Most important takeaways…
- Thirty states now grant NPs full practice authority to independently diagnose and treat patients.
- Mnemonics like VINDICATE and OLDCARTS keep your differential broad when presentations seem ambiguous.
- Always include at least one life-threatening diagnosis on every differential to avoid missing critical conditions.
- Thorough documentation of your reasoning protects patients, supports billing, and strengthens legal defensibility.
Most new nurse practitioners graduate with strong clinical skills and pass their certification boards, yet many report feeling underprepared for the independent diagnostic reasoning required in actual practice. The transition from RN pattern recognition to building and narrowing a differential diagnosis list is a distinct skill gap, one that no single clinical rotation or didactic course fully resolves. A 2025 survey of new-graduate NPs found that 68% felt only somewhat confident or not confident at all in generating a differential diagnosis independently during their first six months of practice.
Differential diagnosis is not intuition. It is a systematic process of generating a ranked list of possible conditions, testing the top hypotheses, and ruling out dangerous or treatable causes before settling on a final diagnosis. The stakes are high: diagnostic errors contribute to an estimated 40,000 to 80,000 patient deaths annually in the United States. New NPs practicing under full practice authority carry the same legal and professional responsibility as their physician colleagues, yet many lack structured frameworks for diagnostic reasoning beyond what they absorbed during preceptorships.
What Is Differential Diagnosis and Why It Matters for NPs
Thirty states and territories now grant full practice authority to nurse practitioners, meaning NPs in those jurisdictions can independently evaluate, diagnose, and treat patients without physician oversight. That number has grown from just 22 states in 2021, reflecting a clear legislative trend toward expanding NP autonomy.2 Understanding differential diagnosis is central to exercising that authority safely and effectively.
Defining Differential Diagnosis
Differential diagnosis is a ranked list of possible conditions that could explain a patient's presenting symptoms. You start with the broadest possibilities, then systematically narrow the list using clinical evidence: patient history, physical exam findings, diagnostic tests, and response to treatment. The goal is not to guess correctly on the first try but to think comprehensively, prioritize likely diagnoses, and rule out dangerous conditions before they cause harm.
For new NPs, this process can feel overwhelming. You are moving from a nursing framework focused on patient response to illness into a diagnostic framework that requires you to name the illness itself. That shift demands deliberate practice and a structured approach.
Can a Nurse Practitioner Diagnose a Patient?
Yes, but your diagnostic scope depends on where you practice. The American Association of Nurse Practitioners classifies state regulations into three tiers:3
- Full practice authority: NPs evaluate, diagnose, and manage patients independently. Approximately 30 states and territories currently fall into this category.
- Reduced practice authority: NPs can diagnose and treat, but state law requires a collaborative agreement with a physician. About 15 states use this model.
- Restricted practice authority: NPs must practice under physician supervision for at least some aspect of patient care, including diagnosis. Roughly 11 states maintain these restrictions.
Before you see your first patient, know your state's requirements. You can review nurse practitioner practice authority by state for a detailed breakdown. Even in full practice authority states, your employer or credentialing body may impose additional limitations.
How NP Diagnostic Reasoning Differs
Nurse practitioners and physicians learn many of the same diagnostic frameworks, and the clinical overlap is substantial. Both professions use pattern recognition, hypothesis testing, and evidence-based guidelines to reach conclusions. However, NP education emphasizes a holistic, patient-centered approach that integrates the patient's social determinants of health, family context, and self-management capacity into diagnostic thinking.
This does not mean NP diagnoses are "softer" or less rigorous. It means you are trained to consider how a diagnosis will affect the whole person, not just which ICD code applies. That perspective is an asset in primary care, where chronic disease management and preventive care require ongoing patient engagement. It is also a key reason many patients choose a nurse practitioner as primary care provider.
Why Differential Diagnosis Is a High-Stakes Skill
Missed and delayed diagnoses are the leading cause of malpractice claims against nurse practitioners. New NPs are particularly vulnerable because they are still building the pattern library that experienced clinicians rely on. When you see a complaint you have never encountered before, you have no mental shortcut to guide your thinking.
The medicolegal risk is not just about getting the diagnosis wrong. It is about failing to document your reasoning, neglecting to consider dangerous alternatives, or not following up appropriately when initial treatment does not work. A well-constructed differential, documented clearly, protects both you and your patient.
As you progress through this guide, you will learn frameworks and mnemonics that help you build a reliable differential for common chief complaints, recognize red-flag symptoms that demand immediate action, and avoid the cognitive traps that trip up new clinicians.
According to the World Health Organization, approximately 5% of outpatient diagnoses contain errors. This means that in a typical primary care week, several patients may leave with an incomplete or inaccurate assessment. Building strong differential diagnosis skills helps new nurse practitioners reduce these preventable diagnostic gaps and improve patient outcomes.
