Most important takeaways…
- Most trauma centers require the AGACNP certification, not the FNP, making track selection critical before enrolling.
- Becoming a trauma NP typically takes seven to ten years from an initial nursing degree to practice.
- NP employment is projected to grow 35% through 2034, with trauma centers among the fastest-expanding hiring settings.
- Experienced trauma NPs can reach $200,000 annually by layering call shifts, procedures, and strategic location choices.
Trauma nurse practitioners are an established advanced practice role in trauma surgery and emergency care, functioning as autonomous clinicians rather than bedside trauma RNs. Across roughly 2,000 verified U.S. trauma centers, these NPs now lead resuscitations, perform invasive procedures, and manage complex care under collaborative agreements.
Entering the role requires an RN license, a graduate degree through an Adult-Gerontology Acute Care NP track, national board certification, and state licensure. While no standalone "trauma NP" certification exists, the position is embedded within acute care surgery teams and critical care nursing units.
Compensation often exceeds general NP averages, particularly for those taking call or holding procedural privileges. Wide variation in state scope-of-practice laws means your salary and autonomy are tied tightly to your institution and region.
What Does a Trauma Nurse Practitioner Do?
As trauma centers nationwide expand advanced practice coverage to meet 24/7 staffing demands, the trauma nurse practitioner has shifted from a support role into a frontline provider position, often the first advanced clinician at the bedside when a trauma activation rolls through the bay.1
Core Clinical Responsibilities
In a Level I or II trauma center, the trauma NP's day moves between the bay, the ICU, the floor, and the OR. The core responsibilities cluster around four areas:
- Initial trauma assessment: Performing rapid primary and secondary surveys on incoming patients, often arriving simultaneously with the attending surgeon during activations.
- Diagnostics: Ordering and interpreting imaging (CT, FAST exams, plain films) and laboratory studies to triage injuries and guide resuscitation.
- Bedside procedures: Placing central and arterial lines, inserting chest tubes, performing laceration repair and complex wound closure, and managing airways within institutional privileging.
- Care coordination: Communicating with attending trauma surgeons, intensivists, consulting services, and case management to move patients through admission, operative planning, and disposition.
Autonomy in Practice
This is where the trauma NP role diverges sharply from bedside or ED roles. Trauma NPs frequently manage the trauma service census overnight and on weekends, rounding independently, writing orders, adjusting analgesia and antibiotics, and making disposition decisions under collaborative agreements or full practice authority (depending on state law).2 The legal floor is set by state practice statutes; the practical ceiling is set by institutional privileging, which spells out exactly which procedures a given NP can perform unsupervised at that hospital.1 Many trauma NPs also sit on quality improvement committees and help draft the protocols that govern resuscitation, VTE prophylaxis, and rib fracture pathways. Their scope of practice, including assessment, diagnosis, treatment, and prescribing, is comparable to that of other acute care nurse practitioner roles but focused on higher-acuity, multisystem injuries.3
A Note on Job Titles
"Trauma nurse practitioner" is the informal shorthand most clinicians use, but it rarely appears on the actual job posting. Recruiters more often list these roles as Acute Care Nurse Practitioner, Trauma Surgery; NP, Surgical Critical Care; or APP, Trauma Service. Some postings overlap considerably with critical care nurse practitioner positions. When searching openings, use all of these terms; the underlying role is the same.
Trauma NP Vs. Trauma RN: Key Differences
Both trauma nurses and trauma nurse practitioners work in high-acuity environments, often side by side in the same trauma bay. The distinction between the two roles comes down to education, licensure, and how far each can independently carry a patient's care.
Education and Licensure
A trauma RN enters practice with an associate or bachelor's degree in nursing, typically completing two to four years of education before earning an RN license.1 A trauma NP builds on that foundation with a master's or doctoral degree, adding another two to four years of graduate-level training.2 The NP pathway results in an Advanced Practice Registered Nurse credential, which unlocks a substantially different scope of authority.
Scope of Practice
This is where the roles diverge most clearly. Trauma RNs provide direct bedside nursing care, coordinate with the care team, and carry out orders written by providers. They are essential to patient safety and often the first to spot a change in status, but they work within a physician- or provider-directed framework.
Trauma NPs, by contrast, assess patients independently, reach diagnoses, order and interpret diagnostic tests, prescribe medications, and manage treatment plans.2 In many trauma centers and emergency departments, NPs serve as primary providers, particularly during nights, weekends, and surge periods. Some trauma NPs also perform procedures such as chest tube placement or intubation depending on state regulations and institutional credentialing. If you are weighing how trauma NP responsibilities compare with related specialties, our breakdown of acute care, critical care, and trauma nurse practitioner differences can help clarify the landscape.
