Most important takeaways…
- Structured nurse-family collaboration from admission through bereavement reduces preventable crisis calls and boosts caregiver satisfaction.
- CMS mandates hospice interdisciplinary team meetings at least every 15 days, making the nurse the essential coordinator across disciplines.
- NHPCO caregiver curricula cover symptom management, safety, and emotional support so nurses can standardize family training at home.
- Over 51 percent of Medicare decedents enrolled in hospice care, underscoring the growing need for strong family partnerships.
How much of hospice care is actually delivered by professionals? Less than you might expect. Family caregivers provide roughly 70 to 80 percent of total care hours for patients receiving hospice at home, handling everything from medication administration to repositioning and emotional support.
That reality makes nurse-family collaboration a clinical necessity, not a courtesy. Yet the tension is persistent: families report feeling underprepared for the hands-on demands of end-of-life caregiving, while nurses operate under visit schedules that compress teaching and assessment into narrow windows. Both sides feel the gap, and research consistently ties that gap to preventable symptom crises and higher caregiver distress.
Closing it requires more than goodwill. Structured communication protocols, competency-based caregiver training, and genuine interdisciplinary coordination are the mechanisms that turn a well-meaning relationship into a functioning partnership.
Hospice Vs. Palliative Care: Key Differences Every Nurse Should Know
The single biggest barrier to timely hospice enrollment is confusion about the difference between hospice and palliative care, and that confusion starts long before families call an agency. When families hear "hospice," they often think it means giving up, when in fact palliative care has been part of the treatment plan all along. Understanding these distinctions helps you guide families through enrollment conversations with clarity instead of fear.
When Care Begins: Diagnosis vs. Terminal Prognosis
Palliative care can start the day a patient receives a serious diagnosis, whether that's heart failure, COPD, cancer, or dementia. It runs alongside curative or disease-modifying treatment. The patient may still be receiving chemotherapy, dialysis, or other interventions aimed at slowing disease progression. The palliative care nurse practitioner on the team focuses on symptom management, care coordination, and quality of life while the primary team pursues treatment.
Hospice, by contrast, requires a physician's certification that the patient has a terminal prognosis of six months or less if the disease follows its expected course.1 Enrollment means the patient has chosen comfort-focused care instead of curative treatment. That shift in goals is the defining line, not the diagnosis itself.
What Medicare Covers Under the Hospice Benefit
The Medicare Hospice Benefit covers a comprehensive package that families often don't realize exists until you explain it. Medicare pays for all hospice services related to the terminal diagnosis, including nursing care through intermittent home visits with 24/7 on-call availability, medications for symptom control, durable medical equipment, social work, chaplain services, and volunteer support.2 An interdisciplinary team is required by regulation, so families get coordinated care, not fragmented visits.3
Caregiver education is included in the benefit without separate billing.3 You teach families how to manage symptoms, reposition for comfort, administer medications, and recognize changes. These are often difficult conversations, but they build confidence and reduce crisis calls. Bereavement counseling is also covered, both before and after the patient's death, typically for up to 13 months.2 Respite care is available when family caregivers need a break: Medicare covers up to five days of inpatient respite per episode, with a 5 percent coinsurance.3 Home-based respite is not currently covered, though the Hospice CARE Act has proposed adding it.4
Why Misunderstanding Delays Enrollment
Families resist hospice when they think it means "nothing more can be done." In reality, hospice is an intensive intervention. It brings a team into the home, provides supplies and medications, and offers training and round-the-clock support. When you clarify that palliative care has likely been part of the plan already and that hospice simply focuses those services on comfort rather than cure, resistance often softens. Setting accurate expectations from day one prevents the crisis enrollments that leave families underprepared and overwhelmed.
A Step-By-Step Framework for Nurse-Family Collaboration: Admission Through Bereavement
Hospice agencies that invest in structured family collaboration frameworks from the moment of admission see a measurable drop in preventable crisis calls.1 Research consistently shows that partnership quality at admission predicts caregiver satisfaction later, and families who feel heard and prepared are less likely to call in panic when symptoms escalate.2 The following five-phase framework draws on best-practice guidelines from the NHPCO and the Clinical Practice Guidelines for Quality Palliative Care, as well as the ELNEC family engagement model.3
Phase 1: Pre-Admission Orientation
Before the first home visit, the admissions nurse sets expectations. The nurse explains what hospice provides, clarifies the difference between hospice and palliative care, and listens to the family's priorities and fears. This phase is about planting trust.
