Most important takeaways…
- Redesigning scheduling templates to match actual NP visit types is the highest-impact, lowest-cost workflow project you can start.
- Team-based rooming and pre-visit planning shift data gathering to support staff, freeing 5 to 10 minutes per encounter for clinical decisions.
- EHR optimization projects can cut after-hours documentation time by 20 to 30 percent, reclaiming one or more hours each day.
- Structured chronic care visit protocols and small outcome metric sets turn any of these projects into a defensible DNP capstone.
How do you shave 20 minutes off your daily charting when you are already seeing 18 to 22 patients and your MA keeps getting pulled for phone triage?
Nurse practitioners in primary care face a compounding problem: patient panels are growing, but the documentation burden, inbox volume, and scope-of-practice constraints that shape small-practice workflows have not eased. Unlike physicians in larger systems, many NPs work without dedicated scribes, advanced practice support staff, or the scheduling autonomy to build in buffer time. The result is a daily grind of late lunches, after-hours notes, and the nagging sense that something has to give.
Four focused quality improvement projects can change that reality. Each one targets a specific bottleneck, offers a realistic timeline, and delivers metrics you can track. Just as important, leading QI work positions you for nurse practitioner advancement opportunities and the salary premiums that come with them.
How to Design an NP-Focused Quality Improvement Project
The tension between wanting meaningful practice change and feeling overwhelmed by research methodology stops many nurse practitioners from ever launching a quality improvement project. The good news: you do not need a complex study design or a hospital-based team. A focused, well-structured project in your own primary care clinic can improve patient flow, reduce your daily stress, and even serve as a DNP capstone with only minor adaptation.
The PDSA Cycle, Translated for Primary Care
PDSA stands for Plan-Do-Study-Act, and it is the backbone of most quality improvement work. In a primary care setting, it works like this:
- Plan: Identify one workflow problem (for example, visits consistently running 15 minutes behind by mid-morning) and propose a specific change to address it.
- Do: Test that change on a small scale, perhaps with one provider's panel for a single week.
- Study: Collect data during and after the test. Did visit cycle times decrease? Did patient satisfaction hold steady?
- Act: Based on what you learned, adopt the change, modify it, or try something different.
The beauty of PDSA in an NP-run clinic is speed. You are not waiting on a hospital committee to approve a unit-wide rollout. You can test a scheduling tweak on Monday, review the data on Friday, and refine it the following week. Most successful primary care QI projects run through two or three PDSA cycles before landing on a sustainable solution.
Shadow Your Own Clinic Day First
Before you design any intervention, you need a clear picture of where time actually goes. Spend one or two days logging your workflow with simple timestamps. Track these categories:
- Rooming and intake (from the moment you enter the exam room to the start of your clinical assessment)
- Direct patient interaction (history, exam, counseling, shared decision-making)
- Documentation (charting during and after the visit)
- Inbox and administrative tasks (results review, refill requests, prior authorizations, patient portal messages)
- Transition time (walking between rooms, pulling up the next chart, informal hallway conversations)
You can use a small notebook, a spreadsheet on your phone, or even voice memos. Certain nurse practitioner apps can make time-tracking even easier if you prefer a digital approach. The goal is not perfection; it is pattern recognition. Most NPs who do this exercise discover that one category consumes a disproportionate share of their day, and that category becomes the target for your project.
A Realistic 12-Week Implementation Timeline
Quality improvement projects thrive on structure. A 12-week timeline keeps the work manageable alongside a full clinical schedule:
- Weeks 1 to 2: Collect baseline data. Log the metric you plan to improve (visit cycle time, documentation minutes per encounter, inbox hours per day) across at least 10 clinic sessions.
- Weeks 3 to 4: Design your intervention. Use what you learned from shadowing and baseline data to create a specific, testable change. Write it down in one or two sentences so every team member understands it.
- Weeks 5 to 10: Pilot the intervention. Run two or three PDSA cycles, adjusting after each one. Keep collecting data in the same format you used at baseline.
- Weeks 11 to 12: Measure outcomes against your baseline and decide whether to adopt, adapt, or abandon the change.
This timeline fits neatly into a single academic quarter, which matters if you are pursuing a DNP.