Earnings and Career Trajectory
The salary gap reflects the difference in responsibility. Trauma RNs earn a national median around $82,500 annually.1 Trauma NPs earn considerably more, with a national median in the range of $128,000, reflecting both the advanced degree requirement and the expanded clinical authority.2
For a working RN weighing whether to pursue an NP, the comparison is useful in another way: the skills and clinical judgment built during years of trauma nursing are a genuine head start. Graduate programs value that hands-on experience, and many trauma NPs say their RN background made them more confident providers from day one of practice.
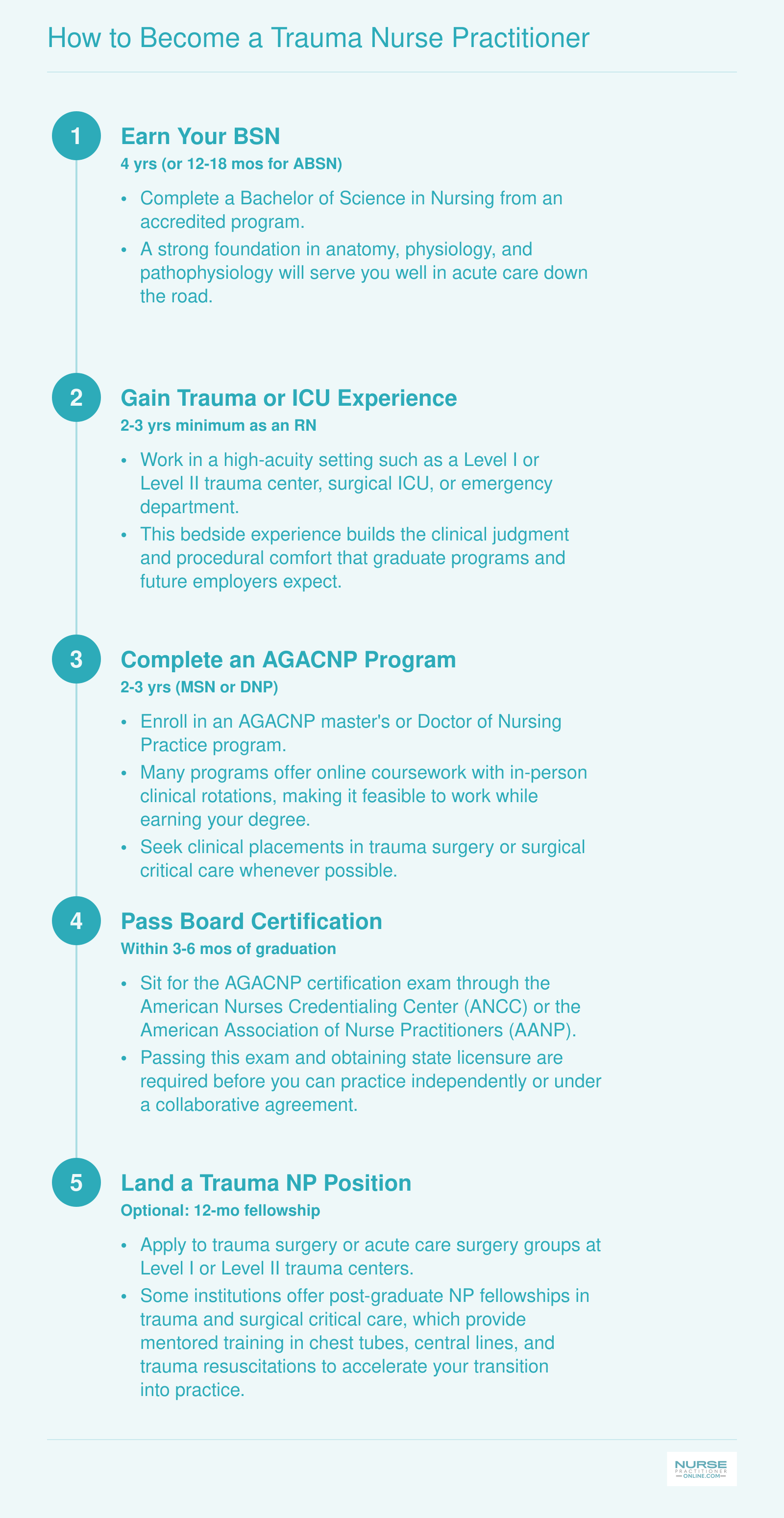
How to Become a Trauma Nurse Practitioner
The path to practicing as a trauma nurse practitioner follows a clear sequence, though it typically takes seven to ten years from your first nursing degree to a trauma NP role. One important note: the Adult-Gerontology Acute Care Nurse Practitioner (AGACNP) track is the recommended population focus for trauma work, not the Family Nurse Practitioner (FNP). Trauma patients require acute, episodic care for unstable and complex conditions, which falls squarely within the AGACNP scope of practice. Most trauma surgery groups and Level I trauma centers expect or require the AGACNP credential.
