Most important takeaways…
- Nearly 30 percent of family NP graduates now take their first job outside primary care settings.
- Burnout, excessive documentation demands, and rigid scope of practice laws push NPs away from primary care faster than low pay alone.
- Specialty NPs consistently outearn primary care NPs, with gaps often reaching 15 to 25 percent depending on the role.
- States granting full practice authority report stronger NP retention in primary care than restricted practice states.
Federal workforce data show that the share of NPs practicing in primary care has slipped from roughly 70% to under 60% over the past decade, even as new NP graduates hit all-time highs. That gap lands squarely in the career decisions of working nurses: should you pursue a family NP path despite mounting burnout reports, or pivot toward a specialty with higher pay and more predictable schedules? This tension now defines the primary care landscape. The numbers confirm a steady migration, but the drivers go deeper than the paycheck. Recognizing the patterns behind this exodus helps you weigh your own next step without ignoring what the data says about retention, autonomy, and long-term satisfaction.
How Many NPs Are Actually Leaving Primary Care?
Understanding the exact number of nurse practitioners leaving primary care requires pulling together multiple data sources. No single survey captures the complete picture, but together, federal workforce statistics, professional association surveys, and academic placement outcomes reveal a clear trend: primary care is losing ground.
National Survey Trends Show a Decline
The American Association of Nurse Practitioners (AANP) conducts a National NP Sample Survey every two to three years. In 2016, self-reported data indicated that close to three-quarters of NPs identified primary care as their main practice setting. By the most recent survey cycles, that figure had dropped below two-thirds, with the fastest declines occurring in family practice and adult primary care settings. While the absolute number of NPs in primary care has still grown (thanks to a booming overall NP workforce) the proportion has steadily eroded.
Federal Workforce Projections Paint a Long-Term Picture
The Health Resources and Services Administration (HRSA) models future supply and demand for health care professionals. Recent projections suggest that while the overall NP workforce will expand significantly through 2025 and beyond, demand in specialty areas such as acute care, psychiatry, and cardiology is growing at a faster clip than in primary care. HRSA's data also highlights regional variation: medically underserved areas often still rely heavily on primary care NPs, but even there, specialty roles are expanding as hospital systems grow.
New Graduates Are Choosing Different Paths
Many universities that offer family nurse practitioner (FNP) programs publicly report where their graduates work after licensure. An increasing share of FNP graduates are accepting positions in specialty clinics, emergency departments, or hospitalist groups rather than traditional primary care offices. While FNP education remains rooted in family-centered primary care, the job market is pulling talent toward highest paid NP specialties. Graduation surveys across multiple large programs show that the percentage of new FNPs who plan to work exclusively in primary care has fallen by 10 to 15 percentage points over the past decade.
What BLS Employment Data Tells Us
The Bureau of Labor Statistics (BLS) Occupational Employment Statistics tracks NPs by industry code. Between 2016 and 2025, the fastest-growing employment sectors for NPs were specialty hospitals, outpatient surgical centers, and psychiatric facilities. While offices of physicians (which include both primary and specialty care) remain the largest employer, growth there has been slower than in specialty inpatient settings. The BLS data does not separate primary care from specialties within physician offices, but the overall shift toward hospital-based employment signals that fewer new graduates are opting for traditional community-based primary care.
Taken together, these sources indicate that while a majority of NPs still practice in primary care, that majority is shrinking. The field is not losing providers overnight, but the long-term trajectory points toward a more specialty-heavy workforce. For working nurses considering advanced practice, understanding this trend can help clarify where jobs are growing. It can also reveal where retention challenges may create unique nurse practitioner advancement opportunities.