Pick One Metric and Protect It
The single most common mistake in QI work is trying to measure everything. When you track too many outcomes, you dilute your focus and make it harder to draw clear conclusions. Before you start, commit to one primary metric. Good options for primary care NP projects include:
- Average visit cycle time (patient arrival to checkout)
- Minutes of documentation per encounter
- Third-next-available appointment slot (a standard access measure)
- Percentage of visits that start within five minutes of the scheduled time
You can track secondary metrics if you want context, but your project lives or dies on that single primary number.
Connecting to DNP Capstone Work
Each of the four projects covered in this article (scheduling redesign, team-based rooming, EHR optimization, and chronic care visit streamlining) can serve as a DNP scholarly project with minor modifications. The key additions are a formal literature review, a theoretical framework such as Lewin's Change Theory or the Model for Improvement, and IRB determination (most clinic-based QI projects qualify for exemption). If you are enrolled in or considering an online DNP program, designing your capstone around a real workflow problem in your own practice means you graduate with a project that already improved your daily life, not a binder that sits on a shelf. For those still exploring program options, our guide on how to enroll in NP school online walks through the application process step by step.
Primary Care Visit Cycle: Where NPs Lose Time
Before you can fix your workflow, you need to see where the minutes actually go. These benchmarks, drawn from national survey data, reveal the pressure points most primary care NPs share. Use them as a baseline when you design your own quality improvement project.

Project 1: Redesign Scheduling Templates for NP Panels
Scheduling template redesign is often the highest-impact, lowest-cost quality improvement project an NP can lead. When your template does not reflect the actual work you do, every day becomes a scramble of overruns, delayed patients, and charting that bleeds into evening hours. A well-designed template aligns slot length with visit complexity, protects time for same-day acute needs, and distributes demanding encounters so you are not running on empty by 2 p.m.
Step 1: Audit Your Current Template
Before changing anything, collect baseline data for two to four weeks. Pull a report from your practice management system or manually tally:
- Visit types: Count acute, follow-up, annual physicals, chronic care, and telehealth encounters per day.
- Slot length vs. actual time: Compare scheduled slot duration with real start-to-finish encounter time, including documentation.
- No-show and same-day cancellation rates: Note which visit types have the highest gaps.
- Session overruns: Track how often you finish more than 15 minutes past your scheduled end time.
This audit reveals mismatches.1 You may discover that 15-minute follow-up slots routinely take 22 minutes, or that acute visits cluster unpredictably because patients cannot get same-day appointments.
Step 2: Build a Mixed-Capacity Template
Evidence-informed scheduling models recommend reserving 50 to 60 percent of daily slots as open-access appointments for same-day or next-day needs.2 That sounds aggressive, but open-access designs consistently reduce no-show rates and improve patient access.3 Within that framework, consider the following structure:
- Reserve 20 to 30 percent of daily slots specifically for same-day acute visits.
- Schedule two to three telehealth-only blocks per day, ideally for stable chronic care check-ins or medication refill reviews.
- Stagger complex chronic care visits so no more than two appear back-to-back. A diabetic foot exam followed immediately by a comprehensive geriatric assessment drains cognitive reserves and pushes the rest of the day late.
- Keep your appointment type menu simple. Too many categories confuse schedulers and fragment your day.3
Step 3: Assess Panel Size Sustainability
No universal benchmark exists for NP panel size, but primary care literature suggests panels of 1,200 to 1,800 patients are generally sustainable for full-time providers, depending on patient acuity and team support.4 Calculate your active panel by identifying patients seen at least once in the past 18 months. Your assigned panel may be larger, but inactive patients rarely drive daily demand. If your active panel exceeds sustainable thresholds and you lack team support, template redesign alone will not solve your workflow problems. You may need to advocate for panel redistribution or additional staffing, and that can mean navigating difficult conversations with difficult patients and administrators alike.
Step 4: Test with a PDSA Cycle
A six-week Plan-Do-Study-Act timeline keeps the project manageable:
- Week 1: Complete slot audit and calculate baseline metrics including no-show rate, third-next-available appointment, and session overruns.
- Week 2: Redesign template on paper. Experiment with different configurations before building in your scheduling system.
- Weeks 3 through 6: Pilot the new template. Track in-times and out-times for each session. Review data weekly.