FNP Vs. AGACNP: Which NP Track Leads to Trauma?
Which nurse practitioner certification actually lets you practice in a trauma bay? The answer is unequivocal: Adult-Gerontology Acute Care Nurse Practitioner (AGACNP) is the required credential for most trauma roles, and the vast majority of Level I and Level II trauma centers will not credential a family nurse practitioner for inpatient acute care. Understanding why this distinction exists, and why it matters for your career trajectory and salary, is essential before you choose your graduate program.
Scope of Practice: FNP vs. AGACNP
The core difference lies in population focus and practice setting. FNP programs train you to care for patients across the lifespan (newborns through geriatrics) in primary care and outpatient contexts. You learn health maintenance, chronic disease management, wellness visits, and the diagnostic reasoning needed to manage stable patients in ambulatory clinics or urgent care.
AGACNP education, by contrast, prepares you to manage acutely ill and critically unstable adult patients (young adults through geriatrics) in hospitals. The curriculum emphasizes pathophysiology of acute illness, advanced hemodynamic monitoring, ventilator management, invasive procedures (central lines, chest tubes, arterial lines), rapid deterioration, and resuscitation. Trauma patients, by definition, fall squarely into this acute, unstable, adult population.
Level I trauma centers typically require AGACNP certification because their credentialing and privileging processes align with scope of practice. An FNP's national certification exam does not cover the competencies required for trauma resuscitation, so hospitals cannot legally or ethically credential you for those tasks, even if you have trauma RN experience.
ACNP vs. AGACNP: Are They the Same Thing?
You may see job postings listing ACNP (Acute Care Nurse Practitioner) instead of AGACNP. Historically, ACNP was the older certification title. In 2012, the American Nurses Credentialing Center (ANCC) updated the credential to Adult-Gerontology Acute Care Nurse Practitioner (AGACNP) to clarify the population focus. Functionally, they are equivalent for hiring purposes. Employers use the terms interchangeably, and your AGACNP certification qualifies you for any posting seeking an ACNP. If you want a deeper comparison, our guide to ACNP vs. AGACNP differences breaks it down further.
Salary Implications: Who Gets Paid More?
ACNPs and AGACNPs working in acute hospital settings generally outearn FNPs, particularly in high-acuity specialties like trauma, critical care nursing, and cardiovascular surgery. This reflects both the intensity of the role (nights, weekends, call, procedural responsibility) and the scarcity of qualified candidates. While FNPs working in underserved primary care or certain specialty outpatient roles can command competitive salaries, the acute care differential typically favors AGACNP graduates in trauma.
Certification, Credentials, and Procedural Scope
Earning your national NP board certification is the first major step for licensure, but it is only half the picture. The real scope of your trauma practice, especially the procedures you will be allowed to perform, is determined at the hospital level through a separate credentialing process. Understanding this two-layer system helps you target the right credentials and avoid surprises when you start a new position.
The Two-Layer Credentialing System
National board certification, such as the ANCC AGACNP-BC or the AANP equivalent, establishes your foundational competence as an adult-gerontology acute care nurse practitioner. Most state nursing boards require this for licensure, and it is the baseline that employers expect. For a deeper look at how nurse practitioner licensing works across states, our dedicated guide covers each step. In trauma and acute care settings, facilities often look for additional proof of specialized knowledge and procedural skill. This is where add-on credentials like TCRN and ATCN come in. They do not replace your NP board certification, but they signal to trauma centers that you have invested in the specialty and are prepared for high-acuity roles.
TCRN: Proving Your Trauma Expertise
The Trauma Certified Registered Nurse (TCRN) credential, offered by the Board of Certification for Emergency Nursing (BCEN), is one of the most recognized specialty certifications in trauma care.1 It is open to any licensed RN, including nurse practitioners, and the eligibility requirement is a current, unrestricted RN license.2 BCEN recommends at least two years of trauma nursing experience, but this is not mandatory.2 The exam consists of 175 multiple-choice questions (150 scored) delivered over 180 minutes at a testing center or via live remote proctoring; the current passing score is 104 out of those 150 scored items.3 Content covers clinical practice (44 percent of the exam), the continuum of care (24 percent), professional issues (12 percent), trauma systems and safety (10 percent), and disaster preparedness (10 percent).4 The non-member exam fee is $380.5 TCRN certification must be renewed every four years with 100 hours of continuing education, including 75 clinical hours and 25 professional hours.3 While the credential is not NP-specific, many employers view it as a strong indicator of trauma competency and a commitment to the field.