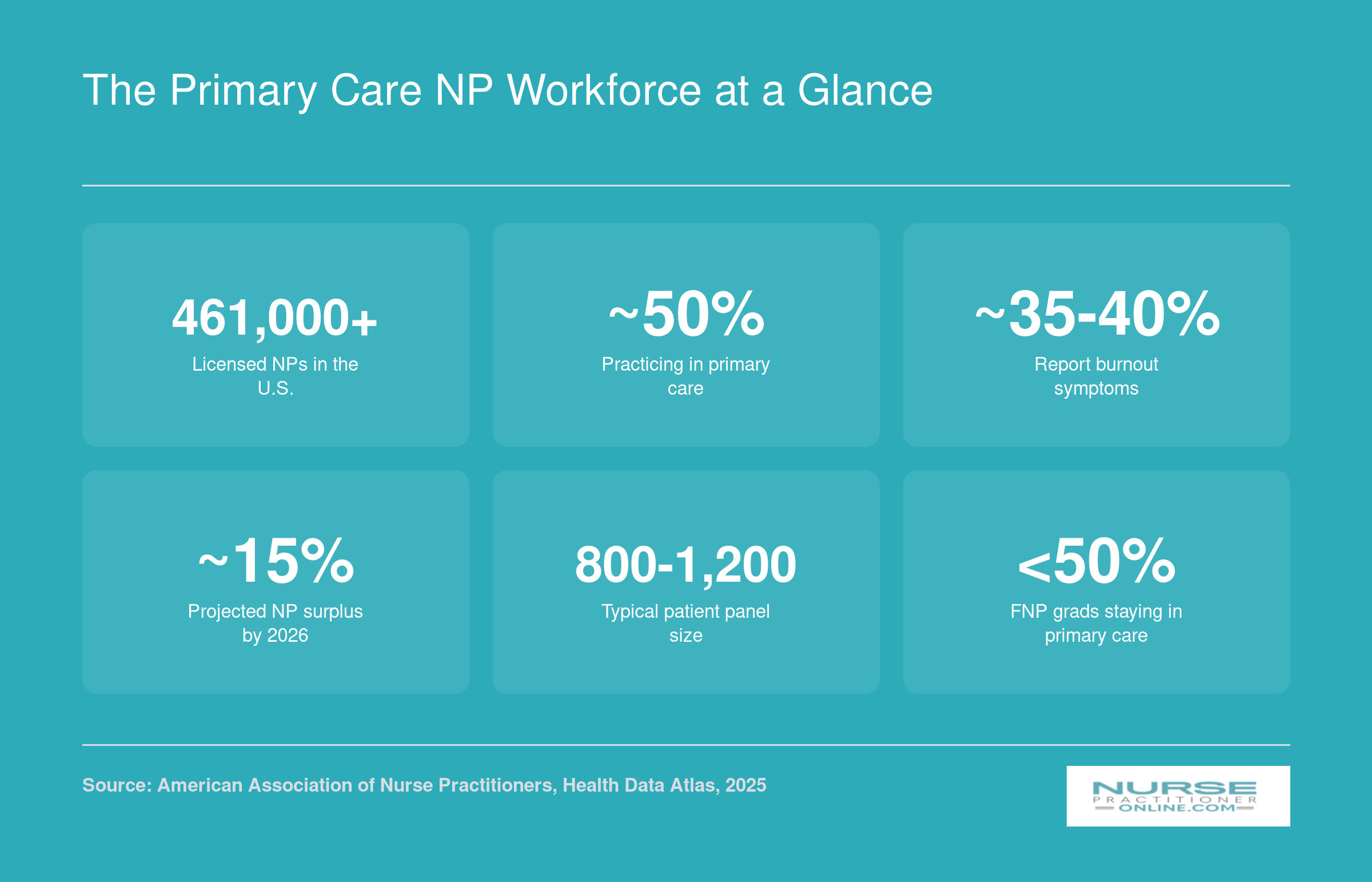
The Primary Care NP Workforce at a Glance
Before we explore why nurse practitioners are leaving primary care, here is a snapshot of the current landscape. Some of these figures are widely cited estimates rather than precise counts, so treat them as useful guideposts rather than exact benchmarks.
Push Factors: Burnout, Workload, and Administrative Burden
Higher pay in specialty roles attracts attention, but many primary care NPs are not simply chasing bigger paychecks. They are fleeing unsustainable working conditions. Understanding these push factors helps explain why retention efforts that focus only on salary often fall short.