- End of Week 6: Compare metrics to baseline. Adjust slot lengths or visit-type distribution based on findings.
What Success Looks Like
Consider a hypothetical NP clinic using uniform 20-minute slots for all visit types. Acute visits pile up on the nurse triage line because no same-day openings exist, and complex chronic care appointments run 10 minutes over, cascading delays through the afternoon. After switching to a mixed template with 25 percent same-day acute slots, variable slot lengths, and staggered chronic care, the clinic saw a 15 percent reduction in no-shows and measurably improved same-day access within one quarter.6 Providers finished on time more often, and patient satisfaction scores climbed.
Scheduling redesign is not glamorous, but it is foundational. Fix the template first, and every other workflow improvement becomes easier to sustain.
Questions to Ask Yourself
Project 2: Implement Team-Based Rooming and Pre-Visit Planning
The way primary care practices structure the time before an NP walks into an exam room is one of the most underutilized levers for improving daily throughput. Shifting clinical tasks to the right team member at the right moment does not dilute care quality. Research consistently shows that team-based models improve adherence to chronic disease protocols and raise clinical quality measures across the board.1
Define Who Does What Before the Door Opens
The goal of team-based rooming is straightforward: by the time the NP steps in, the clinical groundwork is already done. Think of the visit as a relay, not a solo sprint.
A well-run NP-MA-RN triad assigns tasks like this:
- Medical assistant: Records vitals, reconciles the current medication list, administers standing-order screenings, and flags any pending lab results before the NP arrives.
- RN (where available): Addresses open care gaps, administers vaccines, and handles care coordination tasks that require nursing judgment.
- NP: Focuses entirely on clinical decision-making, differential diagnosis, and the therapeutic relationship with the patient.
This delineation is not about cutting corners. It is about ensuring that each credential is working at its highest level. NPs already deliver outcomes equal to or better than physicians in primary care settings, so the real question is whether their time is being spent on tasks that match their training.2
Standing Orders: The Engine That Makes It Work
MA standing orders are the mechanism that allows medical assistants to perform screenings before the NP is in the room. Even in states with restrictive NP practice environments, NPs can draft and authorize these orders. A few concrete examples:
- Point-of-care A1c for patients with a diabetes diagnosis on the schedule
- PHQ-9 depression screen during annual wellness visits
- Urine dipstick for any patient presenting with UTI symptoms
- Blood pressure re-check protocol for patients with hypertension on the panel
With standing orders in place, the NP reviews results rather than waiting for them. Studies confirm that standing orders in primary care lead to higher vaccination rates and more consistent preventive screening.3
Pre-Visit Planning the Day Before
One of the highest-yield habits in team-based primary care is a daily pre-visit planning review. The afternoon before, an MA or RN pulls up the next day's schedule and flags overdue labs, expired specialist referrals, and open preventive care gaps. Research on pre-visit planning and team huddles consistently finds that this practice is one of the most reliable ways to close chronic and preventive care gaps without extending visit length.1
When the NP opens the chart at 8 a.m., the groundwork is already visible. There is no real-time detective work. Having the right nurse practitioner tools in place, from EHR templates to panel management dashboards, makes this step even faster.
Before and After: A Realistic Timeline
Consider a small primary care practice that tracked rooming time before and after introducing MA standing orders and a pre-visit planning protocol. Average rooming time dropped from roughly 12 minutes to about 7 minutes per visit. Across a full clinic day, that freed more than 30 minutes of NP time, time that could be redirected toward complex patients or simply toward ending the day closer to on schedule.4
If you want to replicate that result, use this PDSA structure:
- Week 1: Baseline observation. Time rooming from patient check-in to NP entry. Note where delays cluster.
- Weeks 2 to 3: Draft standing orders and build the pre-visit planning checklist. Train MAs on new workflow steps.
- Weeks 4 to 8: Pilot the new process with a subset of the panel or a single clinic day.
- Weeks 9 to 10: Pull the data. Compare rooming time, care gap closure rates, and any staff feedback before deciding whether to expand.
Both the American Academy of Family Physicians and the National Academies of Sciences, Engineering, and Medicine identify standardized pre-visit planning and robust team-based rooming as core components of high-functioning primary care.34 This project translates that evidence directly into a workflow any NP-led practice can implement.