ATCN: Preparation That Goes Beyond the Test
The Advanced Trauma Care for Nurses (ATCN) course is a different type of credential: it is a hands-on educational program rather than a certifying exam. It is offered through the Society of Trauma Nurses (STN) in collaboration with the SBAIT, and it teaches advanced trauma nursing concepts through didactic sessions and skill stations. Unlike TCRN, which validates broad knowledge via a test, ATCN focuses on practical application, including team communication, initial assessment, and intervention algorithms. Many Level I and II trauma centers highly value ATCN when credentialing NPs, and some require it before granting clinical privileges.
Institutional Credentialing: The Real Gatekeeper
Even after you hold your NP license, board certification, and specialty credentials, the procedures you can actually perform are finalized by each hospital's credentialing committee. This is a separate process where you submit proof of education and supervised experience for each invasive skill. The committee then grants specific privileges. For example, you might be approved for central line insertion but need to log supervised intubations before gaining that privilege. This system means your procedural scope can differ markedly between two Level I centers in the same state, and it always depends on your collaborative practice agreement and the state's nurse practice act.
Common Procedures for Trauma NPs
While no universal list exists, the following procedures are frequently included in credentialing requests for trauma nurse practitioners at major centers: - Chest tube insertion: placement and management of thoracostomy tubes for pneumothorax or hemothorax - Central venous catheter placement: internal jugular, subclavian, or femoral lines for resuscitation and monitoring - Arterial line insertion: radial or femoral arterial catheters for continuous blood pressure monitoring - Endotracheal intubation: advanced airway management in emergent situations - Wound debridement: removal of devitalized tissue and foreign material - Laceration repair: layered closure of complex wounds - Closed fracture reduction: aligning displaced bones without open surgery - FAST ultrasound: focused assessment with sonography to detect free fluid in the abdomen or pericardium
Your Scope Will Vary
It cannot be overstated: there is no single national list of approved procedures for trauma NPs. Your actual scope depends on the state's nurse practice act, your collaborative agreement, the culture and policies of your hospital, and the specific details of your credentialing file. Some facilities allow NPs to perform all of the above and more, while others restrict certain skills to surgical residents or attending physicians only. When interviewing for trauma NP positions, ask directly about the credentialing process and the steps you would need to take to get fully privileged in the procedures that matter to you.
Trauma Nurse Practitioner Salary: National Overview
Because the Bureau of Labor Statistics does not break out trauma-specific nurse practitioner earnings, the figures below reflect all nurse practitioners nationwide. Trauma NPs who work in Level I or Level II trauma centers, take regular call shifts, or hold procedural credentials often earn above these benchmarks. The national data still provides a useful baseline for nurses weighing the financial return of an NP career path.
| Percentile or Measure | Annual Salary |
|---|---|
| 25th Percentile | $109,940 |
| Median (50th Percentile) | $129,210 |
| Mean (Average) | $132,000 |
| 75th Percentile | $149,570 |
Trauma NP Salary by State
Nurse practitioner salaries vary significantly across states, influenced by cost of living, demand, and scope of practice laws. The figures below reflect BLS data for all nurse practitioners. Trauma NPs working in surgical or critical care settings may earn above these medians, particularly in states with full practice authority and high patient volumes.