Burnout Is Widespread and Persistent
National survey data from 2022 revealed that more than 60 percent of nurse practitioners reported experiencing burnout, with 30 percent reporting both burnout and depression.1 This was not a fleeting problem: 62 percent of those affected said their burnout had lasted at least one year, and 20 percent reported suffering for more than two years.1 Earlier research focused specifically on primary care NPs in New Jersey and Pennsylvania found burnout prevalence around 25 percent, suggesting that the pandemic significantly worsened conditions across the profession.2
The consequences extend beyond personal well-being. That same 2022 survey found 31 percent of nurse practitioners were considering leaving healthcare entirely, and 25 percent had already changed work settings specifically because of burnout.1 When a quarter of your workforce is actively relocating to escape their current conditions, that signals a systemic problem rather than individual weakness.
Administrative Burden Tops the List
When nurse practitioners identify what drives their burnout, bureaucratic tasks consistently rank highest. Nearly half (49 percent) cited administrative burden as a primary contributor to their exhaustion.1 Documentation requirements for electronic health records consume significant portions of each patient visit, and prior authorization requests add hours of unpaid labor each week.
Other major factors included:
- Insufficient compensation: 43 percent identified pay that does not match workload demands1
- Lack of respect: 43 percent reported feeling undervalued by employers and healthcare systems1
- Growing patient panels: Primary care clinics often assign more patients per provider to offset staffing shortages
Research also shows that burnout directly erodes care quality. Primary care NPs experiencing burnout were far less likely to perceive that they delivered high-quality care, with an odds ratio of just 0.15.3 For primary care nurse practitioners already stretched thin, this disconnect between professional standards and daily reality becomes a powerful reason to leave.
Post-COVID Acceleration
The pandemic intensified pressures that already existed. Patient acuity increased as people delayed care during lockdowns and arrived sicker. Staffing gaps that opened in 2020 and 2021 never fully closed, leaving remaining providers to absorb higher volumes. Many NPs describe moral injury from working in systems that prioritized throughput over quality during the crisis.
Research on primary care NPs in the Veterans Health Administration offers one hopeful note: facilities that implemented full practice authority saw burnout decrease by six percentage points.4 This suggests that reducing bureaucratic obstacles and granting professional autonomy can meaningfully improve retention, a topic we will explore further when discussing state practice authority.
Questions to Ask Yourself
Primary Care vs. Specialty NP Salaries
Compensation is one of the most frequently cited reasons nurse practitioners transition away from primary care. While exact salary figures vary by source and year, the available data consistently shows that specialty NPs tend to outearn their primary care counterparts. The figures below draw on 2023 BLS data for all NPs nationally and 2025 compensation reports for specialty and family NP roles. Keep in mind that specialty salary data outside of cardiology and family practice is limited in current reporting, so ranges for other specialties are not included here to avoid presenting uncertain numbers as fact.
| NP Role or Setting | Average or Median Annual Salary | Data Year | Source Type |
|---|---|---|---|
| All Nurse Practitioners (National Median) | $129,210 | 2023 | Bureau of Labor Statistics |
| All Nurse Practitioners (National Mean) | $132,000 | 2023 | Bureau of Labor Statistics |
| All Nurse Practitioners (25th Percentile) | $109,940 | 2023 | Bureau of Labor Statistics |
| All Nurse Practitioners (75th Percentile) | $149,570 | 2023 | Bureau of Labor Statistics |
| Family Nurse Practitioner (Median) | $125,000 | 2025 | Industry Compensation Reports |
| Family Nurse Practitioner (Mean) | $129,976 | 2025 | Industry Compensation Reports |
| Family Nurse Practitioner (Low End of Range) | $105,898 | 2025 | Industry Compensation Reports |
| Cardiology Nurse Practitioner (Mean) | $136,846 | 2025 | Industry Compensation Reports |
| Interventional Cardiology NP (Mean) | $131,450 | 2025 | Industry Compensation Reports |
| Cardiothoracic Surgery NP (Mean) | $124,627 | 2025 | Industry Compensation Reports |
| All NPs, Average Total Compensation | $144,509 | 2025 | Industry Compensation Reports |
| All APRNs, Average Total Compensation | $133,000 | 2025 | Industry Compensation Reports |
Pull Factors: Higher Pay, Better Schedules, and Professional Growth
While burnout pushes NPs out of primary care, attractive incentives in specialty fields actively pull them in. Understanding these pull factors is essential for NPs weighing whether to stay in primary care or explore other options.