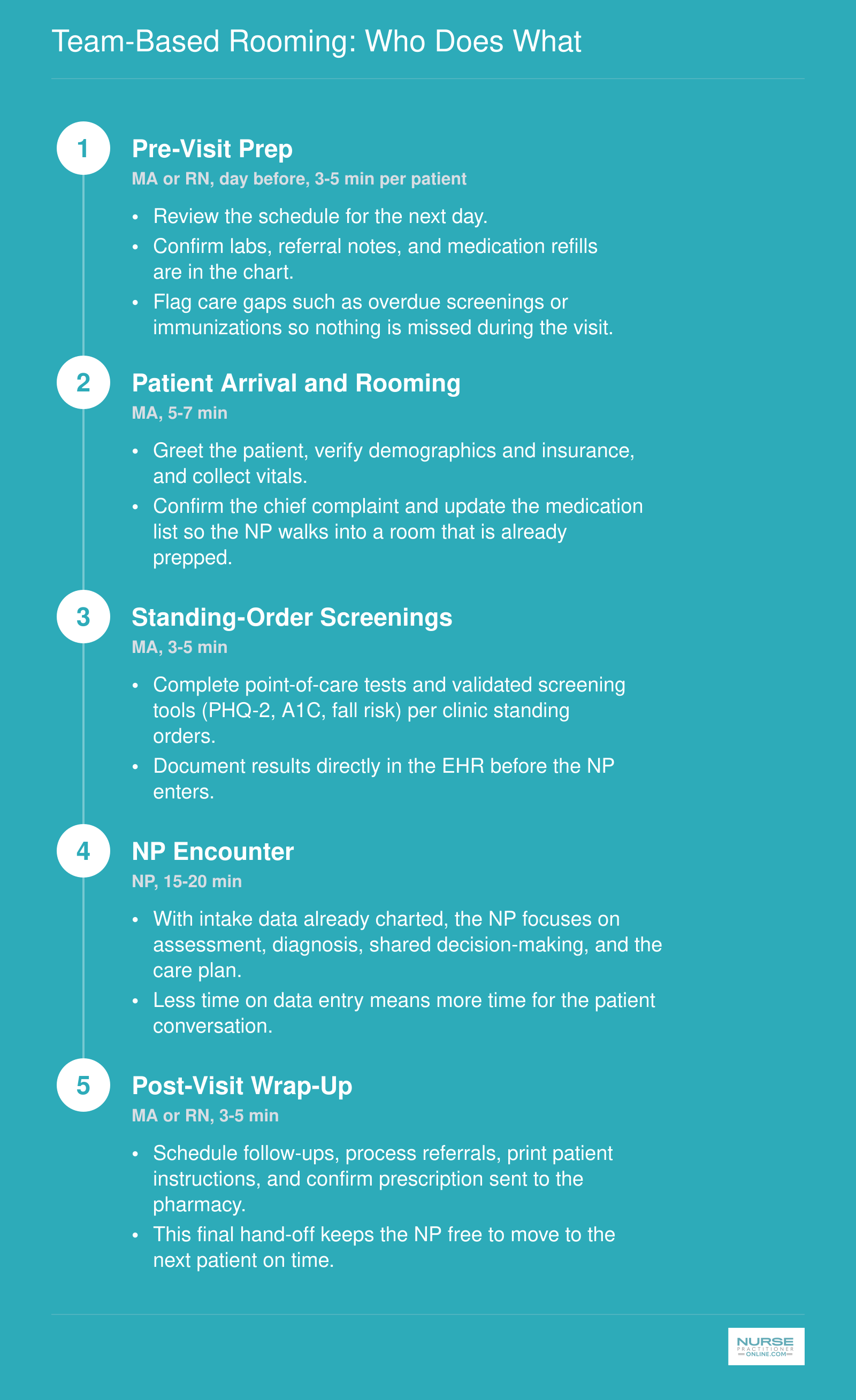
Team-Based Rooming: Who Does What
A well-designed rooming workflow spreads the workload across your team so the NP can focus on clinical decision-making rather than data gathering. Here is a practical five-step sequence you can adapt to your own clinic.