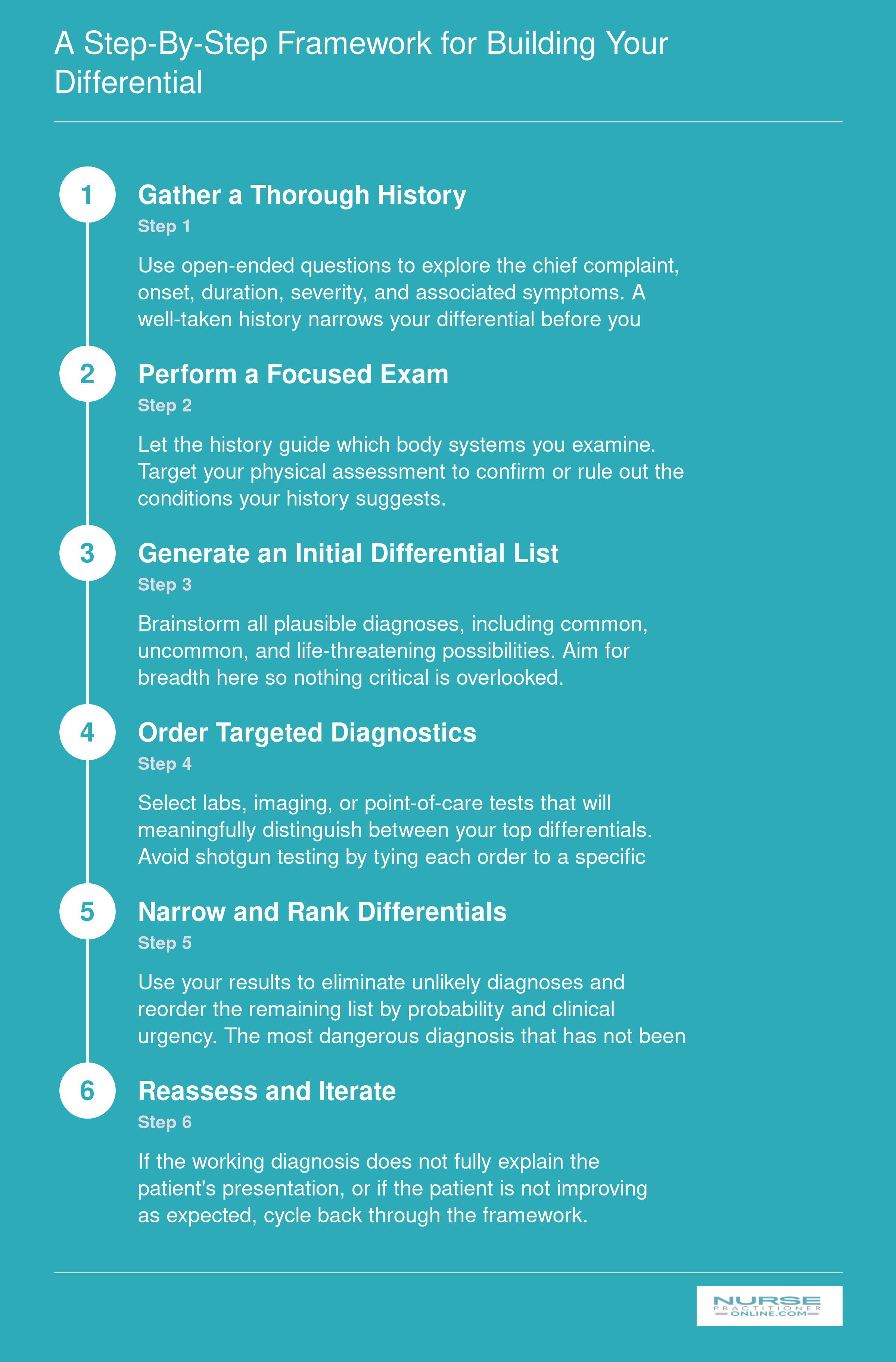
A Step-by-Step Framework for Building Your Differential
Differential diagnosis is not a single moment of insight. It is a structured, repeatable cycle you can practice until it becomes second nature. Follow these six steps every time a patient presents with a new complaint.
How to Build Your Differential: A Practical NP Framework
Some new NPs start ordering tests the moment a patient describes symptoms. Others pause, gather data systematically, and generate hypotheses before touching a lab slip. The second approach leads to better diagnostic accuracy, fewer unnecessary tests, and stronger clinical reasoning skills.
Step One: Comprehensive History Taking
Every differential diagnosis begins with a thorough history. Use OLDCARTS to structure your history of present illness: Onset (when did it start?), Location (where exactly?), Duration (how long does it last?), Character (sharp, dull, burning?), Aggravating factors (what makes it worse?), Relieving factors (what helps?), Timing (constant or intermittent?), and Severity (rate it 1-10). This mnemonic ensures you capture every dimension of the chief complaint. Follow with a targeted review of systems that explores related symptoms without consuming 20 minutes on unrelated body systems.