The Salary Advantage Is Real
The compensation gap between primary care and specialty NP roles is significant and widening. According to recent workforce surveys, psychiatric mental health NPs earn between $15,000 and $25,000 more annually than family NPs in the same geographic region. The differential is even larger in high-demand specialties: dermatology NPs routinely command $20,000 to $30,000 premiums, while acute care NPs in intensive care or emergency settings can see salary bumps of $25,000 to $40,000 or more compared to their primary care colleagues. You can see these figures broken down further across the highest paid nurse practitioner specialties.
For NPs carrying student loan debt or supporting families, these differences translate into years of faster financial progress. A $30,000 annual gap means an extra quarter-million dollars over a ten-year career, making specialty roles difficult to ignore purely on economic grounds.
Schedule Predictability and Work-Life Balance
Beyond the paycheck, many specialty NPs report dramatically better control over their time. Dermatology and aesthetic medicine roles typically operate Monday through Friday with minimal evening or weekend coverage. Psychiatric NPs working in outpatient practices often set their own appointment calendars and avoid the urgent panel add-ons that plague primary care.
Acute care roles may involve shift work, but those shifts are clearly defined. You clock in, deliver high-acuity care, and clock out with minimal chart documentation spilling into evenings at home. Primary care, by contrast, often means scheduled patient hours followed by two to three hours of inbox management, prior authorizations, and quality metric documentation.
Professional Growth and Autonomy
Specialty NPs frequently describe clearer pathways for advancement. Dermatology NPs develop procedural skills in biopsies, cryotherapy, and cosmetic injections that create tangible expertise markers. Psychiatric NPs build psychotherapy competencies and medication management depth that position them as true specialists rather than generalists. If you're considering a transition into psych, our guide on how to transition from FNP to PMHNP walks through the steps.
Many specialty roles also offer greater clinical autonomy. Once you develop proficiency in a focused domain, collaborating physicians and health systems often grant wider latitude for independent decision-making than the protocol-heavy environment common in primary care networks. For NPs wondering whether additional credentials justify the investment, it's worth exploring whether a DNP is worth it for long-term career positioning.