- Nurse responsibilities: Provide clear, plain-language information about the hospice benefit, services, and what to expect. Assess family understanding of the illness and any immediate needs. Gather information on cultural or religious preferences.
- Family role: Ask questions, voice concerns, and identify who will be the primary caregiver(s). Share past experiences with healthcare that might shape expectations.
Phase 2: First 48-Hour Assessment and Trust-Building
The first two days are when relationships solidify. The nurse conducts a comprehensive family-inclusive assessment, covering the patient's condition, symptoms, and goals of care. This is not just a clinical intake; it is a conversation that builds the partnership.
- Nurse responsibilities: Perform a holistic assessment using the NHPCO-identified domains (needs, burden, understanding of illness).4 Discuss prognosis honestly and gently. Introduce the interdisciplinary team and explain each role. Teach the family immediate care skills (e.g., positioning, skin care) using the ELNEC teach-back method.
- Family role: Share day-to-day observations about the patient's comfort and preferences. Begin learning hands-on care with nurse guidance. Voice any emotional or logistical worries so the nurse can tailor support.
Phase 3: Ongoing Care Coordination (Weeks 1 to 4)
This phase is about rhythm. The nurse schedules regular visits and family conferences to reassess goals and symptoms. Collaboration here prevents crises and builds family confidence.
- Nurse responsibilities: Reassess symptoms and adjust the care plan proactively. Facilitate scheduled family conferences with interdisciplinary input. Use plain-language teach-back to ensure family understands medication changes or new symptoms. Act as a liaison, sharing family insights with the team.
- Family role: Report subtle changes in the patient's status that may signal decline. Practice new caregiving skills and ask for help when unsure. Participate in care planning discussions, advocating for the patient's comfort priorities.
Phase 4: Active Dying Support
As death nears, the partnership intensifies. Families often feel overwhelmed, and this is a time when dealing with difficult family members in healthcare situations requires extra empathy. The nurse provides rapid updates, intensified symptom management, and clear anticipatory guidance.
- Nurse responsibilities: Give frequent condition updates and explain what to expect in the final hours. Intensify comfort measures and coach family on supportive presence. Validate emotions and normalize grieving. Coordinate with the team for 24/7 backup.
- Family role: Focus on being present, not perfect. Follow the nurse's guidance to manage fears about breathing changes or restlessness. Accept emotional support and delegate tasks to other relatives if possible.
Phase 5: Bereavement Follow-Up
The partnership does not end at death. Immediate support and a warm handoff to bereavement services reduce long-term distress. The HPNA 2023 to 2026 Research Agenda emphasizes risk-based follow-up through bereavement, organized around the Griggs 2020 multi-level framework.6
- Nurse responsibilities: Provide emotional first aid at the time of death. Conduct a risk assessment for complicated grief. Facilitate a warm handoff to the bereavement team, sharing what the family has been through.
- Family role: Accept initial bereavement resources and name a point person for follow-up. Share their experience if they wish; it helps the care team serve future families better.
This five-phase, bilateral model turns family caregivers from spectators into skilled and supported partners. When both sides know their roles, the journey is less frightening, and the final days are more peaceful.