Project 3: Optimize EHR Documentation Workflows
Primary care clinicians spend roughly 1.5 to 2 hours on after-hours EHR work each day, and well-designed optimization projects have been shown to cut that time by 20 to 30 percent.1 For NPs, that recovered time is the difference between charting at your kid's soccer game and being present for it.
Build Visit-Type-Specific Templates
Generic SOAP templates force you to write every note from scratch. Condition-specific templates flip the work: you edit pre-populated content instead of generating it. Build templates for your top 10 visit types, including diabetes follow-up, hypertension recheck, well-child checks, acute upper respiratory infection, depression follow-up, and Medicare annual wellness visits. Each template should pre-populate the assessment and plan with evidence-based defaults (for diabetes: A1C trend statement, medication review prompt, foot exam documentation, retinopathy screening status) that you tweak rather than type.
The goal is realistic: reduce documentation time from 15 to 16 minutes per encounter to 10 to 12 minutes within a 10-week pilot. That is roughly 90 minutes saved across a 20-patient day.
Use Dot Phrases Strategically
Smart phrases (dot phrases in Epic, auto-text in Cerner) save 2 to 3 minutes per note when used well. Start with these five:
- .normalexam: a complete normal physical exam by system that you delete findings from rather than build up
- .diabetesap: a structured assessment and plan block for stable type 2 diabetes
- .htneduc: a patient education paragraph on lifestyle modification for hypertension
- .avssummary: a templated after-visit summary with medication changes, follow-up timing, and warning signs
- .referralpcp: a referral letter skeleton with HPI, relevant labs, and the specific question you want answered
Tier Your Inbox
Inbox work consumes 1 to 2 hours daily for most primary care providers, and most of those messages do not need an NP's clinical judgment.1 Build a tiered triage protocol with your team:
- Medical assistants handle routine prescription refill requests that match a standing protocol and normal lab results with patient letters
- RNs handle abnormal-but-not-urgent results, patient symptom questions within their scope, and prior auth follow-ups
- The NP only sees results requiring a clinical decision, new symptoms, or messages flagged by the team
A centralized team inbox, rather than a personal queue, makes this delegation visible and accountable.1
Standardize Refills
Write standing refill protocols for stable chronic medications (statins, antihypertensives, metformin, levothyroxine, SSRIs at unchanged doses) tied to up-to-date labs and visit intervals. The MA or RN processes refills against the protocol, and you approve batches once or twice daily instead of clicking through individual requests. Most NPs reclaim 30 to 45 minutes a day with this change alone.
Project 4: Streamline Chronic Care Management Visits
Chronic care is where the tension between thorough and timely hits hardest: a 20-minute slot has to cover a foot exam, a med reconciliation, a goal-setting conversation, and the labs that should have been drawn before the patient ever sat down. The fix is not working faster. It is removing the decisions you should not be making at the visit at all.
Standardize the Visit for Diabetes and Hypertension
Start with the two conditions that fill most NP panels. Build a one-page visit checklist for each. For type 2 diabetes, the visit anchors are: A1c result reviewed, blood pressure recorded, foot exam documented, medication reconciliation, retinal screening status, and one concrete behavior goal set with the patient. For hypertension, the anchors are: in-office BP with proper cuff technique, home BP log reviewed, medication adherence assessed, sodium and lifestyle counseling noted, and titration decision documented. When every NP and MA in the practice works from the same checklist, variation drops and gaps close.1
Use Standing Orders So Labs Are Ready Before You Walk In
Standing order sets let the MA act on protocol without waiting for your signature. Typical rules: A1c every 3 months if the last value was above 7%, annual lipid panel, annual urine albumin-to-creatinine ratio, retinal screening referral if not done in the past year. The MA orders, draws, or schedules these as part of rooming. You walk in with results in hand instead of ordering labs the patient has to come back for.