| State | Total NPs Employed | 25th Percentile | Median Salary | 75th Percentile | Mean Salary |
|---|---|---|---|---|---|
| California | 20,980 | $140,260 | $166,610 | $205,400 | $173,190 |
| New Jersey | 9,590 | $126,030 | $149,620 | $162,250 | $140,470 |
| Alaska | 570 | $104,000 | $145,450 | $165,510 | $142,340 |
| New York | 20,430 | $128,190 | $145,390 | $164,670 | $148,410 |
| Oregon | 2,430 | $129,840 | $144,600 | $163,240 | $148,030 |
| Washington | 4,790 | $125,890 | $140,220 | $161,730 | $143,620 |
| Connecticut | 3,680 | $125,910 | $138,960 | $159,680 | $141,140 |
| Massachusetts | 8,920 | $125,590 | $138,890 | $160,310 | $145,140 |
| New Mexico | 1,870 | $113,240 | $138,440 | $156,000 | $136,620 |
| Arizona | 7,540 | $115,290 | $133,790 | $151,650 | $132,920 |
| Montana | 1,050 | $112,180 | $133,640 | $141,050 | $131,560 |
| New Hampshire | 1,790 | $120,270 | $132,440 | $143,010 | $133,660 |
| District of Columbia | 790 | $119,240 | $131,380 | $143,960 | $137,600 |
| Hawaii | 470 | $121,410 | $130,940 | $158,100 | $135,020 |
| Rhode Island | 1,200 | $126,200 | $130,710 | $160,030 | $139,600 |
| Texas | 21,690 | $110,570 | $129,880 | $143,860 | $130,930 |
| Colorado | 4,130 | $110,300 | $129,750 | $139,440 | $127,610 |
| Vermont | 680 | $115,650 | $129,740 | $139,930 | $130,580 |
| Iowa | 2,810 | $115,950 | $129,420 | $137,900 | $133,020 |
| Florida | 24,690 | $109,670 | $129,010 | $143,670 | $128,340 |
| Idaho | 1,570 | $119,290 | $128,940 | $140,920 | $131,380 |
| Illinois | 9,560 | $111,450 | $128,620 | $138,420 | $128,880 |
| Wisconsin | 4,950 | $117,630 | $128,580 | $137,150 | $130,490 |
| Minnesota | 8,690 | $103,250 | $128,570 | $139,590 | $128,120 |
| Indiana | 7,470 | $111,210 | $128,280 | $134,840 | $126,520 |
Highest-Paying Metro Areas for Nurse Practitioners
Location plays a major role in NP compensation, and trauma NPs working in large metro areas with Level I trauma centers often benefit from higher pay scales. The table below ranks the top-paying metropolitan areas for nurse practitioners based on BLS data. Keep in mind that these figures reflect all NP specialties; trauma NPs in surgical or critical care roles at busy urban centers may earn at or above the upper end of these ranges.
| Metro Area | Total NPs Employed | 25th Percentile | Median Salary | 75th Percentile | Mean Salary |
|---|---|---|---|---|---|
| Los Angeles, Long Beach, Anaheim, CA | 6,400 | $140,230 | $164,510 | $184,670 | $165,030 |
| New York, Newark, Jersey City, NY/NJ | 19,850 | $135,120 | $152,790 | $167,870 | $151,510 |
| Boston, Cambridge, Newton, MA/NH | 6,660 | $126,120 | $138,890 | $161,750 | $146,850 |
| Miami, Fort Lauderdale, West Palm Beach, FL | 9,200 | $109,990 | $135,450 | $150,840 | $132,730 |
| Phoenix, Mesa, Chandler, AZ | 5,970 | $115,290 | $134,630 | $151,670 | $132,670 |
| Houston, Pasadena, The Woodlands, TX | 4,680 | $118,610 | $133,140 | $143,760 | $133,380 |
| Dallas, Fort Worth, Arlington, TX | 5,300 | $114,990 | $131,910 | $154,240 | $130,980 |
| Chicago, Naperville, Elgin, IL/IN | 6,930 | $114,540 | $131,690 | $141,010 | $131,580 |
| Philadelphia, Camden, Wilmington, PA/NJ/DE/MD | 5,780 | $115,400 | $131,590 | $147,900 | $133,360 |
| Washington, Arlington, Alexandria, DC/VA/MD/WV | 4,430 | $117,310 | $129,920 | $150,380 | $131,380 |
| Atlanta, Sandy Springs, Roswell, GA | 6,280 | $115,690 | $128,640 | $140,140 | $129,710 |
| Minneapolis, St. Paul, Bloomington, MN/WI | 5,680 | $106,660 | $128,570 | $139,590 | $128,740 |
| Tampa, St. Petersburg, Clearwater, FL | 3,810 | $105,410 | $128,430 | $134,190 | $125,970 |
| Detroit, Warren, Dearborn, MI | 3,850 | $114,080 | $126,110 | $135,030 | $128,140 |
| Nashville, Murfreesboro, Franklin, TN | 5,380 | $101,520 | $116,160 | $129,590 | $112,610 |
How to Make $200K as a Trauma NP
Reaching the $200,000 threshold as a trauma nurse practitioner requires a combination of strategic career moves, geographic choices, and willingness to take on premium shifts and specialized procedures. The good news: it is achievable for experienced trauma NPs who layer multiple income levers and position themselves in high-demand markets.
Realistic Levers to Boost Compensation
The clearest path to $200K starts with employment at a Level I trauma center in a high-cost-of-living metropolitan area. Cities like San Francisco, New York, Boston, Seattle, and Washington, D.C. routinely offer base salaries in the $140,000 to $160,000 range, and that foundation makes the remaining gap easier to close. From there, overnight and weekend call differentials add meaningful increments; many trauma NPs earn an extra $15 to $25 per hour for overnight coverage, and weekend shifts often carry similar premiums. Picking up extra shifts above your contracted hours, especially during periods of staffing shortages, can push annual earnings well into six figures.