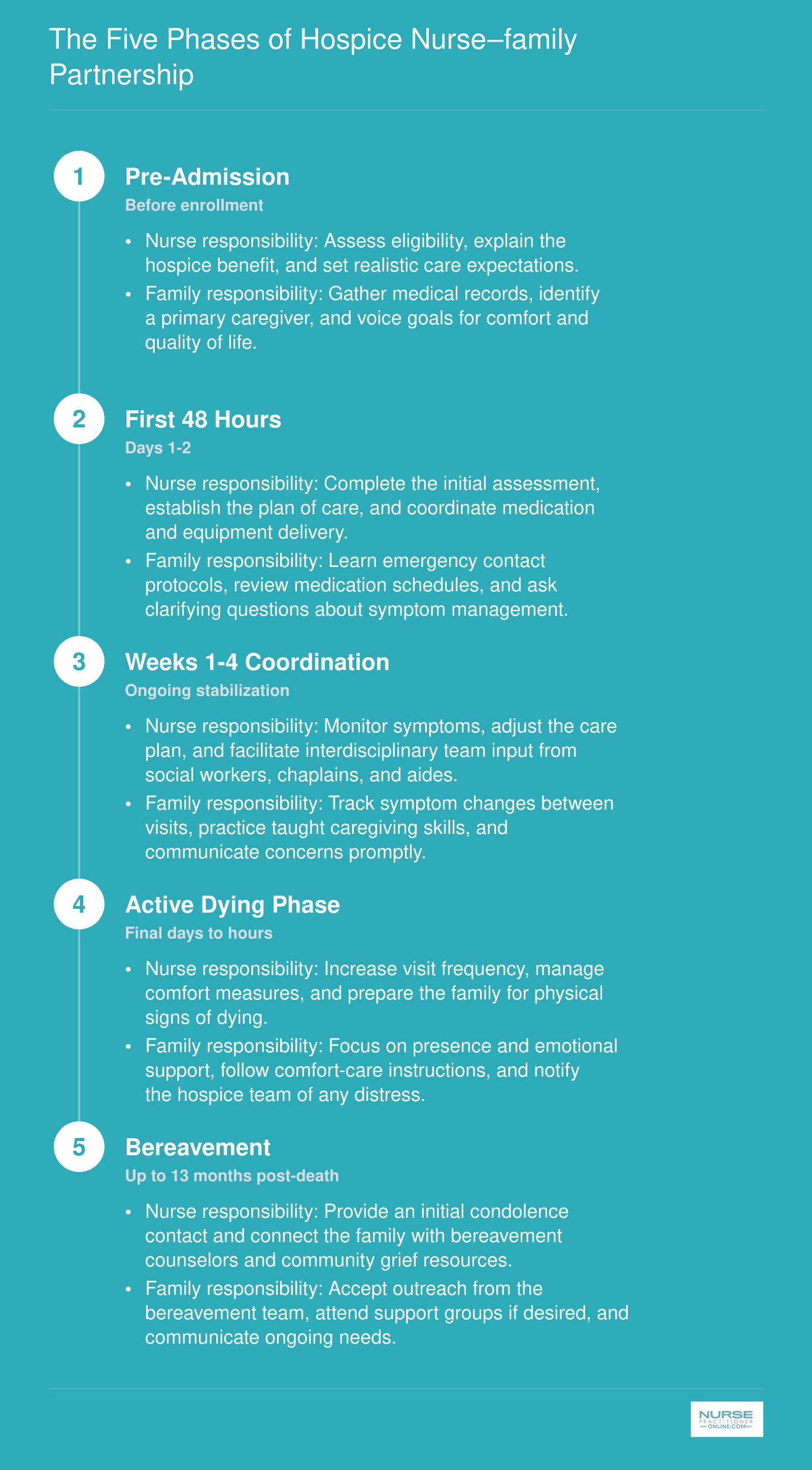
The Five Phases of Hospice Nurse–family Partnership
Use this framework as a quick reference for every hospice admission. Each phase pairs a core nurse responsibility with a corresponding family responsibility so both sides stay aligned from the first contact through bereavement support.
Communication Tools and Family Meeting Strategies That Actually Work
Clear communication in hospice is not a soft skill. It is the clinical scaffolding that prevents crises and preserves trust. When families have structured, predictable conversations with their nurse, their understanding of the care plan deepens, their anxiety drops, and the patient's final days align more closely with what they actually wanted.
SBAR for the Living Room: Adapting a Hospital Tool for Hospice Families
SBAR (Situation, Background, Assessment, Recommendation) originated as a safety tool for rapid nurse-to-physician handoffs, but hospice teams have reshaped it for emotional, high-stakes family talks.1 The goal shifts from getting a quick order to building shared meaning. In practice, that means:
- Situation: Frame what the family is observing right this week, e.g., "You've noticed Mom is sleeping more and eating less."