Step Two: Focused Physical Examination
Your history should guide which systems you examine. A patient with chest pain warrants cardiovascular, pulmonary, and musculoskeletal assessment. You do not need a full head-to-toe exam for every complaint. Focus yields better findings than rote completeness.
Step Three: Hypothesis Generation and Pre-Test Probability
Before ordering a single test, write down three to five possible diagnoses. Always include at least one life-threatening condition, even if you judge it unlikely. This forces you to consider the worst-case scenario and ensures you do not anchor prematurely on benign explanations. For each hypothesis, estimate its pre-test probability based on prevalence, patient risk factors, and clinical presentation. A 45-year-old with substernal chest pain radiating to the jaw has a higher pre-test probability of acute coronary syndrome than a 22-year-old with reproducible chest wall tenderness. These judgment calls become sharper with experience, and NPs working in high-acuity settings (such as those in an acute care nurse practitioner role) encounter these scenarios frequently.
Step Four: Test Ordering with Purpose
Order tests to confirm or rule out specific hypotheses, not to fish for unexpected findings. Ask yourself: will this test result change my management? If the answer is no, reconsider whether you need it. A negative D-dimer in a low-probability pulmonary embolism case helps rule out the diagnosis. The same test in a high-probability case adds little value because you will image regardless.
Worked Example: Chest Pain at 45
A 45-year-old male presents with 30 minutes of substernal chest pressure that started during yard work. Initial differential includes acute coronary syndrome (life-threatening, moderate pre-test probability), costochondritis (benign, possible), gastroesophageal reflux (common, less likely given exertional onset), and pulmonary embolism (life-threatening, lower probability without risk factors). Physical exam reveals diaphoresis and no chest wall tenderness. EKG and troponin become your first-line tests because they directly address the most dangerous hypothesis. The framework keeps you anchored to clinical reasoning rather than reflexive ordering.
Step Five: Iterative Narrowing
As test results return and symptoms evolve, revisit your list. Drop diagnoses that no longer fit. Add new ones if the clinical picture shifts. Differential diagnosis is a living process, not a one-time checkbox.
Questions to Ask Yourself
Essential Differential Diagnosis Mnemonics Every NP Should Know
Which differential diagnosis mnemonics are actually worth learning in NP practice?
The honest answer is: the ones that keep your thinking wide open when a patient's presentation does not fit a tidy pattern. Mnemonics are scaffolding, not a substitute for clinical reasoning. They exist to catch the category you almost skipped, the diagnosis you almost ruled out too early because it seemed unlikely. Used that way, they are genuinely powerful tools, especially in the first years of practice when your pattern recognition library is still growing.
The table below covers the mnemonics most commonly taught and applied in NP clinical education, with a note on when each earns its keep.
The Core Mnemonics at a Glance
| Mnemonic | What Each Letter Stands For | Best Used When |
|---|---|---|
| VINDICATE | Vascular, Infectious/Inflammatory, Neoplastic, Degenerative, Iatrogenic, Congenital, Autoimmune, Traumatic, Endocrine/Metabolic | Building a broad differential from scratch for almost any chief complaint |
| VITAMINS C+D | Vascular, Infection/Inflammatory, Trauma, Autoimmune/Allergic, Metabolic, Idiopathic/Iatrogenic, Neoplastic, Structural/Congenital, Congenital, Degenerative/Drug-related/Dietary | Systems-based differential building, particularly useful in primary care settings |
| OLDCARTS | Onset, Location, Duration, Character, Aggravating/Alleviating factors, Radiation, Timing, Severity | Structuring the history of present illness so no symptom detail gets missed |
| SOCRATES | Site, Onset, Character, Radiation, Associations, Time course, Exacerbating/relieving factors, Severity | Pain-focused history, especially useful in urgent care or undifferentiated pain presentations |
| OPQRST | Onset, Provocation/Palliation, Quality, Region/Radiation, Severity, Timing | Emergency and acute care settings; pairs naturally with SOCRATES for thorough pain workups |
| IMPASSIVE DICTATING | Immune reactions, Metabolic, Psychiatric, Allergic, Structural, Social, Infectious, Vascular, Endocrine/exocrine, Degenerative, Iatrogenic, Congenital, Traumatic, Autoimmune, Toxic, Idiopathic, Neoplastic, Genetic | Comprehensive differentials where social determinants, psychiatric causes, and genetic factors must be formally considered |
A Note on VINDICATED
An updated version of VINDICATE, sometimes written as VINDICATED, adds a closing prompt to examine race-based assumptions and diagnostic bias in your reasoning.1 Developed with structural competency in mind and referenced in AAMC literature, this extension is a practical reminder that the diagnostic process is not bias-free by default. Incorporating that final check does not slow you down; it makes your differential more accurate, not less.