Negotiating for procedural bonuses is another lever. Trauma NPs who independently perform central lines, chest-tube placements, wound debridements, or minor surgical procedures may qualify for per-procedure stipends or quarterly performance incentives that stack on top of base pay.
Surgical Subspecialty Premium
NPs in surgical subspecialties, including trauma and cardiology nurse practitioner roles, consistently earn more than primary-care NPs. National data shows that acute-care NPs (the typical pathway for trauma work) command higher median salaries than family NPs, reflecting the procedural complexity, call burden, and higher-acuity patient populations. Graduates of acute care nurse practitioner programs are well positioned for these roles. The Bureau of Labor Statistics reports that the 75th percentile for nurse practitioners nationally is approximately $140,000; trauma NPs who combine that baseline with shift differentials, geographic pay adjustments, and procedural volume routinely exceed it.
Locum Tenens and Travel Assignments
Locum tenens or travel trauma NP contracts can push total compensation above $200K, sometimes reaching $220,000 to $250,000 annually when housing stipends and per diems are factored in. These assignments thrive in rural trauma centers or facilities experiencing sudden staffing gaps. The tradeoff is instability: contracts are typically thirteen weeks to six months, benefits are limited or self-funded, and you may relocate every few months. For NPs willing to embrace mobility and manage their own retirement accounts and health insurance, locum tenens pros and cons for nurse practitioners are worth weighing carefully before making the leap.
Where Trauma NPs Work: Settings and Specializations
Trauma nurse practitioners practice in high-intensity environments where severe injuries require immediate advanced intervention, ranging from verified trauma centers and burn units to military surgical teams and remote critical-access hospitals. The setting you choose shapes not only your clinical scope but also your schedule, earning potential, and long-term career sustainability.
Level I vs. Level II Trauma Centers
Level I trauma centers represent the highest tier of trauma care, typically affiliated with academic medical centers and serving as regional referral hubs. NPs in these settings handle the broadest procedural scope and highest patient acuity, working alongside large multidisciplinary teams that include trauma surgeons, intensivists, and subspecialty consultants. You may focus on specific rotations or patient populations within a larger service.
Level II trauma centers provide definitive care for most trauma patients but may transfer the most complex cases to Level I facilities. NPs here often carry broader individual responsibility because the team is smaller. You might manage more patients independently overnight or cover multiple aspects of care that would be divided among several providers at a larger center.
Subspecialty Tracks
Within trauma care, NPs can develop expertise in focused areas:
- Adult trauma surgery: The most common pathway, covering blunt and penetrating injuries across general surgical populations.
- Pediatric trauma: Positions in pediatric intensive care units require specialized training in developmental considerations and family-centered care.
- Burn centers: These units combine wound management, critical care, and long-term reconstruction planning.
- Neurosurgical trauma: NPs manage traumatic brain injuries and spinal cord injuries, often collaborating closely with neurosurgery and rehabilitation teams.
- Orthopedic trauma: Focus on complex fractures, pelvic injuries, and limb salvage in conjunction with orthopedic surgeons.
Several of these subspecialty tracks overlap with broader nurse practitioner specialties, so exploring adjacent career paths can help you identify the best fit.
Non-Hospital Settings
Trauma NPs also practice outside traditional hospital walls. Military trauma teams deploy NPs to forward surgical units where they may be the senior medical provider during mass casualty events. Flight NPs working in air-medical transport manage critically injured patients during helicopter or fixed-wing transfers, making time-sensitive decisions without immediate backup. Rural critical-access hospitals increasingly rely on NPs as the sole advanced provider for trauma stabilization before transfer, combining emergency and trauma skills in resource-limited environments.
How Setting Affects Your Career
Your choice of practice environment directly influences daily life. Level I centers often offer more predictable scheduling through shift-based models, while smaller facilities may require heavier call burdens. Salaries tend to be higher in urban Level I centers and specialty settings like burn units, but rural and military positions sometimes offer loan repayment or other incentives. If you are drawn to musculoskeletal trauma specifically, learning more about the orthopedic nurse practitioner role can clarify how that pathway differs from general trauma. Burnout risk varies significantly by setting, a topic the next section addresses in detail.
Day-To-Day Life: Schedule, Call Patterns, and Burnout
Fixed schedules versus rotating call: the shift structure you land in will shape every aspect of your daily experience as a trauma nurse practitioner. Understanding what a typical workweek looks like, and how the pace affects long-term well-being, is essential before committing to this high-acuity specialty.