- Background: Briefly recap the illness trajectory and what has been tried, avoiding jargon. Connect the dots between the disease and the current change.
- Assessment: Name what you, as the nurse, see clinically *and* the family's stated worry. "Her breathing pattern tells me she is comfortable, and I hear that you're scared she's suffering."
- Recommendation: Offer one or two next steps (medication adjustment, a chaplain visit, a family conference) and ask, "Does this feel right to you?"
This adaptation, modeled after the Palliative and End of Life Care Multidisciplinary SBAR tool, keeps the conversation anchored in the person's goals of care and chosen location of death while leaving room for silence and tears.2
The 7-Step Family Meeting Agenda That Prevents Chaos
When a hospice nurse calls a formal family conference, a clear agenda turns a potentially volatile gathering into a productive planning session.3 Use this evidence-informed sequence:
1. Pre-meeting huddle (5 min): Clarify purpose, review clinical status, and decide who absolutely must be present: patient, key decision-makers, social worker, chaplain if needed. 2. Opening ground-setting (2 min): Thank everyone for coming. State the meeting's aim plainly: "We're here to make sure we're all on the same page about Dad's comfort plan." 3. Assess understanding (5 min): Ask each participant, "What is your understanding of what's happening right now?" Listen for gaps. 4. Share medical information (5-10 min): Keep it simple. "Here's what we're seeing... Here's what it likely means for the next days or weeks." 5. Explore values and goals (10 min): "What does a good day look like for him right now? What are you most worried about?" Write down key phrases. 6. Align recommendations and check understanding (5 min): Offer your clinical recommendation tied directly to their stated goals. Ask: "Did I explain that clearly? Can you put it in your own words?" 7. Summarize and plan follow-up (5 min): Hand everyone a bulleted, plain-language action plan covering who does what by when, and schedule the next check-in.
Documentation should capture both the medical facts and the emotional currents, without clinical shorthand that could confuse a later reader.4
Two Communication Models Worth Adopting Tomorrow
Beyond the family meeting structure, two validated frameworks give nurses portable scripts:
- Serious Illness Conversation Guide (Ariadne Labs): A one-page checklist that walks you through the conversation in seven steps. It starts with "I'd like to talk about what lies ahead" and includes the crucial "I wish… I worry… I wonder…" prompts that surface hidden hopes and fears. Many hospice agencies train nurses to use it during every care planning update.
- COMFORT Model: A holistic communication curriculum built on Connect (build rapport), Options (offer real choices), Meaning (explore what gives the patient purpose), Family (involve them as care partners), Openings (notice emotional cues), Relating (show genuine empathy), and Team (collaborate across roles). Nurses can apply the "C" and "O" immediately in any hallway or bedside chat.
While formal comparative trials remain sparse, hospice CAHPS scores and quality improvement data show that structured, multi-modal communication (phone, video, written summaries) increases family satisfaction.5 A practical operations tool like the Family Caregiver Communication Checklist, which standardizes admission education, ongoing updates, crisis protocols, and bereavement follow-up, helps ensure no family falls through the cracks.6 Nurses interested in nursing quality improvement projects will find that embedding these communication protocols into everyday workflows is one of the highest-impact changes a hospice team can make.
Regular Rhythms, Not Fire Drills
The biggest mistake is waiting for a crisis to call a family meeting. Predictable intervals (every two weeks for stable patients, weekly during active decline, and within 24 hours of any care setting transition) give families a container they can trust. When they know the nurse will sit down with them on a Tuesday afternoon no matter what, they save their urgent questions for that sacred space, and the squall of panicked phone calls quiets. That predictability is itself a therapeutic intervention, and it also goes a long way toward preventing nurse practitioner burnout by reducing the reactive chaos that drains hospice teams.