Close the Loop Between Visits
The visit is one touchpoint. The other 89 days matter more. Assign your MA or RN to call patients two weeks after any medication change, track no-shows for chronic care visits and rebook them within a week, and review patient portal BP or glucose logs asynchronously. For Medicare patients with two or more chronic conditions, the Chronic Care Management benefit reimburses for at least 20 minutes of non-face-to-face care coordination per month, which funds this work.2
What the Numbers Look Like
NP-led chronic care redesign projects in the literature commonly move A1c control rates from a 30 to 50% baseline up to 50 to 70% post-intervention, with mean A1c reductions of 0.5 to 1.5 percentage points.1 Hypertension control gains of 10 to 20 percentage points are realistic over 6 to 18 months. One practice published moving diabetes control (A1c under 9%) from 65% to 80% in six months using exactly this combination: standardized visit templates, standing orders, and structured between-visit outreach.1
A 12-Week PDSA Timeline
- Weeks 1-2: Chart audit. Pull 30 to 50 charts per condition and document where current care falls short of the checklist.
- Weeks 3-4: Build the visit template, the standing order set, and the MA rooming script. Get sign-off from your medical director and lab.
- Weeks 5-10: Pilot with one condition (pick diabetes or hypertension, not both). Meet weekly with the care team to surface friction.
- Weeks 11-12: Re-audit the same metrics, compare to baseline, and decide whether to spread to the second condition or refine first.
Pick the condition where your control rates are furthest from the HEDIS benchmark. That is where a tight workflow buys you the most ground.
Measuring Outcomes: Metrics That Prove Your Project Works
Measuring outcomes means choosing a small set of numbers that tell you, in concrete terms, whether your quality improvement project actually changed something for the better. Without baseline data and a clear target, even the most thoughtful workflow redesign is just a hunch. Here is how to select, source, and track the metrics that matter most for primary care office flow.
Operational Metrics: Time and Access
Start with the metrics your patients and staff feel every day.
- Visit cycle time: This is the total minutes from patient check-in to checkout. The Medical Group Management Association (MGMA) publishes annual survey data with national medians for primary care. Use these benchmarks to set a realistic target, such as reducing your average cycle time by 10 to 15 percent.
- Documentation time per encounter: If your EHR optimization project is working, you should see clinician charting time drop. The MGMA and the American Academy of Family Physicians (AAFP) practice management resources both offer comparison data for documentation burden.
- No-show rate: National primary care no-show rates typically hover around 15 to 20 percent, though your panel may differ. Track this monthly to see whether scheduling template changes are keeping patients engaged.
- Same-day access rate: Can a patient who calls in the morning get seen that day? As of 2026, roughly 62 percent of patients nationally report inadequate access to timely primary care, and 76 percent wait more than 10 minutes past their appointment time.1 Even modest improvements here signal a real win.
Patient Experience Metrics
Patient satisfaction scores give you the "how did it feel" side of your data story. Press Ganey and CG-CAHPS are the two most widely used instruments in primary care. CG-CAHPS results for many practices are publicly available through the Centers for Medicare and Medicaid Services (CMS) comparison websites. Practice-specific or specialty-specific percentile breakdowns often require a subscription or organizational membership, but the publicly posted data still provides a useful reference point.
Clinical Quality Benchmarks
If your project touches chronic care management, tie your outcomes to established clinical measures. The role of the primary care nurse practitioner is central to these efforts, because NPs often manage the bulk of chronic disease panels in smaller practices.
- Diabetes A1c control: The National Committee for Quality Assurance (NCQA) publishes national percentiles in its Quality Compass reports, and the CDC's National Diabetes Statistics Report offers population-level targets.
- Hypertension blood pressure control: NCQA HEDIS measures and the CDC's Million Hearts initiative both set clear benchmarks. Tracking the percentage of your hypertensive panel at goal before and after workflow changes gives you a clinically meaningful outcome.
Research shows that chronic disease patients who have a usual source of care are 20 percent less likely to be hospitalized and 11 percent less likely to visit the emergency department, reinforcing why continuity-focused workflow improvements carry real clinical weight.2
Where to Find Free Benchmarks
Not every practice can afford paid databases. If your organization lacks access to MGMA or NCQA subscriptions, you still have options. State health department reports, Medicare claims analyses through the CMS Chronic Conditions Data Warehouse, and peer-reviewed studies indexed in PubMed frequently cite national averages drawn from these authoritative sources. A useful starting point is published research on primary care flow improvement, which often contains benchmarks you can reference without a paywall.3
Putting It All Together
Pick three to five metrics that align directly with the project you chose. Collect at least four weeks of baseline data before you implement changes, then track the same numbers weekly for at least one full PDSA cycle. When you can show, for example, that your scheduling redesign cut average cycle time by 12 percent and raised same-day access from 40 to 55 percent, you have evidence that speaks to administrators, colleagues, and accreditation reviewers alike. That kind of data also strengthens a DNP scholarly project or a portfolio for QI leadership roles down the road.