Typical Shift Patterns
Trauma NPs generally work in settings that demand around-the-clock coverage, so schedules vary widely by employer. Common arrangements include:
- 12-hour clinical shifts: Many Level I and Level II trauma centers staff NPs on 12-hour day or night rotations, often three to four shifts per week.
- Call coverage: On-call expectations are the norm. Some programs use a 24-hour in-house call model, while others rely on home call with a rapid-response expectation of 20 to 30 minutes.
- Weekend and holiday rotations: Trauma does not follow a calendar. Expect regular weekend obligations and holiday coverage, typically shared among a team of providers.
Workload can be intense. Studies of advanced practitioners in high-volume specialties report seeing an average of 13 patients per day, with ranges spanning 6 to 22 patients depending on census and acuity.1 Trauma NPs in busy surgical services often land at the upper end of that spectrum during peak shifts.
Burnout Reality
The emotional and physical toll of trauma care is well documented. According to a 2024 survey of nurse practitioners across specialties, roughly 37 percent reported burnout, and an additional 28 percent reported experiencing both burnout and depression simultaneously.2 A separate multi-state study of over 1,200 NPs found a burnout rate of about 26 percent, though that sample focused on primary care rather than acute surgical environments.3
Trauma NPs face unique stressors that can push those numbers higher: exposure to severe injuries, high-stakes decision-making with limited time, overnight call disruptions, and the cumulative weight of patient mortality. Research published in journals focused on trauma and acute care surgery consistently identifies irregular shift patterns and prolonged call hours as key contributors.
Protecting Yourself
Burnout is not inevitable, but it does require deliberate prevention. Strategies that trauma NPs and their employers use to maintain sustainability include:
- Negotiating predictable call schedules with adequate recovery days between shifts.
- Working in group practice models where call is distributed equitably among multiple providers.
- Using institutional wellness resources, peer support programs, and regular debriefing after critical cases.
- Setting clear boundaries around overtime, especially during fellowship-style early career years when the temptation to prove yourself can override self-care.
If you are still exploring training pathways, reviewing online DNP acute care nurse practitioner programs can help you identify programs that include clinical rotations in trauma settings, giving you a realistic preview of the workload before you commit. Medscape also releases annual reports that break down burnout statistics by NP specialty, giving you benchmark data to compare against a prospective employer's workload expectations.
The reality is that trauma NP work is demanding, but many practitioners describe it as the most professionally fulfilling role they have held. The key is choosing an employer and schedule structure that supports longevity rather than treating you as an endlessly available resource.
Career Outlook and Advancement for Trauma NPs
The demand for trauma nurse practitioners is accelerating faster than almost any other clinical role, driven by projected NP job growth of 35% through 2034 and mounting pressure on trauma centers.1 While the Bureau of Labor Statistics classifies nurse practitioners under SOC 29-1171 and expects employment to grow much faster than average over the 2024 to 2034 decade, trauma-specific demand is further amplified by resident work-hour limits, an aging population, and rising surgical volumes at Level I and II centers. Trauma program managers increasingly view TNPs as a solution to workforce gaps, creating a landscape where skilled trauma NPs can write their own ticket.
Outpacing the Market: Why Trauma NPs Are in High Demand
BLS projections place nurse practitioner job growth at 35% from 2024 to 2034, a rate that dwarfs most occupations.1 Trauma centers, in particular, feel the squeeze: ACGME duty-hour restrictions have reduced the availability of surgical residents, while trauma admissions continue to climb. Hospitals are turning to advanced practice providers to fill the void, and trauma NPs, with their ability to manage complex patients across the continuum, are among the most sought-after. This convergence of regulatory pressure and clinical need means that today's trauma NP graduates often receive multiple offers before completing their programs.
From Clinical Practice to Leadership: The Trauma NP Career Ladder
A trauma NP career typically begins with a staff role embedded in a trauma service, where you manage initial assessments, perform life-saving procedures, and coordinate care from resuscitation through discharge. With experience, you can advance to senior or lead NP positions, mentoring new hires and influencing protocol development. The next rungs include formal leadership titles such as NP coordinator or director of advanced practice, where you oversee APPs across the trauma program, manage budgets, and drive quality improvement initiatives. Many experienced trauma NPs eventually pivot into trauma program management or become academic faculty, teaching the next generation of nurses and NPs. This ladder offers both clinical and administrative growth, often without requiring a departure from direct patient care.