Questions to Ask Yourself
Caregiver Training: What Hospice Nurses Teach Families at Home
Building a Foundation with Established Curricula
As a hospice nurse, you don't have to design caregiver education from scratch. The National Hospice and Palliative Care Organization (NHPCO) offers a comprehensive "Caregiving Essentials" curriculum that covers symptom management, safety, and emotional support. This ready-to-use material aligns with industry standards and can be adapted to individual family needs. For more in-depth professional development, the American Academy of Hospice and Palliative Medicine (AAHPM) provides targeted training resources, including modules on communication and family dynamics. Nurses interested in deepening their expertise in this specialty may also explore adult gerontology nurse practitioner programs, which often include coursework relevant to end-of-life care. Tapping into these established programs ensures that your teaching is both evidence-based and consistent with best practices.
Evidence-Based Teaching: The Teach-Back Method
One of the most effective strategies for caregiver training is the teach-back method. Rather than simply explaining a task, you ask the caregiver to repeat the information in their own words or demonstrate the skill. This immediate feedback reveals gaps in understanding and reinforces learning. To explore the latest research on this approach in hospice settings, search PubMed or other academic databases using keywords like "teach-back hospice caregiver" and filter for studies published from 2022 to 2026. You'll find evidence on how teach-back improves medication management, pain assessment, and confidence among family caregivers. Incorporating this method into your training routine makes your teaching stick and reduces follow-up crises.
Assessing Caregiver Readiness
Before you dive into instruction, it helps to gauge a caregiver's starting point. The Preparedness for Caregiving Scale is a validated tool that measures how ready a family member feels to take on caregiving tasks, from physical care to emotional coping. You can locate the scale and studies on its effectiveness through academic publishers like Springer or Elsevier. Using such an assessment early in the admission process allows you to tailor your training to the caregiver's specific concerns and avoid overwhelming them. It also provides a baseline to measure progress over time, which can be reassuring for both you and the family.
Regulatory and Employer Expectations
Home hospice care is subject to regulations that often outline minimal caregiver training requirements. For an overview of occupational standards and state-specific mandates, visit the Bureau of Labor Statistics (BLS.gov) and your state's health department website. These resources can clarify what training hospice agencies are expected to provide and how it intersects with nursing licensure. While they won't give you a script for each teachable moment, they help you understand the legal framework so you can document your instruction appropriately and advocate for resources when needed.
Core Caregiver Training Checklist for Hospice Nurses
This checklist is designed as a practical, printable tool that hospice nurses can adapt for each family they train. Organize teaching sessions by domain, demonstrate each skill clearly, and confirm caregiver competency before moving on. Tailor the pace and language to the family's comfort level, and revisit skills as the patient's condition changes.
| Training Domain | Specific Skill | Teaching Method | Competency Check |
|---|---|---|---|
| Medication Management | Administering oral and sublingual medications on schedule | Nurse demonstration followed by supervised return demonstration | Caregiver correctly prepares and gives a dose while nurse observes |
| Medication Management | Recognizing and reporting side effects or adverse reactions | Teach back using a printed side effect reference card | Caregiver identifies at least three warning signs and explains when to call the hospice team |
| Symptom Monitoring | Assessing pain using a simple rating scale (e.g., 0 to 10) | Role play scenarios with the nurse guiding the caregiver through assessment | Caregiver accurately rates pain in two practice scenarios and documents findings |
| Symptom Monitoring | Monitoring for changes in breathing patterns, skin color, and level of consciousness | Bedside coaching during a routine visit with visual reference guides | Caregiver describes key changes to watch for and when to contact the nurse |
| Personal Care | Safe repositioning and turning to prevent pressure injuries | Hands on practice at bedside with proper body mechanics coaching | Caregiver demonstrates a safe two person or one person turn without prompting |
| Personal Care | Mouth care, skin hygiene, and toileting assistance | Step by step walkthrough with caregiver performing each task under supervision | Caregiver completes full personal care routine independently while nurse observes |
| Emergency Planning | Knowing when to call the hospice team versus 911 | Review of the hospice emergency protocol card and discussion of common scenarios | Caregiver correctly categorizes three example situations as hospice call or 911 call |
| Emergency Planning | Managing a comfort crisis (breakthrough pain, acute anxiety, respiratory distress) | Guided simulation using the patient's current comfort kit medications | Caregiver walks through the crisis protocol step by step and identifies correct medication and dose |
| Emotional and Spiritual Support | Recognizing signs of caregiver burnout and knowing how to request respite care | Supportive conversation with printed self care resource list | Caregiver verbalizes at least two personal warning signs and describes how to access respite services |
| Emotional and Spiritual Support | Providing presence and comfort during active dying | Nurse led discussion of what to expect, paired with a written guide on the signs of approaching death | Caregiver expresses understanding of the dying process and identifies comfort measures they feel prepared to offer |
Interdisciplinary Team Roles in Hospice Partnerships
CMS requires hospice interdisciplinary groups to meet at least every 15 days, aligning with bi-weekly reassessments that drive the plan of care.1 That regulatory floor is designed to keep every discipline tightly coordinated, but the real impact on families comes from how each team member functions day to day and how the nurse knits those functions together.