The Telehealth Pull
Psychiatric and dermatology NP positions increasingly offer fully remote work options, a flexibility primary care has been slower to adopt at scale. Telepsychiatry platforms allow NPs to practice across state lines (in states with full practice authority or interstate compacts), set their own hours, and eliminate commutes entirely. Teledermatology is growing rapidly for consult and follow-up visits. Primary care, with its emphasis on physical exams, preventive screenings, and hands-on acute care, remains more tethered to in-person delivery and brick-and-mortar clinic schedules.
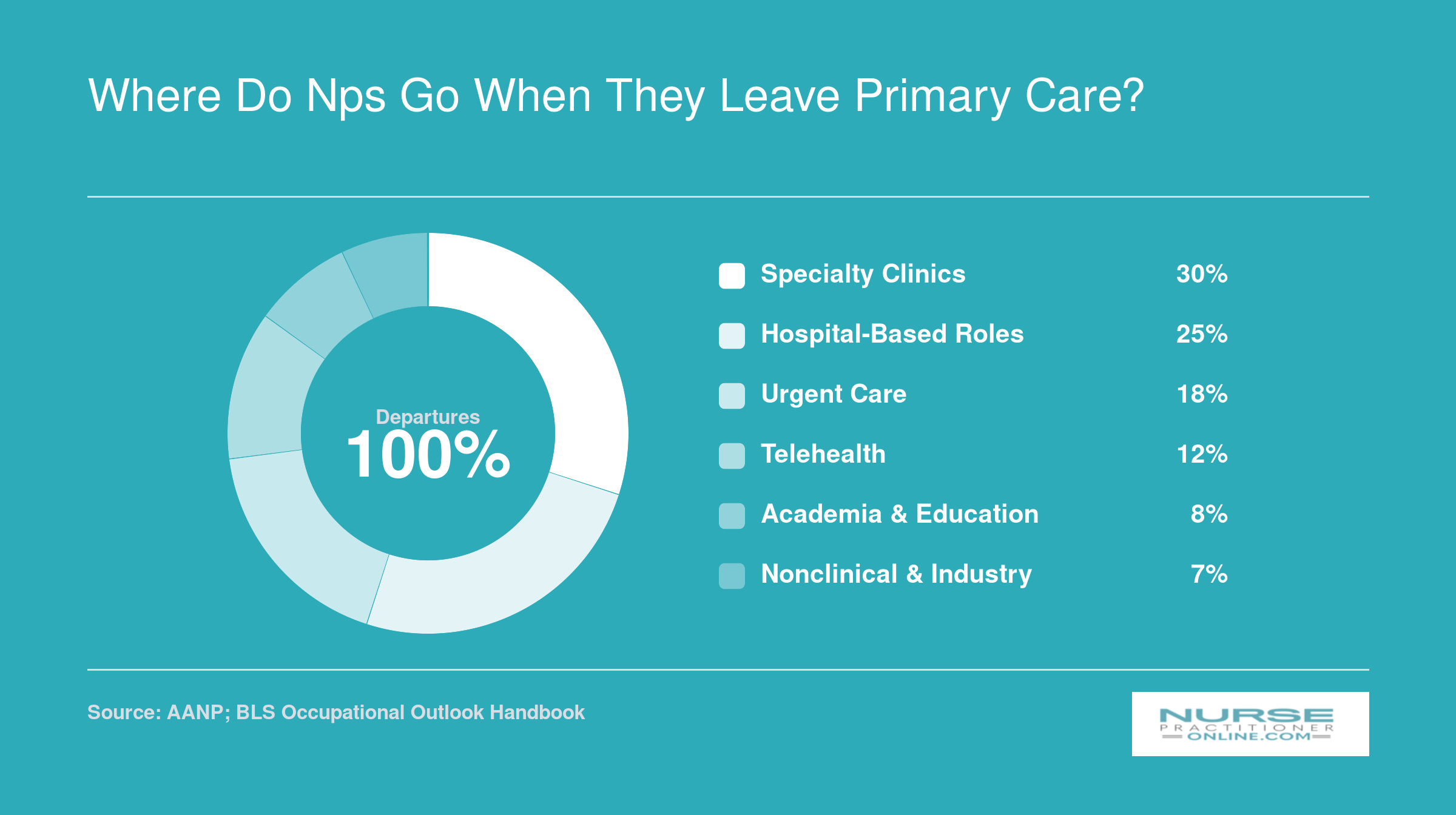
Where Do NPs Go When They Leave Primary Care?
Detailed 2026 practice setting data from the AANP is still being collected, so exact percentages are not yet available. However, workforce surveys and job market trends consistently point to the same destinations. To explore the most current data yourself, check the BLS Occupational Outlook Handbook for national employment projections, review annual AANP practice reports once released, browse university nursing program alumni career outcomes pages, and filter job boards like Indeed or LinkedIn by setting to see which roles are actively hiring NPs.
Related Articles
How State Practice Authority Affects NP Retention in Primary Care
Your ability to practice at the top of your license, without administrative headaches, can make or break a career in primary care. When state law forces you to pay for a collaborating physician or limits your prescriptive authority, the daily grind of primary care feels heavier, and the pull of specialty settings, where physician oversight is already built into the team structure, grows stronger.
The Three Tiers of NP Practice Authority
States fall into three categories. Full practice states let you evaluate, diagnose, interpret tests, and prescribe under the sole authority of the state board of nursing, with no required physician supervision.2 Reduced practice states impose some collaborative agreement for prescribing or a subset of clinical activities, while restricted practice states demand continuous physician supervision or delegation for the full scope of NP care. As of 2026, approximately 30 states, the District of Columbia, and two U.S. territories have adopted full practice authority, with the remainder operating under reduced or restricted models. You can review the current landscape in our nurse practitioner practice authority by state guide.