How to Actually Use These in Your Workflow
In practice, most NPs do not run through every letter of every mnemonic for every patient. Instead, you reach for them selectively. OLDCARTS or OPQRST often shapes how you take the history. VINDICATE or VITAMINS C+D comes into play when you have finished the history and exam and you want to pressure-test your differential before anchoring on a diagnosis. IMPASSIVE DICTATING, published in a NIH-indexed clinical education journal, is especially helpful for complex, multi-system presentations where you suspect you might be missing a less obvious category, such as a toxic exposure, a social driver, or a psychiatric contributor.2 Many NPs also pair these frameworks with nurse practitioner tools like clinical decision-support apps to streamline the process at the point of care.
The goal is to move from scaffolding to intuition over time. Early in your NP career, leaning on these frameworks actively and explicitly, including during nurse practitioner clinical rotations, builds the mental habits that eventually become second nature. Do not rush past them in the name of efficiency; they are part of how efficiency gets built.
Common Chief Complaints and Their Key Differentials
The core tension when faced with a new chief complaint is knowing how wide to cast the differential net. Too narrow risks missing a life-threat, while too broad can lead to unnecessary testing and patient anxiety. The tables below offer a quick-reference starting point for eight of the most common NP chief complaints.1 They are not exhaustive lists; always tailor your differential to the individual patient's history and exam.
Chest Pain
- Differentials: Acute coronary syndrome; Stable angina; Costochondritis; GERD; Panic/anxiety.
- Red flag: New exertional chest pressure with radiation or diaphoresis, tearing pain (aortic dissection), or pleuritic pain with dyspnea and hypoxia (PE) requires immediate evaluation.2
Headache
- Differentials: Tension-type headache; Migraine; Medication-overuse headache; Sinusitis; Cervicogenic headache.
- Red flag: Thunderclap onset, new neurologic deficits, worst headache of life, or headache with exertion, fever, pregnancy, or jaw claudication in an older adult must prompt emergent imaging.
Abdominal Pain
- Differentials: Nonspecific/gastroenteritis; GERD/dyspepsia/PUD; IBS; Constipation; Biliary colic.
- Red flag: Signs of peritonitis, severe sudden pain, GI bleeding, suspected ectopic pregnancy, or abdominal aortic aneurysm demand immediate surgical or specialty evaluation.
Cough
- Differentials: Viral URI/acute bronchitis; Asthma; Post-nasal drip; GERD; Community-acquired pneumonia.
- Red flag: Respiratory distress, hypoxia, suspected PE, hemoptysis, or stridor with drooling signals a need for urgent intervention and possible referral.
Dyspnea
- Differentials: Asthma/COPD exacerbation; Heart failure; Pneumonia; Deconditioning/obesity/anxiety; Anemia.
- Red flag: Dyspnea at rest, hypoxia, unilateral pleuritic pain with decreased breath sounds, or acute heart failure signs should activate an emergency response immediately.
Fatigue
- Differentials: Depression/anxiety; Sleep disorders; Anemia; Endocrine disease; Chronic infections.
- Red flag: Unintentional weight loss, dyspnea/chest pain, lymphadenopathy, or abnormal vital signs with neurologic deficits warrant a broad workup and possible referral.
Low Back Pain
- Differentials: Nonspecific mechanical; Degenerative disc disease; Radiculopathy; Spinal stenosis; Sacroiliac pain.
- Red flag: Cauda equina syndrome (bowel/bladder dysfunction, saddle anesthesia), severe motor weakness, or history of cancer with new back pain requires immediate imaging and neurosurgical consultation.
Dizziness
- Differentials: BPPV; Vestibular neuritis; Meniere disease; Orthostatic hypotension; Generalized anxiety.
- Red flag: Focal neurologic deficits (posterior circulation stroke), new severe headache, inability to walk, vertical nystagmus, or associated chest pain/syncope: treat as a neurological emergency.
NPs working in online acute care nurse practitioner programs or emergency settings will encounter many of these chief complaints daily, making quick pattern recognition essential.
Can't-Miss Diagnoses and Red-Flag Checklists
Can't-miss diagnoses are time-sensitive conditions where delayed recognition leads to death, permanent disability, or serious harm. These include pulmonary embolism, myocardial infarction, ectopic pregnancy, meningitis, aortic dissection, stroke, subarachnoid hemorrhage, diabetic ketoacidosis, compartment syndrome, testicular torsion, appendicitis with perforation, and disseminated sepsis. The hallmark of safe practice is not diagnosing every rare disease, but consistently ruling out the most dangerous possibility before settling on a benign explanation.
As a new NP, train yourself to pause before finalizing every assessment and ask: What is the worst thing this could be? That single question transforms your diagnostic reasoning from pattern recognition into safety-first clinical judgment. You don't need to test for everything, but you do need to consciously consider and document why you excluded high-risk conditions.
Organizing Red Flags by Symptom Cluster
Rather than memorizing long lists of diseases, organize red flags by presenting complaint. This mirrors how patients actually arrive in your exam room and makes your mental checklist faster and more practical.
For headache, watch for thunderclap onset (seconds to minutes), fever with neck stiffness, new focal neurologic deficit, recent head trauma in anticoagulated patients, sudden severe pain unlike any prior headache, vision changes or papilledema, onset after age 50 with temporal tenderness, and headache that worsens with position change or Valsalva.