The Core IDT: Who Does What
- RN case manager: The family's primary clinical partner. The nurse assesses symptom changes, adjusts the care plan, teaches hands-on care, and translates medical complexity into language the family can act on.
- Hospice aide: Provides personal care (bathing, grooming, positioning) and spends more bedside time than anyone else. The aide is often the first to notice subtle changes and reports them directly to the nurse.
- Social worker: Addresses emotional, financial, and logistical needs. This includes advance directives, funeral planning, community resources, and family dynamics that affect care.
- Chaplain: Offers spiritual support individualized to the patient and family, whether that means prayer, ritual, legacy work, or simply a non-judgmental listening presence. A chaplain is not there to impose religious beliefs.
- Attending physician or hospice medical director: Certifies terminal prognosis, oversees medical direction, and collaborates with the nurse on complex symptom management decisions.
- Bereavement counselor: Provides grief support to the family for up to 13 months following the death, often beginning contact before the loss to build trust.
The Nurse as the Family's Primary Coordinator
Every discipline reports observations and concerns back to the RN case manager. The nurse holds the clinical picture, understands the family's stated goals, and decides when to escalate to the physician, bring in the social worker for a family meeting, or request an additional aide visit. When a family member asks a question no one seems to have answered, the nurse is the person who chases down the response and makes sure it lands in language the family understands. That quarterback role means nurses must know exactly what each team member can and cannot do, so referrals are precise and families stay confident. Nurses interested in deepening expertise in this area may consider pursuing a hospice nurse practitioner pathway.
Clearing Up Common Role-Confusion Situations
Families often misdirect requests because they do not understand the scope of each role. Three scenarios surface repeatedly:
- Asking the hospice aide to change medications: Aides cannot adjust, start, or stop any medication. The nurse teaches families to report symptoms and medication concerns directly to the RN, never to the aide, and explains that the aide's role is to observe and communicate.
- Expecting the chaplain to be religious: Some families assume spiritual care means pushing a specific faith. The nurse clarifies early that the chaplain meets patients and families wherever they are, whether secular, spiritual but not religious, or deeply faith-based, and that the family sets the agenda.
- Treating the social worker as only a benefits coordinator: While social workers do help with finances and resources, their core work is emotional support and counseling. Nurses encourage families to lean into the social worker's relationship for coping strategies, not just paperwork.
Proactive expectation-setting at admission and during the first several visits prevents these misunderstandings from becoming friction points.
How IDT Meetings Drive the Care Plan
Bi-weekly IDT meetings are structured case reviews that examine current goals, symptom status, risk factors, and upcoming transitions.2 Under the latest regulatory framework, families and caregivers are encouraged to participate, either by joining a portion of the meeting directly, through pre-meeting conversations with the nurse, or via post-meeting written summaries.3 The nurse brings the family's voice to the table, often quoting the family's own words when presenting goals. A plan of care update is triggered not just by the calendar but by real-life events: a crisis, rapid decline, new symptom burden, or admission to a facility.1 Patient and family goals must be documented in the family's own words and mapped to care plan elements, and each goal is assigned to a responsible discipline so accountability is clear.1 By keeping this process visible and actionable, the IDT meets the standards CMS reinforces through the Hospice Quality Reporting Program's patient and family experience domains.4
Technology and Resources That Strengthen Hospice Collaboration
Digital communication tools and telehealth platforms have transformed hospice care from a series of intermittent in-person visits into a continuous, responsive partnership between nurses and families. The right technology extends the reach of the hospice team without replacing the essential human connection at the bedside.