Data Linking Full Practice Authority to Primary Care Retention
Research shows a clear relationship between FPA and where NPs choose to work. During the 2010 to 2018 study period, 29% of NPs in full-practice states worked in primary care Health Professional Shortage Areas (HPSAs), compared to just 22% in non-FPA states.1 Adopting FPA increased the probability of an NP practicing in a shortage area by 30.5% overall, and by 46.5% for those working full time.1 Self-employment rates tell a similar story: FPA states saw a 176.8% jump in self-employed NPs, suggesting more independent primary care practices.1 These patterns indicate that when full authority exists, NPs are more likely to enter and stay in primary care.
How Restrictions Hamper Primary Care Retention
In reduced- or restricted-practice states, collaborative agreements create financial and administrative friction. Paying a collaborating physician several thousand dollars per month cuts directly into a primary care nurse practitioner's already modest income, while specialty clinics often absorb or integrate these costs. Scope limitations also breed frustration: you went to school to manage complex cases, yet you're forced to route everyday decisions through a physician. That underutilization fuels burnout and makes the switch to specialty practice, where oversight is less of a hurdle, seem like the logical next step.
Recent Legislative Gains as a Retention Lever
Since 2020, more states have embraced full practice authority as a policy lever to keep NPs in primary care. South Dakota's 2017 move to FPA, for instance, has been followed by expansions in states like Massachusetts and Delaware.2 Each expansion chips away at the barriers that push primary care NPs toward specialty roles, and early workforce data suggest that granting full authority helps redistribute NPs into areas of greatest need. For a closer look at which states have recently changed their laws, see our independent nurse practitioner states analysis. For working nurses considering the NP path, practicing in an FPA state can mean the difference between a rewarding primary care career and a stressful one that feels unsustainable.
What Could Bring NPs Back to Primary Care?
The debate on retaining NPs in primary care often splits between two paths: simply raising paychecks or fundamentally redesigning the job. The data suggests we need both, and a lot more.
Closing the Pay Gap
While salary alone won't solve the exodus, it remains the most immediate lever. Some health systems are now experimenting with compensation parity, where primary care NPs earn the same base salary as their specialty peers, supplemented by productivity bonuses tied to quality metrics rather than volume. Loan repayment programs like the National Health Service Corps (NHSC) also show promise: service-obligated clinicians are about 30% less likely to leave underserved areas compared to those without obligations.1 However, overall retention among NHSC participants still sits at only 29%, compared to 52% for non-obligated providers, suggesting financial incentives must be paired with workplace improvements to truly move the needle.1
Redesigning the Workload
Burnout isn't just about long hours; it's about how those hours are spent. Team-based care models that add scribes, medical assistants, and dedicated administrative support can dramatically reduce the clerical burden that drives many NPs to specialty roles. Practices that cap panel sizes and carve out non-visit time for documentation have seen improved job satisfaction. The most successful redesigns treat the NP as a clinical decision-maker, not a documentation clerk, directly targeting the administrative fatigue highlighted earlier.
Full Practice Authority as a Retention Tool
As discussed in the state practice authority section, NPs in states with full practice authority report greater professional autonomy and satisfaction. When NPs can practice to the full scope of their training, ordering tests, prescribing, and managing panels without physician oversight, they're more likely to see primary care as a long-term career, not a stepping stone. Legislative expansion isn't just a patient-access issue; it's a retention tool. If you're interested in shaping these policies, the nurse practitioner health policy toolkit offers a practical starting point.
Hybrid Roles That Blend Passions
Letting NPs develop a clinical focus within primary care, such as leading a diabetes management clinic or integrating behavioral health, can offer the professional growth that might otherwise pull them into a full specialty shift. These hybrid roles recognize that primary care is broad enough to accommodate deep interests without forcing a complete departure.
Starting Stronger: The Pipeline Solution
Finally, NP programs can do more to prepare graduates for a sustainable primary care career. This means longer, high-quality clinical rotations in well-supported primary care sites, mentorship programs that continue into the first years of practice, and curricula that emphasize business literacy and burnout resilience. Choosing best online MSN nurse practitioner programs with robust clinical placement support is one way new students can set themselves up for long-term success. Early exposure to effective team models can shift new grads' expectations from survival mode to a career they're eager to sustain.
