Most important takeaways…
- Public health NPs bridge clinical care and community resources through screening, referral, and follow-up beyond the exam room.
- BLS projects nurse practitioner employment to grow 46 percent from 2023 to 2033, largely driven by public health expansion.
- Most public health NPs earn a primary board certification like FNP-BC, then add credentials such as ANCC Advanced Public Health Nursing.
- No single degree is labeled public health nurse practitioner, so the pathway requires pairing an MSN or DNP with intentional public health coursework.
More than 80 million Americans live in federally designated Health Professional Shortage Areas, yet only a fraction of nurse practitioners are trained to address the social determinants driving poor health outcomes in those communities. The gap is widening. Traditional clinic-based care cannot solve problems rooted in housing instability, food insecurity, or lack of transportation. Clinical-community linkages, a framework that connects medical care to community resources, have emerged as the most effective response, and nurse practitioners are uniquely positioned to lead that work.
The challenge is practical. Most NP programs still emphasize individual patient encounters, not population-level interventions or upstream prevention. Public health departments, schools, community health centers, and nonprofits need clinicians who can diagnose a patient and also design a diabetes prevention program or partner with housing agencies to reduce asthma exacerbations. That dual skill set remains rare, even as demand for it accelerates across underserved urban and rural areas alike.
What Is a Public Health Nurse Practitioner?
A public health nurse practitioner is an advanced-practice registered nurse (APRN) with a master's or doctoral degree, full diagnostic and prescriptive authority in most states, and a working focus on population health rather than only the patient in front of them. The role sits at the intersection of two well-established fields: advanced clinical practice and public health.
The Dual-Lens Role
Where a primary care NP treats the diabetes patient who walks into the clinic, a public health NP treats that patient and asks why the surrounding zip code has triple the diabetes rate. The work is simultaneous, not sequential. In a single afternoon, a public health NP might adjust insulin for one patient, write a referral to a food-access program for another, and meet with a county health officer about a community screening initiative.
That dual lens, individual clinical care plus population-level assessment, is what distinguishes the role. Public health NPs are trained to read social determinants (housing, food security, environmental exposures, structural racism, transportation gaps) the same way they read lab values.
How It Differs from Adjacent Roles
The titles in this space overlap, and it helps to draw clean lines:
- Public health nurse (PHN): Typically a BSN-prepared RN working in a health department or community agency. PHNs do vital outreach, case management, and education, but they do not diagnose conditions or prescribe medications.
- Community health nurse: Often used interchangeably with PHN. Scope is similar: RN-level practice focused on community wellness without independent prescriptive authority.
- Standard NP (FNP, ANP, PNP, etc.): Full clinical authority, but trained and credentialed around individual patient care in a clinic, hospital, or specialty setting. Population health is not the organizing frame.
The public health NP layers the population focus onto the full NP clinical toolkit.
An Emerging, Hybrid Title
Worth knowing: "public health nurse practitioner" is not yet a standalone board certification in the way FNP or AGNP is. Most clinicians in this role hold a standard NP certification, and the family nurse practitioner pathway is among the most common starting points. Others pursue Adult-Gerontology NP credentials and then add public health training, often through a dual MSN/MPH degree, a post-master's certificate, or credentials like the Advanced Public Health Nursing certification from the ANCC. For nurses weighing their options, understanding nurse practitioner advancement opportunities can help clarify how a public health orientation fits into a broader career plan. The title describes a practice orientation as much as a specific credential.
What Are Clinical-Community Linkages?
When a patient's health depends more on stable housing than a new medication, the traditional clinic visit falls short. Countless health outcomes are shaped outside the exam room, by food security, transportation, safe neighborhoods, and access to social services. Yet most healthcare settings aren't equipped to bridge that gap. That's where clinical-community linkages (CCLs) come into play, and nurse practitioners are uniquely prepared to lead them.
Bridging the Gap Between Clinic and Community
A clinical-community linkage is a deliberate, bidirectional connection between healthcare providers and community resources. The CDC defines CCLs as relationships between the clinical and community sectors that aim to improve population health by preventing and managing chronic diseases.1 The Agency for Healthcare Research and Quality (AHRQ) adds an emphasis on sustainability: effective linkages are lasting partnerships between primary care clinicians and community organizations that deliver preventive services.2 In practice, that means a clinic doesn't just hand a patient a list of phone numbers; it builds a coordinated pathway that follows the patient all the way to the service they need, and gets feedback on whether it worked.