DNP Project Ideas Connected to Primary Care Workflow
Tackling a workflow bottleneck as a staff-driven improvement is one thing. Elevating that same problem into a rigorous Doctor of Nursing Practice capstone project is another, and the difference lies in the framework you wrap around the intervention. Each of the four projects outlined in this guide can become a publishable DNP scholarly project when you layer in a structured evidence review, formal Plan-Do-Study-Act cycles with documented data collection, institutional review board approval when required, and statistical analysis that quantifies the impact. That shift from informal improvement to formal scholarship positions you as a thought leader and opens doors to clinical leadership roles and higher compensation. If you are weighing whether the degree itself makes sense, exploring whether a DNP is worth it can help you decide before committing to a capstone.
Turning the Four Core Projects into DNP Capstones
Redesigning scheduling templates for nurse practitioner panels becomes a capstone when you define a pre-post study design, pull baseline access metrics from your EHR, implement the new template, measure same-day appointment availability and patient wait times at 4, 8, and 12 weeks, and compare the results using paired t-tests or control charts. Team-based rooming can be framed as an intervention to reduce rooming time and improve vital-sign documentation completeness, with process mapping before and after, staff time studies, and patient satisfaction surveys as your outcome measures. Optimizing EHR documentation workflows might focus on reducing average note completion time or after-hours inbox work, tracked through EHR audit logs and validated by provider self-report. Streamlining chronic care management visits lends itself to a study of billing code capture, patient activation scores, and clinician time per visit.
Four Additional DNP Project Ideas for Primary Care
- Patient portal adoption to reduce phone call volume: Measure baseline call volume to the triage line, implement a targeted education campaign encouraging portal messaging for refills and test results, and track the shift from synchronous phone calls to asynchronous portal messages over 12 weeks. Published DNP projects have demonstrated that online direct-scheduling platforms reduce staff time on phone scheduling and increase the proportion of appointments booked via the platform.1
- Group visit models for chronic disease education: Design a shared medical appointment protocol for diabetes or hypertension, co-facilitated by an NP and a medical assistant, and measure hemoglobin A1c or blood pressure control, patient activation, and per-patient visit time compared to individual visits.
- Medical assistant competency training programs for expanded rooming roles: Develop a structured curriculum that teaches MAs to complete medication reconciliation, enter standing orders for preventive screenings, and pre-chart chronic disease flowsheets. Measure rooming time, documentation accuracy, and NP satisfaction before and after training.
- Telehealth triage protocols for after-hours concerns: Create standardized decision trees that empower triage nurses to offer video visits for low-acuity concerns outside business hours. Track the proportion of after-hours calls that convert to telehealth visits instead of emergency department referrals, patient satisfaction, and provider workload.
Published DNP capstones in ambulatory care have tested tele-work nurse staffing models that improve productivity and patient throughput, implemented mental health screening workflows that boost screening rates and provider compliance, and embedded advance care planning into oncology clinics with measurable increases in documented conversations and appropriate billing.2
Practical Advice for Choosing and Executing Your Project
Start with your own clinic's most visible pain point. If your team complains daily about the triage phone ringing off the hook, portal adoption is your lever. If you personally stay late three nights a week closing notes, EHR workflow optimization is the project. Secure preceptor and site-leader buy-in early by framing the project as solving a real operational problem, not just fulfilling a degree requirement. Choose a project with a measurable outcome you can track in 8 to 12 weeks, because DNP timelines are tight and you need enough cycles to demonstrate sustained change. Avoid sprawling multi-site interventions or projects that depend on hospital IT releasing new software.
Nurse practitioners who lead published quality improvement projects position themselves for clinical leadership roles, get invited to speak at conferences, and command higher compensation because they have demonstrated the ability to diagnose system problems and implement evidence-based solutions at scale. Completing a DNP capstone is also a powerful way to unlock nurse practitioner advancement opportunities beyond direct patient care. Your DNP project is not just a graduation hurdle. It is a portfolio piece that proves you can lead change.