Telehealth for After-Hours Triage and Symptom Management
Video visits now serve as a critical bridge between scheduled in-person encounters, particularly for urgent symptom changes that do not require an emergency department visit. A 2024 randomized trial enrolling 1,250 patients with advanced lung cancer found that palliative video visits (4.7 per patient) delivered outcomes equivalent to in-person consultations (4.9 visits per patient), with patient satisfaction scores averaging 8.9 out of 10 and caregiver satisfaction at 8.8 out of 10.12 In rural and remote hospice populations, 67 percent of families reported satisfaction specifically related to reduced travel burden.2
The Consolidated Appropriations Act of 2026 explicitly extended Medicare coverage for telehealth services delivered by hospice physicians and nurse practitioner tools, formalizing flexibilities that originated during the COVID pandemic.3 Federal studies of hospice face-to-face recertification visits found no statistically significant difference in reauthorization decisions whether the encounter occurred via telehealth or in person.4 This evidence base supports using video for triage, medication adjustments, and family teaching while reserving in-person visits for comprehensive assessments, hands-on symptom management, and moments when physical presence matters most.
Patient Portals and Secure Messaging Platforms
Secure messaging keeps families informed between visits without the friction of phone tag. Leading hospice EHR platforms, including Homecare Homebase, Netsmart, MatrixCare Hospice, AlayaCare, Axxess Hospice, and WellSky Hospice, now offer patient and caregiver portal features that display medication schedules, care plan updates, visit summaries, and educational resources.2 Families can report symptoms through structured questionnaires, and nurses can review trends before the next visit.
Specialized telehealth programs such as Health Recovery Solutions' palliative care suite combine video visits with daily symptom self-reporting and caregiver-submitted observations, creating a longitudinal data stream that alerts the hospice team to subtle changes before they become crises.5 This continuous monitoring model reduces unnecessary hospitalizations while giving families confidence that their observations are seen and valued.6
Community Resource Mapping and Coordination Tools
Technology also strengthens the logistical scaffolding around hospice care. Many hospice agencies now maintain digital resource directories that nurses can search and share during family meetings, connecting caregivers with respite care vouchers, disease-specific support groups (both virtual and local), durable medical equipment vendors, and financial assistance programs. Some EHR systems integrate directly with community resource platforms, allowing nurses to generate personalized resource packets that reflect a family's ZIP code, language preference, and specific needs. This proactive mapping ensures that families do not have to navigate a fragmented social service landscape alone, particularly during the intense early weeks of hospice enrollment when caregiving demands are highest.
Cultural Considerations and Special Populations in Hospice Partnerships
Hospice teams are being asked to serve more linguistically and culturally diverse families than ever, yet most clinical training still leans on a checklist model of cultural competence rather than the cultural humility framework that organizations like the Center to Advance Palliative Care now recommend.1 The shift matters because end-of-life decisions sit at the intersection of faith, family hierarchy, and deeply personal beliefs about suffering, and no nurse can memorize her way to fluency in all of them.
Cultural Beliefs That Shape Family Participation
Cultural worldview influences who speaks, who decides, and what interventions families will accept. Federal hospice regulations already require non-discrimination and mandate that bereavement assessments account for social, spiritual, and cultural factors.2 A few patterns hospice nurses encounter regularly:
- Collectivist decision-making: In many Latino, South Asian, Middle Eastern, and East Asian families, the eldest son, a family council, or a designated spokesperson, rather than the patient alone, leads care conversations. Pushing for individual patient autonomy can feel disrespectful and erode trust.
- Faith-based concerns about opioids: Some families worry that morphine will hasten death or cloud the mind during prayer or final rites. Walking through dosing, sedation thresholds, and spiritual implications, ideally alongside a chaplain, often resolves the hesitation.
- Skepticism toward hospice itself: In communities with histories of medical mistreatment, including many Black American families, enrolling in hospice can feel like the system giving up. Slower pacing, transparent goals-of-care discussions, and continuity with one trusted clinician help.