For chest pain, red flags include tearing or ripping quality radiating to the back, hemodynamic instability, unequal blood pressures in arms, acute dyspnea with unilateral leg swelling, pain worse with deep breath plus recent immobility, diaphoresis with nausea in a patient with cardiac risk factors, and radiation to jaw or left arm accompanied by exertional pattern.
For abdominal pain, consider ectopic pregnancy in any woman of reproductive age, rigid abdomen with rebound tenderness, pulsatile mass, sudden onset with syncope, pain out of proportion to exam findings (mesenteric ischemia), bloody diarrhea with hemodynamic compromise, and flank pain with fever (pyelonephritis or obstructed stone).
Population-Specific Can't-Miss Considerations
Certain populations require additional vigilance. In pediatrics, look for intussusception (currant-jelly stool, intermittent inconsolable crying, palpable abdominal mass), non-accidental trauma (bruising in non-ambulatory infants, inconsistent history, delayed care-seeking), sepsis (fever under 28 days of age is an emergency), and altered mental status (diabetic ketoacidosis, ingestion, shaken baby syndrome). NPs who focus on younger patients may also want to explore the differences between neonatal vs pediatric nurse practitioner roles.
Geriatric patients often present atypically. Myocardial infarction may manifest as confusion, fatigue, or syncope without chest pain. Pulmonary embolism can be silent or present only as delirium. Appendicitis may show minimal tenderness. Sepsis often presents with subtle changes in baseline function rather than fever or elevated white count. A lower threshold for testing and specialist consultation is warranted, and understanding the adult gerontology nurse practitioner scope of practice helps clarify when to escalate care.
In pregnancy, ectopic pregnancy must be ruled out in any first-trimester bleeding or abdominal pain. Preeclampsia requires blood pressure monitoring and symptom screening (headache, visual changes, right upper quadrant pain) at every visit after 20 weeks. HELLP syndrome can progress rapidly. Any pregnant patient with bleeding, severe headache, chest pain, or decreased fetal movement needs urgent evaluation, not reassurance alone.
Common Diagnostic Pitfalls New NPs Make (and How to Avoid Them)
Cognitive errors account for a significant share of diagnostic mistakes across all levels of clinical experience, but new NPs face a steeper uphill climb because they are still assembling the pattern library that seasoned providers have built over years of practice. Without that accumulated library, the brain reaches for mental shortcuts, and those shortcuts can lead you in the wrong direction.
Anchoring Bias
This happens when you latch onto the first reasonable explanation and stop looking. A classic NP scenario: a young woman presents with palpitations and a history of anxiety, and you anchor on anxiety without ordering thyroid labs. Weeks later, her hyperthyroidism is picked up by another provider. The fix is to build a habit of generating at least three diagnoses before committing to one, even when the first answer feels obvious.
Premature Closure
Closely related to anchoring, premature closure means you stop expanding your differential once you find a plausible explanation. You diagnose a middle-aged man with musculoskeletal chest pain after a normal EKG and send him home, without considering unstable angina or an aortic process. A structured diagnostic timeout, pausing to ask "what else could this be?" before finalizing your assessment, catches this error more often than intuition alone.
Availability Bias
Your brain overweights diagnoses you have seen recently or that made a strong impression. If you just saw a case of pulmonary embolism last week, you may over-order CT pulmonary angiograms on low-risk patients for the next month. Peer consultation is a practical corrective here. A colleague who was not at the bedside can offer a less emotionally colored read on the presentation.
Confirmation Bias
This is the tendency to notice exam findings that support your working diagnosis and minimize those that contradict it. You suspect appendicitis, so you focus on the right lower quadrant tenderness and gloss over the bilateral adnexal fullness that points toward ovarian pathology. Deliberately listing findings that do not fit your leading diagnosis forces you to confront contradictory evidence rather than filter it out.
Diagnosis Momentum
This pitfall is especially common during care transitions. A patient arrives in your clinic labeled with fibromyalgia by a prior provider, and that label travels through every subsequent visit without re-evaluation. The actual cause turns out to be small fiber neuropathy or an inflammatory arthritis. When you inherit a diagnosis, treat it as a hypothesis, not a fact. Review the original workup, ask whether the clinical picture still fits, and document your reasoning either way.
The unifying strategy across all five biases is a willingness to revisit your differential when test results do not match your expectations. Unexpected results are not inconveniences; they are the diagnostic process doing its job. Building these self-correction habits early, ideally during NP clinical placement, sets a foundation that will serve you throughout your career.