Nurse Practitioner Salary and Career Growth Through QI Leadership
Quality improvement leadership can be a meaningful catalyst for career advancement and higher compensation. The table below presents national salary benchmarks for nurse practitioners based on Bureau of Labor Statistics data from 2024. NPs who step into practice improvement roles, such as clinical director or operations lead positions, often command compensation at or above the 75th percentile, reflecting the added value of workflow optimization and organizational leadership skills.
| Metric | Value |
|---|---|
| Total National Employment | 307,390 |
| Median Annual Salary | $129,210 |
| 25th Percentile Annual Salary | $109,940 |
| 75th Percentile Annual Salary | $149,570 |
| Mean Annual Salary | $132,000 |
Common Questions About NP Quality Improvement Projects
Quality improvement can feel overwhelming when you are already juggling a full patient panel. These answers cut through the jargon and give you practical starting points you can apply in your own clinic.
- What is the PDSA cycle in nursing quality improvement?
- PDSA stands for Plan, Do, Study, Act. You plan a small change (for example, adding a pre-visit lab protocol), test it on a limited number of patients, study whether wait times or outcomes improved, then decide to adopt, adjust, or abandon the change. It is designed for rapid, low-risk testing so you can refine a workflow before rolling it out clinic-wide. Most primary care QI teams run multiple PDSA cycles over 8 to 12 weeks.
- What are examples of quality improvement projects in nursing?
- Common projects include redesigning scheduling templates to match visit complexity, implementing team-based rooming protocols, optimizing EHR documentation with dot phrases and smart sets, and streamlining chronic care management visits with standing order sets. Other examples are reducing no-show rates through automated reminder systems, creating standardized diabetic foot exam workflows, and launching same-day prescription refill protocols. Each project should target a specific, measurable outcome such as cycle time or patient satisfaction scores.
- How do you improve patient flow in a primary care office?
- Start by mapping each step of a typical visit, from check-in to checkout, and time every handoff. Then target the longest delays. Staggering appointment types (acute versus chronic), empowering MAs to complete intake tasks before the NP enters the room, and batching EHR inbox work into set blocks all reduce bottlenecks. Tracking door-to-door cycle time weekly helps you see whether changes are actually working or need another round of adjustment.
- What procedures can an FNP perform?
- Family nurse practitioners commonly perform skin biopsies, joint injections, incision and drainage, suturing, splinting, IUD and Nexplanon insertions, and point-of-care ultrasound in primary care settings. Scope of practice varies by state, so always check your state board's regulations. Adding procedural time slots to your schedule can boost revenue, reduce referrals, and give patients faster access to care, all of which improve overall office flow.
- How can nurse practitioners reduce documentation burden?
- Build a personal library of EHR dot phrases, smart sets, and order panels tailored to your most frequent visit types. Delegate pre-charting of vitals, medication reconciliation, and health maintenance alerts to trained support staff. Schedule two or three dedicated inbox management blocks per day instead of responding in real time between patients. Voice-to-text tools and AI-assisted note drafting are also gaining traction in 2026 and can cut charting time by 20 to 30 percent for many NPs.
- What are good DNP project ideas for primary care?
- Look for a recurring pain point in your clinic that has measurable data. Strong DNP project topics include implementing a depression screening and follow-up protocol using the PHQ-9, reducing A1C recheck lag time for diabetic patients, piloting a nurse-led transitions-of-care call program to cut 30-day readmissions, and creating a hypertension management pathway using home blood pressure monitoring. Choose a project where you can collect baseline data quickly and complete at least three PDSA cycles within your program timeline.
Four projects, one starting point. Pick the single workflow problem costing you the most time right now, whether that is a misaligned scheduling template, a chaotic rooming process, an EHR inbox that never empties, or a chronic care visit that routinely runs over.
Spend the first two weeks collecting baseline data using the metrics covered earlier in this article. That number gives you something to improve against. A 10 percent reduction in visit cycle time or after-hours documentation, modest on its own, compounds quickly: across a full week of patient care, it can return an hour or more to your day. You do not need to overhaul everything at once. If your project sparks interest in a DNP capstone, reviewing DNP prerequisites now saves time later. Start Monday with one project, one metric, and two weeks of honest observation. The rest follows from there.