The practical move is humility: ask what the family believes about a good death, who should be in the room for decisions, and what rituals matter, rather than assuming based on surname or zip code. Best-practice guidelines recommend documenting family roles and preferred communication styles at admission.2
Language Access and Informed Consent
Professional medical interpreters, in person or by video, should be the default for admission, consent, medication teaching, and goals-of-care meetings. Bilingual family members are appropriate for casual conversation but should not interpret clinical content: they may soften prognosis, omit distressing details, or lack the medical vocabulary to convey dosing instructions accurately. Document the language used and the interpreter ID for every consent encounter.2
Three Special Populations Worth Naming
- Pediatric hospice: Parents become primary caregivers while grieving in real time. Expect anticipatory grief, marital strain, and complex sibling dynamics, and build in extra psychosocial support.
- Dementia patients: Decision-making shifts to a surrogate, often a spouse or adult child carrying guilt about prior choices. Revisit goals of care as the disease progresses, and remember that spiritual counseling must align with the patient's and family's stated preferences.2
- Rural families: Limited access to in-person chaplains, social workers, and respite care means nurses lean harder on telehealth and community partners, including faith congregations and local volunteer networks. Nurses interested in broadening their role in underserved settings may explore nurse practitioner advancement opportunities to expand their clinical scope.
According to NHPCO Facts and Figures 2024 Edition, more than half of Medicare decedents, about 51.6 percent, enrolled in hospice care. For the most current caregiver burden and preparedness data, the NHPCO website, the NAC/AARP Caregiving in the U.S. report, and BLS.gov are your best starting points.
Frequently Asked Questions About Hospice Nurse–family Collaboration
These are some of the most common questions nurses and family caregivers ask about building effective hospice partnerships. Each answer offers a concise overview, and you can explore the corresponding section of this guide for more detail.
- What is the difference between hospice and palliative care?
- Palliative care focuses on symptom relief and can begin at any stage of a serious illness, often alongside curative treatments. Hospice care, by contrast, is reserved for patients with a terminal prognosis (typically six months or less) who have chosen comfort over cure. Both prioritize quality of life, but hospice includes a broader support structure for the entire family. See the 'Hospice vs. Palliative Care' section above for a deeper comparison.
- How do hospice nurses work with families and caregivers on a daily basis?
- Hospice nurses serve as the primary clinical point of contact, visiting the home on a scheduled basis and remaining available by phone between visits. Daily responsibilities include assessing the patient, adjusting the care plan, coaching caregivers through symptom management, and providing emotional support. The 'Step by Step Framework for Nurse and Family Collaboration' section maps this involvement from admission through bereavement.
- What training do hospice nurses provide to family caregivers at home?
- Training typically covers medication administration, pain assessment, safe repositioning, wound care basics, recognizing signs of decline, and comfort measures such as oral care and breathing techniques. Nurses also teach caregivers when and how to call for emergency guidance. The 'Caregiver Training' section and the accompanying checklist outline every core skill families should learn.
- What communication tools do hospice teams use for family meetings?
- Common tools include structured family meeting agendas, teach back methods to confirm understanding, goals of care conversation guides, and shared documentation platforms that keep every team member informed. Many agencies also use telehealth or secure messaging for real time updates between in person visits. The 'Communication Tools and Family Meeting Strategies' section walks through each approach in detail.
- How do hospice nurses coordinate with other members of the interdisciplinary team?
- Hospice nurses act as the clinical hub, relaying observations to physicians, social workers, chaplains, home health aides, and bereavement counselors. Coordination happens through regular team meetings, shared electronic records, and direct communication after each home visit. The 'Interdisciplinary Team Roles' section explains how each discipline contributes and how the nurse connects them all.
- What resources are available for family caregivers working with hospice?
- Families can access respite care, bereavement programs, caregiver support groups, educational materials from the hospice agency, and community organizations such as local Area Agencies on Aging. Many hospice programs also offer 24/7 nurse hotlines. The 'Technology and Resources That Strengthen Hospice Collaboration' section provides a fuller overview of digital and in person support options.