The Three Core Components of a Strong Linkage
Every effective CCL rests on three pillars:
- Clinical identification of needs: Healthcare settings, often during a primary care visit, screen for social determinants of health like food insecurity, housing instability, or lack of transportation.
- Community organization capacity: Community-based groups (food pantries, housing authorities, health educators) are ready to deliver resources tailored to the patient's situation.
- Bidirectional referral and feedback: A structured system passes the referral from clinic to community site and then closes the loop with outcome data. This feedback loop ensures the linkage isn't a one-way handoff but an ongoing collaboration that adjusts based on what patients actually experience.
These components aren't just theoretical. Operational structures can include formal referral pathways, shared care coordination teams, data-sharing agreements, or even community health workers who personally connect patients to services.3 Post-2023 federal guidance has sharpened the focus on health equity, urging linkage designs that intentionally reach priority populations and address structural social determinants.4
Why Nurse Practitioners Are the Natural Link
NPs bring a rare combination of clinical authority and holistic training. They hold prescriptive power, so they can manage chronic conditions medically, but they are also educated in patient-centered, upstream-focused care. An NP's typical visit goes beyond symptoms; it explores the whole context of a person's life. That dual lens makes it instinctive to screen for social needs and translate those into actionable referrals. Moreover, NPs often work in community settings like Federally Qualified Health Centers, school-based clinics, and rural health posts, where the distance between clinic and neighborhood is shortest. They see the same barriers their patients face and can build trust that a distant specialist could not.
Linkages in Action: Real-World Examples
Consider a Federally Qualified Health Center NP who screens for food insecurity during a well-child visit. With a formal linkage, she doesn't just suggest a local food bank; she sends a warm referral through a shared platform, and the pantry confirms that the family received a week's worth of meals. Or think of a school-based pediatric nurse practitioner coordinating asthma care: she partners with the county health department to arrange home environmental assessments and remediation for triggers like mold, then receives follow-up data showing reduced emergency visits. These aren't one-off favors; they're structured linkages that turn good intentions into measurable clinical improvement projects.
Questions to Ask Yourself
Why Public Health Needs Nurse Practitioners
Reactive care versus proactive care: that contrast sits at the heart of why the public health system urgently needs more nurse practitioners. The United States has spent decades patching gaps in reactive, hospital-centered medicine while preventable chronic disease, health disparities, and access barriers have widened. NPs are positioned to tip the balance back toward prevention and community-based care, and the workforce data makes the case clearly.
A Shortage That Keeps Growing
The Bureau of Labor Statistics projects nurse practitioner employment will grow roughly 46 percent from 2023 to 2033, making it one of the fastest-growing occupations in healthcare. That growth is not happening in a vacuum: it reflects a system scrambling to staff primary care access points that physicians alone cannot fill. Somewhere between 75 million and 80 million Americans currently live in federally designated primary care Health Professional Shortage Areas, according to federal health workforce data. In practical terms, millions of people have no reliable access to a primary care nurse practitioner, no one to catch diabetes before it causes kidney failure, no one to connect a struggling family to housing assistance or mental health services.
Filling the Gaps Physicians Leave
Physicians have historically gravitated toward urban centers, specialty practice, and settings that offer higher reimbursement. Rural counties, tribal lands, and under-resourced urban neighborhoods are often left behind. Nurse practitioners with full practice authority, now recognized in a growing number of states, can open independent clinics, take on patient panels, and deliver the full scope of primary care without a physician co-signature. Understanding which states need nurse practitioners the most helps illustrate how uneven access remains across the country. That autonomy is not a workaround; it is a policy tool that brings real care to the communities that need it most.
Whole-Person Training Meets Population Health
NP education emphasizes whole-person assessment, which means graduates are trained to look beyond the presenting complaint and ask about stress, food security, transportation, and social support. That training aligns almost perfectly with the social determinants of health framework that public health professionals use to address root causes of illness. Where a physician visit might end with a prescription, an NP encounter can end with a referral to a community food pantry, a warm handoff to a behavioral health counselor, or enrollment in a chronic disease self-management program.
