected leave when you need it.
How to Advocate Practically
Join your state nurse practitioner association and the American Association of Nurse Practitioners, both of which actively lobby for full practice authority and improved working conditions.2 If you want a step-by-step roadmap for political engagement, our nurse practitioner health policy toolkit walks through seven practical actions you can take today. Volunteer for or request a seat on your facility's wellness committee, where you can propose concrete policy changes. If your workplace has union representation, use that channel to negotiate safer workloads. Advocacy does not require a law degree; it requires showing up, naming the problem, and proposing the fix.
According to the 2026 NSI National Health Care Retention and RN Staffing Report, the average cost of turnover for a single registered nurse is roughly $60,090. When burnout drives even a handful of nurse practitioners or nurses out of an organization, the financial losses can quickly reach into the millions.
How NP Salary and Career Outlook Factor Into Burnout Decisions
Earning a strong salary does not immunize you from burnout, but understanding exactly where you fall on the pay spectrum can help you make informed decisions about reducing your hours, switching specialties, or relocating. The table below, based on approximate 2024 Bureau of Labor Statistics data for nurse practitioners, shows the salary spread from the 25th to the 75th percentile. Notice that the gap between lower and higher earners is nearly $40,000. If you are on the lower end, financial stress may be compounding your emotional exhaustion, making it harder to cut back on shifts or invest in self care. On the other hand, if you are closer to the 75th percentile, you may have more room to negotiate a schedule change without a devastating impact on your household finances. For any NP seriously considering leaving the profession altogether, weighing a median salary of roughly $129,000 against what alternative careers offer is a critical step before making a permanent decision.
| Salary Metric | Annual Earnings |
|---|---|
| 25th Percentile | $109,940 |
| Median (50th Percentile) | $129,210 |
| Mean (Average) | $132,000 |
| 75th Percentile | $149,570 |
| Total National Employment | 307,390 |
Frequently Asked Questions About NP Burnout
Burnout raises real questions about your health, your rights, and your next steps. Here are straightforward answers to the concerns nurse practitioners ask most often.
- What is the burnout rate for nurse practitioners?
- Research consistently shows that roughly 30 to 50 percent of nurse practitioners report moderate to severe burnout at any given time. Rates spiked during and after the pandemic, and surveys through 2025 and into 2026 suggest they remain elevated. The exact figure depends on the specialty, practice setting, and measurement tool, but the trend is clear: burnout affects a significant share of the NP workforce.
- What are the early signs of nurse practitioner burnout?
- Watch for persistent emotional exhaustion that does not resolve after a day off, growing cynicism toward patients or colleagues, difficulty concentrating on clinical decisions, and a declining sense of professional accomplishment. Physical symptoms such as chronic headaches, disrupted sleep, and frequent illness also appear early. If you notice yourself dreading shifts you once enjoyed or emotionally detaching from patient interactions, those are reliable early red flags.
- How is NP burnout different from regular nurse burnout?
- NP burnout carries unique stressors tied to autonomous prescribing responsibility, diagnostic decision making, and navigating scope of practice restrictions. Nurse practitioners also face administrative burdens like insurance credentialing and documentation demands that bedside RNs typically do not. The combination of higher clinical accountability, productivity quotas, and sometimes limited organizational support creates a burnout profile distinct from that of staff nurses.
- Which NP specialty has the highest burnout rate?
- Primary care and psychiatric/mental health NPs consistently report some of the highest burnout rates. Primary care NPs face heavy patient panels and chronic disease management loads, while psych NPs absorb significant emotional labor from patients in crisis. Emergency and acute care NP roles also trend high due to shift intensity and unpredictable workloads. Specialty clinics with more predictable schedules generally report lower rates.
- What should I do if I'm already burned out as an NP?
- Start by talking to your primary care provider or a mental health professional who understands healthcare work. Prioritize immediate self care: sleep, nutrition, physical activity, and social connection. Evaluate whether your workload or schedule can be renegotiated with your employer. Consider peer support groups specifically for nurse practitioners. If your current role is unsustainable, explore a lateral move to a different setting or specialty before leaving the profession entirely.
- Can my employer fire me for taking leave due to burnout?
- If you qualify under the Family and Medical Leave Act (FMLA), you are entitled to up to 12 weeks of unpaid, job protected leave for a serious health condition, which can include burnout related diagnoses like major depression or anxiety disorders. State laws may offer additional protections. Document your condition with a healthcare provider, notify HR in writing, and consult an employment attorney if you face retaliation or termination after requesting leave.
- Are there free burnout assessment tools for nurse practitioners?
- Yes. The Maslach Burnout Inventory is the gold standard in research, though the full version requires a license. Free screening alternatives include the Professional Quality of Life (ProQOL) scale, the Copenhagen Burnout Inventory, and the Mini Z Burnout Survey developed by the American Medical Association. Many professional NP organizations also host self assessment quizzes on their websites. These tools are not diagnostic, but they can help you gauge where you stand and decide whether to seek professional support.
Nurse practitioner burnout is a systemic crisis, not a personal failing. No amount of meditation or boundary-setting will fix unsafe staffing ratios, and no organizational policy will work if you refuse to delegate or take time off. Both personal strategies and institutional reform are essential, and neither is sufficient alone.
This week, take a validated burnout self-assessment like the Maslach Burnout Inventory or the Professional Quality of Life Scale. If your score raises concern, talk to a colleague, supervisor, or counselor before the quarter ends. Early intervention matters. The NP profession is growing, and the shift toward full practice authority is accelerating across states. Burned-out nurse practitioners who stay in the field and advocate for better working conditions are shaping what comes next. Protecting your career means protecting yourself first.