Post-Graduate Fellowships: Building Specialty Expertise
For new NPs aiming to enter trauma care, a post-graduate fellowship or residency can bridge the gap between general NP education and the high-acuity demands of a Level I center. These programs typically last 12 to 18 months and combine mentored clinical rotations with structured didactic components. You will rotate through trauma surgery, neurotrauma ICU, orthopedic trauma, and emergency general surgery while attending weekly conferences and simulation labs. Well-known programs include the R Adams Cowley Shock Trauma Center NP Fellowship at the University of Maryland, the Vanderbilt University Medical Center Acute Care NP Fellowship (which heavily emphasizes trauma), and the Emory University Acute Care/Trauma NP Residency. Fellowship-trained trauma NPs often command higher starting salaries and transition more smoothly into autonomous practice. If you are considering a related high-acuity path, emergency nurse practitioner roles share many of the same procedural competencies and offer a complementary career trajectory.
Strengthening the Business Case for Trauma NP Hiring
Trauma NPs directly improve patient outcomes in measurable ways, reducing time-to-procedure for interventions like chest tube insertion or central line placement and providing longitudinal continuity that reduces handoff errors. Studies have shown that embedding NPs on trauma services shortens length of stay and lowers complication rates. These metrics translate into lower costs and better quality scores, making the financial argument for expanding trauma NP teams hard to ignore. Nurses interested in online post-master's ACNP certificate programs can use that credential as a stepping stone into trauma practice. As trauma program directors face growing pressure to meet benchmarks while managing lean resident teams, the return on investment from a well-trained trauma NP becomes a compelling lever for recruitment and retention.
Common Questions About Trauma Nurse Practitioners
Below are some of the most common questions working nurses ask when considering a career as a trauma nurse practitioner. Each answer draws on information covered throughout this guide.
- Is there such a thing as a trauma nurse practitioner?
- Yes. While there is no single certification labeled "Trauma NP," nurse practitioners who specialize in trauma care are a well established part of modern trauma programs. Most earn an Acute Care NP (AGACNP) credential and then gain specialized trauma experience on the job. Many also hold the Trauma Certified Registered Nurse (TCRN) credential to demonstrate focused expertise.
- Who gets paid more, FNP or ACNP?
- ACNPs typically earn more than FNPs, largely because they work in higher acuity hospital settings such as trauma surgery, critical care, and emergency departments. Bureau of Labor Statistics data shows that NPs in hospital roles tend to out-earn those in outpatient or primary care. Exact differences vary by region and employer, but ACNPs often see a premium of several thousand dollars per year.
- What is the average salary for a TCRN?
- The TCRN is a specialty certification for registered nurses, not nurse practitioners, so TCRN holders earn RN level wages. According to BLS data, the median RN salary in 2024 was approximately $86,070 per year. RNs who hold the TCRN may earn slightly above that median because they typically work in high acuity trauma centers, but the credential itself does not automatically raise pay.
- Which NP specialty should I choose if I want to work in trauma?
- The Adult Gerontology Acute Care Nurse Practitioner (AGACNP) track is the strongest pathway. AGACNP programs prepare you to manage acutely and critically ill patients, which aligns directly with trauma care. Family Nurse Practitioner (FNP) programs focus on primary care across the lifespan and generally do not include the acute care clinical hours trauma employers require.
- Can a trauma NP prescribe medications?
- Yes. Nurse practitioners, including those working in trauma, hold prescriptive authority in all 50 states. In full practice authority states, NPs prescribe independently, including controlled substances. In reduced or restricted practice states, a collaborative agreement with a physician may be required. Trauma NPs routinely prescribe pain management medications, antibiotics, sedatives, and other drugs critical to acute patient care.
- Do trauma NPs work in the emergency department or on the surgical floor?
- Both. Trauma NPs commonly rotate between emergency department trauma bays and surgical intensive care or step down units. Some focus primarily on the initial resuscitation and stabilization in the ED, while others manage postoperative recovery on surgical floors. The exact split depends on the institution, the size of the trauma program, and whether the facility is a Level I, II, or III trauma center.
Explore More
- Acute Care Nurse Practitioner (ACNP)
- Adult-Gerontology Nurse Practitioner (AGNP)
- Cardiology Nurse Practitioner
- Critical Care Nurse Practitioner (CCNP)
- Dermatology Nurse Practitioner
- Emergency Nurse Practitioner (ENP)
- Family Nurse Practitioner (FNP)
- Forensic Nurse Practitioner
- Functional Medicine Nurse Practitioner
- Holistic Nurse Practitioner
- Neonatal Nurse Practitioner (NNP)
- Occupational Health Nurse Practitioner
- Oncology Nurse Practitioner
- Orthopedic Nurse Practitioner
- Palliative Care Nurse Practitioner
- Pediatric ER Nurse
- Pediatric Nurse Practitioner (PNP)
- Psychiatric-Mental Health Nurse Practitioner (PMHNP) Guide
- What Do Urgent Care Nurse Practitioners Do? Role Guide
- Women's Health Nurse Practitioner (WHNP)