Research consistently shows that NP-staffed clinics produce outcomes comparable to physician-only models across chronic disease management, preventive screenings, and patient satisfaction. Some studies suggest outcomes are better in certain populations, though researchers caution that clinic design, patient population, and resources all influence results. What the evidence does support clearly is that NP-led care is not a compromise.
Reducing Costs at the System Level
Cost-effectiveness is the argument that tends to move policymakers. NP-led community health interventions are associated with reduced emergency department utilization and fewer preventable hospital readmissions, two of the most expensive outcomes in the system. When a nurse practitioner follows up with a recently discharged heart failure patient, connects a diabetic patient with a community health worker, or runs a school-based clinic that catches asthma flares early, the downstream savings are measurable. For a healthcare system straining under the weight of preventable illness, that fiscal argument reinforces what clinicians already know: getting care into communities before crises develop is simply smarter medicine.
How NPs Strengthen Clinical-Community Linkages in Practice
Clinical-community linkages come alive when a nurse practitioner spots a health risk in the exam room and follows it out the door into the patient's neighborhood, school, food pantry, or housing program. The work is concrete: screen, refer, follow up, measure, repeat. Below are three practice patterns showing how NPs translate that bridging role into measurable outcomes.
Case Scenario: Chronic Disease Management in an FQHC
In a federally qualified health center, an NP running a panel of adults with type 2 diabetes pairs in-clinic visits with referrals to a community health worker for home glucose coaching, a SNAP enrollment navigator, and a YMCA diabetes prevention class. Research on NP-led chronic disease interventions shows this kind of integrated model can cut emergency department visits by 15 to 30 percent.1 A 2025 analysis of full practice authority states found that diabetes readmission rates were meaningfully lower where NPs practice independently (incidence rate ratio 0.97) compared to restricted states (1.00), with similar gains for hypertension and asthma readmissions.2
Case Scenario: School-Based Vaccination and Screening
A school-based NP partnering with the county health department runs catch-up immunization clinics, vision and behavioral health screenings, and referrals into Medicaid-enrolled primary care homes. The clinical-community linkage here is operational: the NP holds the clinical license, the health department supplies vaccine and surveillance data, and school staff handle outreach. When a child screens positive for asthma symptoms, the NP coordinates a same-week clinic visit and a home environmental assessment through the local public health program.
Case Scenario: Nurse-Led Case Management for Super-Utilizers
Medicaid super-utilizers, patients with six to eight ED visits per year driven by unmanaged chronic disease, housing instability, or behavioral health needs, are a population where NP-led case management produces some of the clearest returns. Documented care coordination programs have brought those patients down to three to four ED visits per year and reduced hospital admissions by 20 to 40 percent through structured panel management, motivational interviewing, and warm handoffs to social services.3
The Data Layer
What ties these scenarios together is the NP's use of population-level data. Panel management dashboards flag patients overdue for A1C checks or blood pressure follow-up. Community health assessments identify ZIP codes with the highest uncontrolled hypertension rates. Nursing quality improvement projects run quarterly tell the NP whether the referral pipeline to community partners is actually closing care gaps, or whether it needs to be rebuilt.