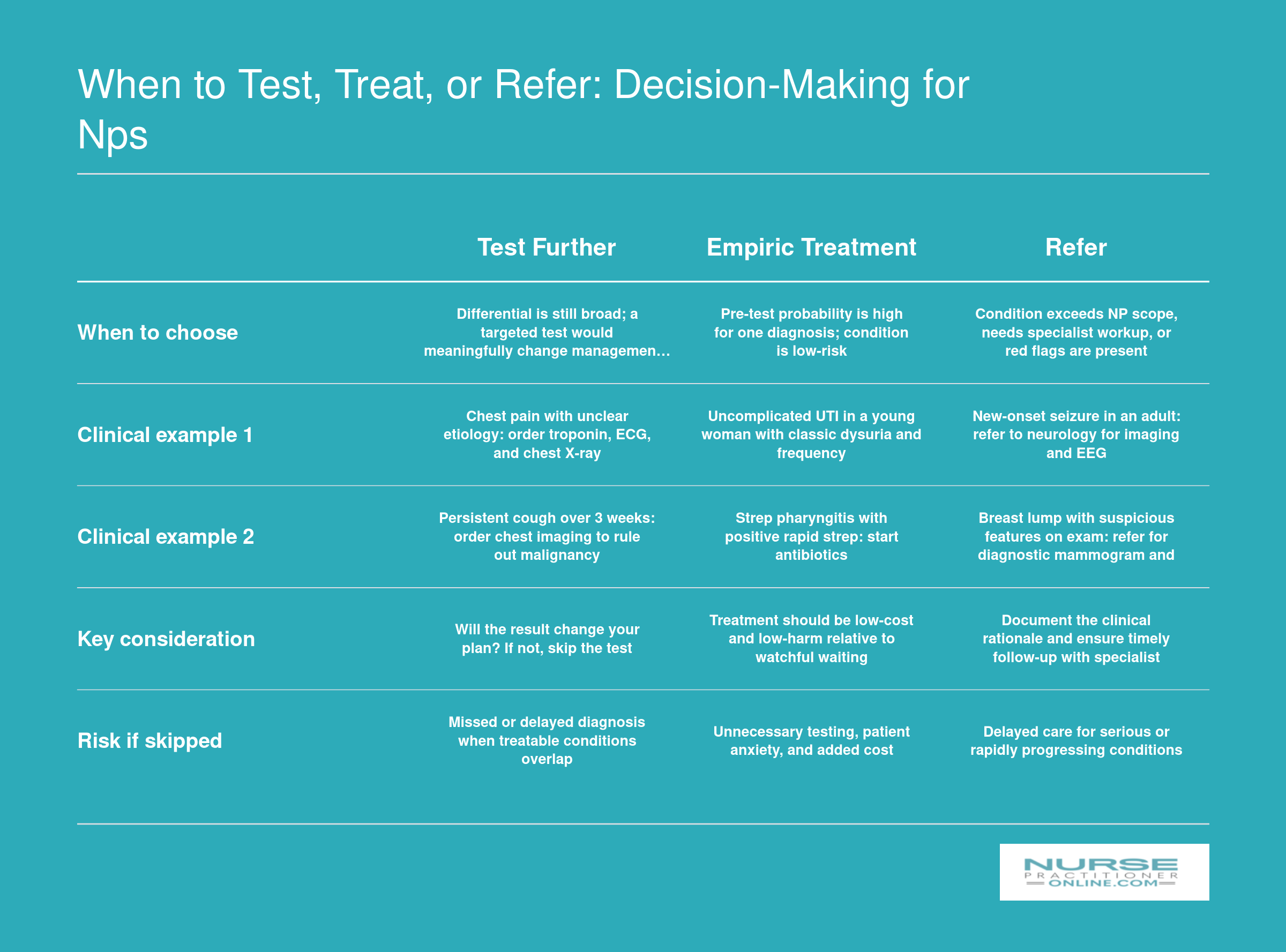
When to Test, Treat, or Refer: Decision-Making for NPs
Not every differential demands the same next step. When you have narrowed your list, the clinical priority shifts to action: should you order more diagnostics, start empiric treatment, or send the patient to a specialist? This three-path framework helps new NPs make that call efficiently and safely.
When to Test, Treat, or Refer: Practical Guidance for NPs
Test, treat, or refer: these three paths diverge at every clinical encounter, and choosing the right one is a skill refined with experience, evidence, and honest self-assessment. New NPs often struggle to decide when diagnostic workup is essential, when empiric therapy is prudent, and when specialty consultation is the safest next step. This section offers a practical framework grounded in professional standards and real-world clinical scenarios.
Testing: When to Order, When to Observe
Effective testing balances clinical suspicion against pre-test probability and the risk of harm. For example, when a patient presents with pleuritic chest pain and mild tachycardia, using the Wells criteria to stratify pulmonary embolism risk guides whether to order a D-dimer (for low-probability cases) or proceed directly to CT angiography (for higher-probability cases). Overuse of low-yield tests increases costs, anxiety, and false-positive results that trigger unnecessary downstream interventions. Underuse, however, can miss time-sensitive diagnoses. Asking yourself three questions before ordering helps: Does this test change management? What is the pre-test probability? What is the harm of waiting?