What This Trend Means for Your NP Career Path
The migration of nurse practitioners away from primary care does not make family medicine a poor career choice. It simply means you should choose your specialty with intention, weighing your financial needs, lifestyle goals, and professional interests against the realities of each practice setting.
If You're Choosing Between FNP and Specialty Programs
Family nurse practitioner programs still offer the broadest scope of practice and the most geographic flexibility. If you value career optionality above all else, an FNP degree keeps more doors open than any specialty track. The data in this article simply reinforces that you should enter primary care with your eyes open to the trade-offs: lower base pay but often richer benefits, higher administrative burden but greater patient continuity, and limited specialty income potential but strong federal and state loan forgiveness programs.
Before you commit to a specialty NP track based solely on salary figures, calculate total compensation. A primary care NP earning $110,000 with $30,000 in annual loan forgiveness, four weeks of paid time off, and a Monday-through-Friday schedule may enjoy better financial and personal outcomes than a specialty NP earning $135,000 with no forgiveness, irregular shifts, and higher student debt.
If You're Already in Primary Care
Current primary care NPs hold unusual leverage in 2026. The shortage is real, and employers know it. Use this article's data points when negotiating contracts: request sign-on bonuses, higher base pay, reduced patient panels, protected administrative time, or expanded CME budgets. If your employer resists, remember that competing practices and health systems are actively recruiting primary care NPs.
Next Steps
Compare nurse practitioner program types to understand how online nursing programs arrange local clinical placements and how curriculum differs across specialties. Research your state's practice authority laws, since full practice authority directly affects your autonomy and earning potential in primary care. Finally, explore salary data specific to your target specialty and geographic region, and consider whether a DNP is worth it for your long-term goals, before making any program commitment.
Frequently Asked Questions About NPs in Primary Care
These are some of the most common questions working nurses and NP students ask about the primary care workforce. Each answer draws on data and themes explored throughout this article.
- How many nurse practitioners currently work in primary care?
- Estimates suggest that roughly half of all nurse practitioners practice in primary care settings, though that share has been gradually declining. The American Association of Nurse Practitioners reports that family, adult, and pediatric primary care NPs still represent the largest segment of the profession. However, workforce surveys show a measurable shift toward specialty and acute care roles over the past decade.
- What is the burnout rate for nurse practitioners in primary care?
- Studies indicate that burnout affects a significant portion of primary care NPs, with some surveys placing the rate above 50 percent. Contributing factors include heavy patient panels, administrative documentation burdens, and limited organizational support. As discussed earlier in this article, burnout is one of the strongest push factors driving NPs away from primary care into specialty or non-clinical roles.
- Do nurse practitioners earn more in specialty practice than primary care?
- In most cases, yes. National salary data consistently shows that NPs in specialties such as psychiatry, dermatology, and acute care earn meaningfully more than their primary care counterparts. The gap can range from $10,000 to $30,000 or more annually depending on the specialty, geographic region, and practice setting, as outlined in the salary comparison earlier in this article.
- What states have full practice authority for nurse practitioners?
- As of 2026, more than half of U.S. states and the District of Columbia grant full practice authority, allowing NPs to evaluate, diagnose, and prescribe independently. States that restrict NP autonomy through collaborative or supervisory agreements tend to see lower NP retention in primary care, since limited scope can reduce both job satisfaction and earning potential.
- Can a family nurse practitioner work in a specialty?
- Family nurse practitioners (FNPs) can work in certain specialty settings, but their scope depends on state regulations, employer requirements, and additional training. Some FNPs transition into urgent care, dermatology, or occupational health. However, specialties like psychiatry or neonatal care typically require a dedicated post-master's certificate or a different NP certification altogether.
- What is being done to address the primary care NP shortage?
- Efforts include expanding loan repayment programs for NPs who commit to primary care, broadening full practice authority legislation, and increasing residency and fellowship opportunities in underserved areas. Some health systems are also restructuring primary care workflows to reduce administrative burden. As explored earlier in this article, improving compensation parity and workplace conditions are widely viewed as essential retention strategies.