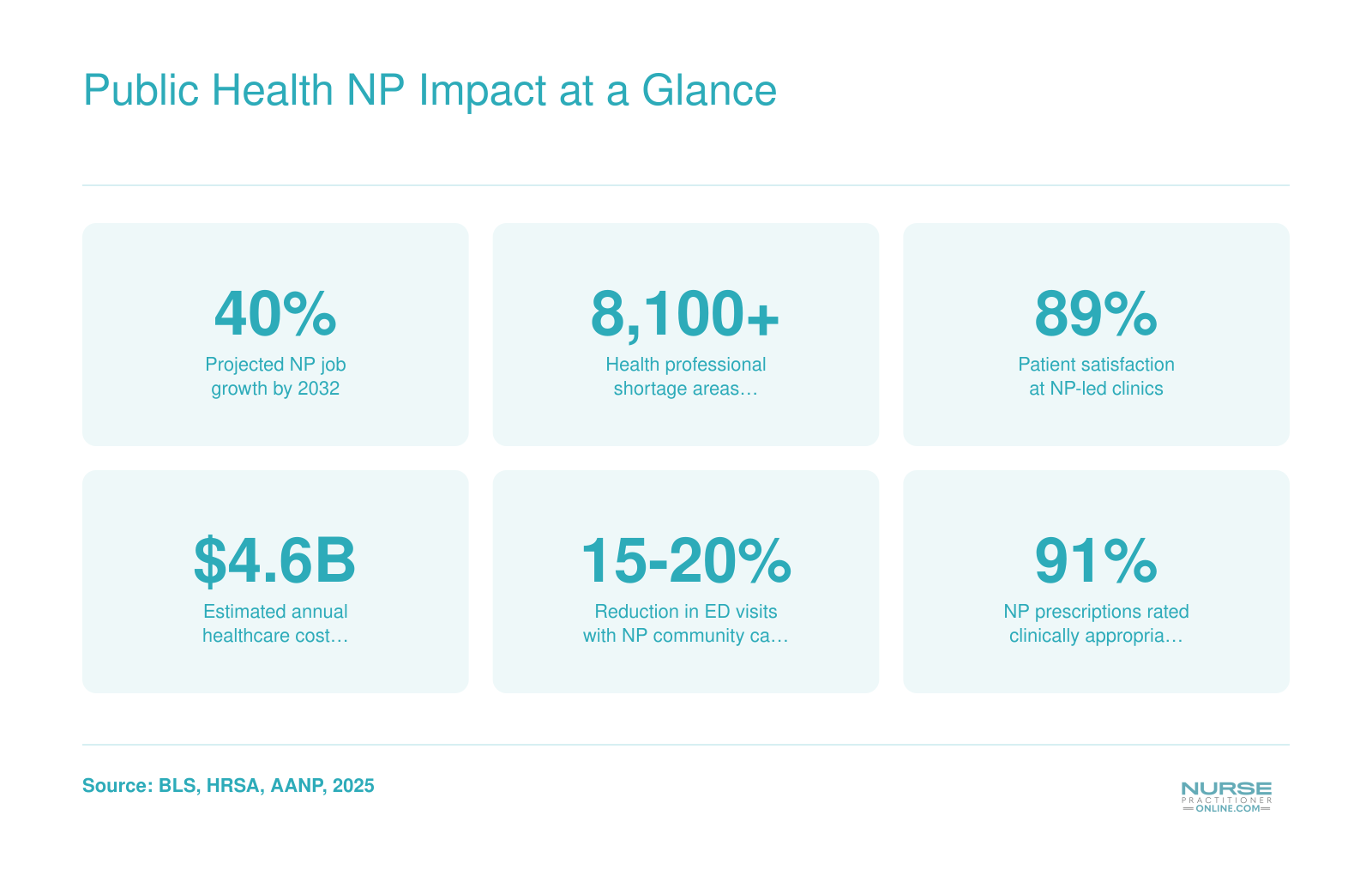
Public Health NP Impact at a Glance
Nurse practitioners are reshaping public health outcomes across the country. These figures illustrate why the need for nurse practitioners in community and public health settings continues to grow.
How to Become a Public Health Nurse Practitioner
There is no single degree labeled 'Public Health Nurse Practitioner,' which means the pathway requires intentional choices at several decision points along the way.
Start with Your Foundation: BSN and RN Licensure
Every public health NP begins as a registered nurse. You need a Bachelor of Science in Nursing, a passing NCLEX score, and active state licensure. Most public health employers and graduate programs expect at least one to two years of bedside or community nursing experience before you apply to NP school. Direct patient care builds the clinical judgment and communication skills that transfer directly into population-level work.
Choose Your Graduate Pathway
Most public health NPs enter through a standard Family Nurse Practitioner program. FNP credentials grant you the widest scope of practice, from newborns to older adults, which is essential when working with diverse communities. An adult-gerontology nurse practitioner track is another common route, especially if your public health focus leans toward chronic disease management in older populations.
You can pursue either a Master of Science in Nursing or a Doctor of Nursing Practice. MSN programs typically run 18 to 24 months for full-time students, while DNP programs add another year or more depending on your starting credential. Both prepare you to sit for nurse practitioner licensing and national certification exams.