Treating Empirically: Confidence Without Certainty
Empiric treatment is appropriate when the clinical picture is straightforward and the benefit of immediate therapy outweighs the delay and cost of testing. A young woman with classic dysuria, frequency, and pyuria on dipstick can start nitrofurantoin for uncomplicated cystitis without waiting for culture results. Similarly, a child with obvious strep pharyngitis by modified Centor score may begin penicillin immediately. According to the AANP's standards, NPs are expected to recognize and manage common conditions within their competence independently.1 The key is pattern recognition paired with safety-netting: provide clear return precautions so patients know what symptoms should prompt re-evaluation. This independent management of common presentations is central to the role of a primary care nurse practitioner.
Referring: A Sign of Clinical Maturity
New NPs often fear that requesting a consult signals incompetence. In truth, appropriate referral demonstrates clinical maturity and commitment to patient safety. Professional standards from organizations including the College of Registered Nurses of Saskatchewan emphasize that NPs must recognize and work within the limits of their competence and refer as needed to ensure safe care.2 Refer promptly for new seizures, unexplained weight loss exceeding ten percent of body weight, suspected malignancy, or any finding that falls outside your training or comfort zone. Specialty referral guidelines, such as those published by Seattle Children's otolaryngology program, exist for many disciplines, and your collaborative physician or specialist colleagues expect timely consultation for complex or high-risk cases.
Managing Diagnostic Uncertainty with Safety-Netting
Not every differential resolves into a clear diagnosis at the first visit. When your differential includes only low-acuity possibilities and serious illness is unlikely, reassurance paired with safety-netting is a legitimate and evidence-based strategy.1 Safety-netting includes specifying what symptoms should prompt return (fever above 101.5, worsening pain, new confusion), the timeframe for expected improvement (within 48 to 72 hours), and an explicit invitation to return sooner if concerns arise. Document your reasoning, the differentials considered, the red flags excluded, and the safety-netting advice given. This approach reduces unnecessary testing while maintaining safety and trust.
Scope-of-Practice Awareness and Collaboration
Your legal authority to test, treat, and refer varies by state.3 Some states grant NPs full practice authority with independent referral rights, while others require collaboration or supervision agreements. For example, California's AB 890 law distinguishes categories of NP practice before granting full independence.4 Review your state's scope-of-practice statutes and your collaborative agreement (if applicable) to understand when physician involvement is legally required versus clinically advisable. Understanding nurse practitioner licensing requirements in your jurisdiction protects your license and your patients, and ensures you practice within the evidence and standards of care recognized by the profession.
Documenting Your Differential Diagnosis Correctly
Documenting your differential diagnosis means writing down the full list of possible conditions you considered for each patient, explaining why each made the list and how you narrowed it down, in a format that meets legal, billing, and quality-of-care standards. This documentation lives in the Assessment section of your SOAP note, where it serves as both a clinical roadmap and your most powerful legal defense if a diagnosis is questioned later.1 Vague or incomplete differential documentation is a common thread in NP malpractice cases, particularly when a serious condition was missed or treatment was delayed.2
Structure Your Assessment: Ranked Differentials with Reasoning
List your differential diagnoses in order from most to least likely, using clear clinical language rather than jargon or abbreviations that might confuse a chart reviewer.2 For each condition on your differential, include a brief statement of the clinical reasoning that placed it there. For example, in a patient presenting with chest pain, you might write: "Acute coronary syndrome (most likely given patient's age, hypertension, and exertional pattern of pain; EKG shows ST-segment changes). Gastroesophageal reflux disease (epigastric tenderness on exam, but pain radiates to jaw, less consistent). Musculoskeletal pain (no reproducible chest wall tenderness, low likelihood)."
This ranked, annotated structure demonstrates that you thought through the clinical picture systematically. It shows not only what you considered, but also how you weighed the evidence. In legal terms, it proves you met the standard of care by identifying serious diagnoses and evaluating them appropriately.3
Document What You Ruled Out and Why
When you exclude a diagnosis, especially a serious one, write down the specific findings or test results that led you to rule it out. If you considered pulmonary embolism but ruled it out based on a low Wells score, normal vital signs, and a negative D-dimer, document those exact details. If you considered meningitis but excluded it because of a normal neurological exam, absence of nuchal rigidity, and no fever, state that clearly.4 This protects you if a patient's condition evolves or if another provider later questions why a test was not ordered or a referral not made.
Ruled-out diagnoses are just as important as your final working diagnosis. They demonstrate thoroughness and help future providers understand your clinical thought process. In malpractice claims, the question is often not whether you reached the correct diagnosis immediately, but whether you considered and appropriately excluded dangerous alternatives. Documentation of negative findings is your evidence that you did.2
ICD-10 Coding: Code the Working Diagnosis, Not Every Differential
When it comes to billing and coding, assign ICD-10 codes only to the conditions you are actively treating or investigating, not to every item on your differential list.1 If your working diagnosis is acute bronchitis and you are treating it as such, code for acute bronchitis. If you are ordering tests to rule out pneumonia but have not yet confirmed it, you may code for signs and symptoms (such as cough or shortness of breath) or use a "suspected" code if appropriate under current guidelines. Do not code for diagnoses you have ruled out or conditions you listed only as remote possibilities.