Add Public Health Training
After earning NP certification, many nurses build public health expertise through continuing education, on-the-job training, and post-graduate certificates. Some programs offer dual MSN/MPH degrees that combine clinical authority with formal training in epidemiology, biostatistics, health policy, and community assessment. Dual degrees usually add one year to a standalone MSN but save time compared to earning the degrees separately.
If you already hold an MSN, you can pursue a standalone MPH in 12 to 18 months, often online and part-time, while working in a public health role.
What Changes When You Transition from Bedside to Public Health
Your clinical judgment, rapport-building, and triage instincts transfer seamlessly. What shifts is your unit of care: instead of one patient at a time, you assess neighborhoods, design interventions for high-risk groups, and collaborate with schools, housing authorities, and food banks. You may learn grant writing, program evaluation, and data visualization. Some NPs find the pace slower and more strategic; others appreciate the chance to address root causes rather than downstream symptoms. For those drawn to roles beyond direct patient care, non-clinical nurse practitioner jobs offer yet another avenue for population-level impact.
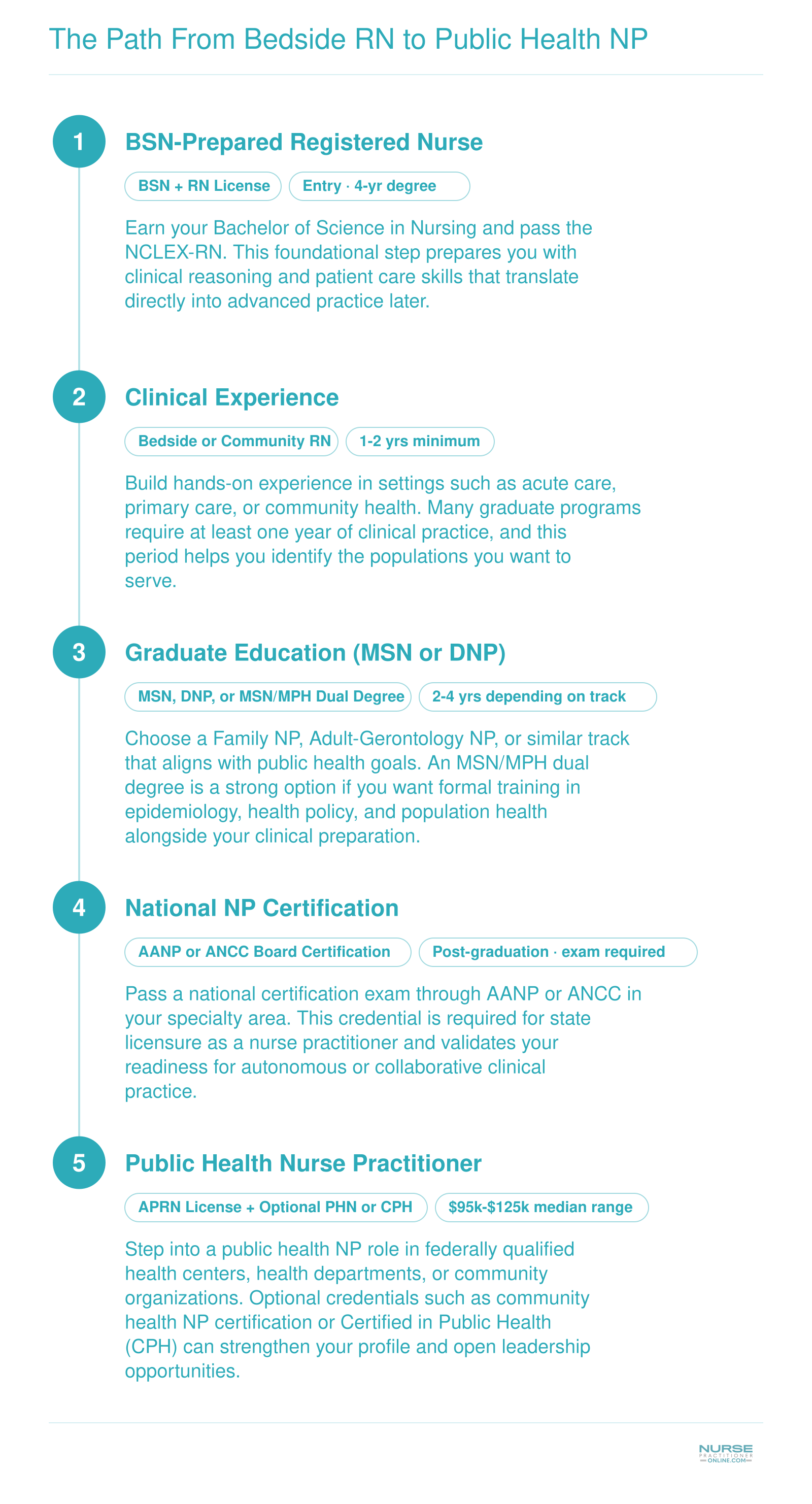
The Path From Bedside RN to Public Health NP
Moving from bedside nursing into public health practice is a structured journey with clear milestones. Here is what the typical progression looks like, along with approximate timelines and key decisions at each stage.
Public Health NP Certifications and Credentials
There is no single "community health nurse practitioner certification." Becoming a public health NP means stacking two layers of credentials: a primary NP board certification that gives you prescriptive authority, plus optional public health credentials that signal population-level expertise.
Primary NP Board Certifications
Your foundation is national NP certification. For public health work, the most common entry points are:
- ANCC Family Nurse Practitioner (FNP-BC): Issued by the American Nurses Credentialing Center. The FNP scope (newborn through older adult) maps well to community clinics, school-based health, and rural health settings where you'll see whole families.
- AANP Family Nurse Practitioner (FNP-C): Issued by the American Academy of Nurse Practitioners Certification Board. Clinically equivalent to FNP-BC; many NPs choose between them based on exam style and renewal preferences.
- ANCC Adult-Gerontology Primary Care NP (AGPCNP-BC) or Acute Care (AGACNP-BC): A strong fit if your community work centers on chronic disease management, older adults, or hospital-to-community transitions.
Eligibility for all three requires an accredited MSN or DNP in the matching population focus, an unencumbered RN license, and supervised clinical hours. Exam fees generally run in the $295 to $395 range depending on professional membership status. If you're weighing primary care versus acute care tracks, our guide on acute care NP vs primary care NP breaks down the key differences.
Public Health Specific Credentials
Layered on top of NP certification, you have a few options, though the landscape is shifting in 2026.
- ANCC Advanced Public Health Nursing (PHNA-BC): Notably, ANCC has retired this credential for new applicants.1 Current certificants can renew on the standard five-year cycle (75 CE hours, including 25 pharmacotherapeutics hours for APRNs) for $250 to $350 depending on membership.1 Reapplication after lapse runs $400, and a retired-designation option is available for $75 to $100.
- California Public Health Nurse (PHN) Certificate: A state-issued credential requiring an active California RN license and a BSN with embedded PHN coursework (or equivalent post-baccalaureate coursework).2 Application fees run $75 to $150. Several states have similar PHN designations.
- NBPHE Certified in Public Health (CPH): A broader public health credential ($385 exam) open to graduates or students of CEPH-accredited programs, or those with a degree plus public health work experience.3 The National Board of Public Health Examiners is also developing a Certified Public Health Nurse (CPHN) credential, expected to launch in late 2026, which may become the new standard.4
- APHA Public Health Nursing Section: A professional home and policy voice, but it does not issue formal certifications.1
Optional but Useful Add-Ons
If your community work intersects with emergency preparedness, consider the ANCC National Healthcare Disaster Professional (NHDP-BC) credential, which requires three years of disaster-related experience within the last ten years.3 Initial certification runs $270 to $395. For those exploring best online FNP programs as a starting point toward public health practice, the family track remains the most versatile pathway into community-based care.
The practical takeaway: secure your NP board certification first, then choose public health credentials that match your state and your scope. Watch the NBPHE CPHN launch closely; it may consolidate what is currently a fragmented credentialing path.
Where Public Health NPs Work: Settings and Roles
Not every public health setting is the right fit for every nurse practitioner. Your ideal workplace depends on what you value most, whether that is salary, autonomy, community impact, or work-life balance. Here is a practical look at the most common practice environments and what each one offers.