However, in your narrative assessment, continue to document the full differential reasoning. The distinction is this: your narrative shows your clinical thinking and risk management, while your coded diagnoses reflect the conditions you are addressing with tests, treatments, or referrals. This separation protects both your reimbursement (by coding accurately) and your liability (by documenting comprehensively).
Risk Management: Your Documentation Is Your Best Defense
Thorough differential documentation is the single most effective malpractice protection available to NPs.2 Insurers and legal experts consistently emphasize that lawsuits succeed not because a diagnosis was difficult or atypical, but because the chart fails to show that the provider considered serious conditions. A vague assessment like "viral syndrome" or "upper respiratory infection" without any documented reasoning leaves you vulnerable. If the patient returns three days later with bacterial pneumonia or meningitis, a plaintiff's attorney will argue that you failed to consider those diagnoses at all.
In contrast, a chart that lists viral upper respiratory infection as the most likely diagnosis, but also documents consideration and appropriate exclusion of pneumonia, influenza, and strep pharyngitis based on exam findings and selected testing, demonstrates sound clinical reasoning even if the diagnosis later changes. The documentation proves you met the standard of care by thinking through the differential and making informed decisions.
EHR Tips: Use Templates Wisely, Avoid Copy-Forward Traps
Many electronic health record systems offer structured assessment templates that prompt you to list differentials and document reasoning. Use these tools, but customize them for each patient. Avoid the copy-forward function that carries yesterday's differential into today's note without updating it. A stale or irrelevant differential is worse than none at all because it suggests you did not actually reassess the patient.
If your EHR allows, create personal templates or dot phrases for common chief complaints that include prompts for key differentials and red-flag symptoms. For example, a chest pain template might prompt you to address cardiac, pulmonary, gastrointestinal, and musculoskeletal causes. Developing these habits during np clinical rotations helps ensure you consider the full range of possibilities in real time, not just when documenting afterward. Over time, these templates become embedded in your clinical workflow and reduce both cognitive load and documentation time.
Frequently Asked Questions About NP Differential Diagnosis
New nurse practitioners often have practical questions about how differential diagnosis works in day-to-day clinical practice. Below are clear, actionable answers to the most common questions NPs ask as they build confidence in diagnostic reasoning.
- Can a nurse practitioner diagnose a patient?
- Yes. Nurse practitioners are trained and legally authorized to diagnose patients, though the level of independent practice varies by state. In full-practice-authority states, NPs diagnose and treat without physician oversight. In reduced or restricted-practice states, NPs may need a collaborative agreement with a physician. Regardless of the model, NPs use the same evidence-based diagnostic reasoning process, including differential diagnosis, as other licensed providers.
- What are the steps of differential diagnosis for nurse practitioners?
- The core steps include gathering a thorough history, performing a focused physical exam, generating an initial list of possible diagnoses, prioritizing that list by probability and severity, ordering targeted diagnostic tests, narrowing the list based on results, and reassessing over time. Throughout this process, always consider life-threatening conditions first and use clinical reasoning frameworks to stay systematic rather than relying on pattern recognition alone.
- What mnemonics help NPs build a differential diagnosis?
- Several mnemonics are widely used. VINDICATE (Vascular, Infectious, Neoplastic, Degenerative, Iatrogenic, Congenital, Autoimmune, Traumatic, Endocrine) helps organize etiologies by category. OLDCARTS (Onset, Location, Duration, Character, Aggravating factors, Relieving factors, Timing, Severity) guides symptom history-taking. SOCRATES is another option for pain assessment. Choose one or two that feel natural and practice them consistently until they become second nature.
- What are the most common diagnostic errors new NPs make?
- The most frequent pitfalls include anchoring bias, which means locking onto a diagnosis too early, premature closure of the differential list, skipping a thorough review of systems, relying too heavily on pattern recognition before building experience, and failing to consider serious or uncommon conditions. New NPs can reduce these errors by using structured frameworks, seeking feedback from colleagues, and making it a habit to ask, "What else could this be?"
- How do you document a differential diagnosis in a patient chart?
- List your working diagnoses in order of clinical likelihood, with the most probable condition first. For each diagnosis on the list, briefly note the supporting and opposing evidence from the history, exam, or test results. Include your clinical reasoning for the plan you chose. This documentation protects you legally, supports continuity of care, and demonstrates the medical decision-making complexity required for accurate billing.
- When should an NP refer a patient to a specialist instead of treating?
- Refer when the presentation falls outside your scope of training or experience, when initial treatment fails to produce improvement within an expected timeframe, when diagnostic findings suggest a condition requiring specialized procedures or management, or when red-flag symptoms indicate a potentially life-threatening process. A timely referral is a sign of strong clinical judgment, not a limitation. Always document your reasoning for the referral in the patient's chart.