Pros
- Federally Qualified Health Centers (FQHCs) often qualify NPs for federal loan repayment programs, easing student debt significantly.
- FQHCs provide structured team environments with built-in referral networks for underserved populations.
- Local and state health departments typically offer predictable schedules, solid benefits, and meaningful policy-level influence.
- Health department roles can grant NPs considerable clinical autonomy, especially in states with full practice authority.
- School-based health centers let NPs shape children's long-term wellness and build deep, ongoing relationships with families.
- Mobile clinic work delivers immediate, tangible community impact and reaches populations that traditional facilities often miss.
- Nonprofit and NGO positions align strongly with mission-driven NPs and may offer global health or disaster-response opportunities.
- Nonprofits and NGOs frequently encourage innovative care models, giving NPs room to design community-centered programs.
Cons
- FQHC workloads can be heavy due to high patient volumes and limited staffing, which may lead to burnout over time.
- Salaries at FQHCs, health departments, and nonprofits generally fall below what hospital or private-practice NPs earn.
- Health department roles sometimes involve significant administrative and reporting obligations that reduce direct patient care time.
- School-based health centers operate on academic calendars, which can limit year-round employment or continuity of care.
- Mobile clinics often face resource constraints, including limited diagnostic equipment and inconsistent supply chains.
- Nonprofit and NGO budgets can be grant-dependent, creating job instability when funding cycles shift.
- Many public health settings rely on outdated electronic health record systems, adding documentation frustration.
- Rural or underserved placement sites may require lengthy commutes or relocation, affecting work-life balance.
Public Health Nurse Practitioner Salary and Job Outlook
The Bureau of Labor Statistics (BLS) reports salary data for all nurse practitioners nationwide, covering more than 307,000 professionals. While these figures reflect NPs across every specialty and setting, they offer a reliable baseline for public health NPs exploring compensation. Keep in mind that public health NPs may see base salaries slightly below hospital or specialty peers, but total compensation often tells a different story. Federal loan repayment programs such as the National Health Service Corps (NHSC) can provide up to $50,000 or more toward student loans, and many public health employers add generous retirement contributions, flexible scheduling, and pension plans that do not appear in base salary figures.
| Salary Percentile | Annual Salary |
|---|---|
| 25th Percentile | $109,940 |
| National Median | $129,210 |
| 75th Percentile | $149,570 |
| National Mean | $132,000 |
NP Salary by State
Nurse practitioner salaries vary significantly depending on where you practice. The table below shows state-level salary data from the Bureau of Labor Statistics (2024) for all nurse practitioners. Keep in mind that public health NP salaries are not tracked separately, so these figures reflect the broader NP workforce. States marked with full practice authority (FPA) allow NPs to evaluate, diagnose, and treat patients independently, which is especially relevant for public health NPs who need autonomy to serve underserved communities.
| State | Total NPs Employed | Median Salary | Mean Salary | 25th Percentile | 75th Percentile | Full Practice Authority |
|---|---|---|---|---|---|---|
| California | 20,980 | $166,610 | $173,190 | $140,260 | $205,400 | No |
| New Jersey | 9,590 | $149,620 | $140,470 | $126,030 | $162,250 | No |
| Alaska | 570 | $145,450 | $142,340 | $104,000 | $165,510 | Yes |
| New York | 20,430 | $145,390 | $148,410 | $128,190 | $164,670 | Yes |
| Oregon | 2,430 | $144,600 | $148,030 | $129,840 | $163,240 | Yes |
| Washington | 4,790 | $140,220 | $143,620 | $125,890 | $161,730 | Yes |
| Connecticut | 3,680 | $138,960 | $141,140 | $125,910 | $159,680 | Yes |
| Massachusetts | 8,920 | $138,890 | $145,140 | $125,590 | $160,310 | Yes |
| New Mexico | 1,870 | $138,440 | $136,620 | $113,240 | $156,000 | Yes |
| Arizona | 7,540 | $133,790 | $132,920 | $115,290 | $151,650 | Yes |
| Montana | 1,050 | $133,640 | $131,560 | $112,180 | $141,050 | Yes |
| New Hampshire | 1,790 | $132,440 | $133,660 | $120,270 | $143,010 | Yes |
| District of Columbia | 790 | $131,380 | $137,600 | $119,240 | $143,960 | Yes |
| Hawaii | 470 | $130,940 | $135,020 | $121,410 | $158,100 | Yes |
| Rhode Island | 1,200 | $130,710 | $139,600 | $126,200 | $160,030 | Yes |
| Texas | 21,690 | $129,880 | $130,930 | $110,570 | $143,860 | No |
| Colorado | 4,130 | $129,750 | $127,610 | $110,300 | $139,440 | Yes |
| Vermont | 680 | $129,740 | $130,580 | $115,650 | $139,930 | Yes |
| Iowa | 2,810 | $129,420 | $133,020 | $115,950 | $137,900 | Yes |
| Florida | 24,690 | $129,010 | $128,340 | $109,670 | $143,670 | No |
| Idaho | 1,570 | $128,940 | $131,380 | $119,290 | $140,920 | Yes |
| Illinois | 9,560 | $128,620 | $128,880 | $111,450 | $138,420 | No |
| Wisconsin | 4,950 | $128,580 | $130,490 | $117,630 | $137,150 | No |
| Minnesota | 8,690 | $128,570 | $128,120 | $103,250 | $139,590 | Yes |
| Indiana | 7,470 | $128,280 | $126,520 | $111,210 | $134,840 | Yes |
The Bureau of Labor Statistics projects nurse practitioner employment to grow 46 percent from 2023 to 2033, making it one of the fastest growing occupations in the country. Much of that demand is tied directly to expanding public health infrastructure, where NPs are increasingly essential for connecting clinical care to community wellness.
Common Questions About Public Health Nurse Practitioners
If you are considering a move into public health practice, you probably have questions about scope, salary, and the path forward. Below are answers to the questions nurses ask most often about this rewarding specialty.
- What is the difference between a public health nurse and a nurse practitioner?
- A public health nurse (PHN) typically holds a BSN and focuses on population-level health education, disease prevention, and community outreach. A nurse practitioner in public health holds a graduate degree (MSN or DNP), can diagnose and treat patients, prescribe medications, and often leads clinical programs within underserved communities. The NP's advanced scope of practice allows for direct patient care alongside broader public health strategy.
- How do you become a public health nurse practitioner?
- Start by earning your BSN and obtaining RN licensure, then gain clinical experience, ideally in community or primary care settings. Next, complete an MSN or DNP program with a focus on family, adult-gerontology, or population health. After graduating, pass a national certification exam through ANCC or AANP. Adding credentials such as the Advanced Public Health Nursing certification from ANCC can further strengthen your qualifications.
- What are clinical-community linkages in nursing?
- Clinical-community linkages are the connections between healthcare delivery systems and community organizations such as food banks, housing agencies, schools, and social services. In nursing, these linkages ensure patients receive coordinated support beyond the exam room. Nurse practitioners play a key role by screening for social determinants of health, making referrals to local resources, and following up to close gaps in care that clinical settings alone cannot address.
- How much do public health nurse practitioners make?
- According to the Bureau of Labor Statistics, the median annual salary for nurse practitioners across all specialties was approximately $126,260 as of the most recent data. Public health NPs may earn slightly more or less depending on geography, employer type, and experience. Those working in federally qualified health centers or government agencies may also receive additional benefits such as loan repayment, boosting overall compensation.
- Why are nurse practitioners important in community health?
- Nurse practitioners help close critical access gaps in communities facing provider shortages, particularly in rural and underserved urban areas. Their training in holistic, patient-centered care makes them well suited to address chronic disease management, preventive screenings, and behavioral health needs. NPs also build trust with populations that may avoid traditional healthcare settings, improving engagement and long-term health outcomes across entire communities.
- Do public health NPs qualify for loan repayment programs?
- Yes. Nurse practitioners who work in Health Professional Shortage Areas (HPSAs) or at qualifying nonprofit or government sites are often eligible for federal programs such as the National Health Service Corps (NHSC) Loan Repayment Program, which can cover a significant portion of student debt. Many states also offer their own loan forgiveness incentives. Check current eligibility requirements through NHSC and your state's health department.