Most important takeaways…
- Over half of U.S. states and Washington, D.C. now grant nurse practitioners full practice authority to serve as independent PCPs.
- NPs deliver routine physicals, chronic disease management, prescriptions, referrals, and preventive screenings comparable to physician primary care.
- The BLS projects 40 percent job growth for nurse practitioners between 2024 and 2034, far exceeding the national average.
- Medicare, most Medicaid plans, and major private insurers allow patients to formally designate an NP as their primary care provider.
Yes, a nurse practitioner can legally serve as your primary care provider in all 50 states. The degree of autonomous practice varies by state, but the legal and clinical foundation for NP-led primary care is firmly established nationwide.
A primary care provider handles preventive care, chronic disease management, prescription authority, and referrals to specialists. Nurse practitioners, who hold graduate-level clinical training and national board certification, meet every element of that definition. As of 2026, roughly 29 percent of practicing NPs work in primary care settings, filling critical gaps in a system where physician shortages are acute, particularly in rural and underserved communities.
The practical tension for patients and nurses alike is that NP autonomy is not uniform. A family NP in Oregon operates under full practice authority with no physician oversight requirement; that same NP in Texas works under a different regulatory structure. Understanding those distinctions matters whether you are choosing a provider or planning a career. If you are weighing DNP or MSN degree pathways, that choice can also shape the scope of your future practice.
NP Scope of Practice by State: Full Practice Vs. Restricted
The map of where nurse practitioners can work independently keeps shifting, with Utah, New York, Kansas, and Delaware all moving toward full practice authority in recent years and several other states actively debating bills in 2026 legislative sessions. Before you commit to an NP as your primary care provider, or before you choose where to practice as one, you need to know exactly what the rules look like in your state. For a deeper look at the forces driving these changes, see our overview of NP scope of practice: what's changing.
The American Association of Nurse Practitioners (AANP) sorts states into three categories: full practice, reduced practice, and restricted practice. Those labels carry real weight for how an NP can evaluate patients, order tests, manage chronic conditions, and write prescriptions without a physician co-signing the work.
Start With the AANP State Practice Environment Map
The AANP maintains a state practice environment map that is updated as legislation changes. It is the cleanest starting point because it color-codes every state and links to the underlying statutes. In full practice states, NPs evaluate, diagnose, order and interpret diagnostic tests, and prescribe (including controlled substances) under the exclusive licensure authority of the state board of nursing. In reduced practice states, at least one element of NP practice is limited and typically requires a regulated collaborative agreement with a physician. In restricted practice states, NPs need career-long supervision, delegation, or team management by another health provider to deliver care.
Confirm Details With Your State Board of Nursing
National summaries are a great orientation, but they sometimes lag behind a rule change or miss a nuance. Go directly to your state board of nursing website to verify two specifics: whether a written collaborative or supervisory agreement is required, and whether you have independent authority to prescribe Schedule II through V controlled substances. Some states grant full practice for most prescriptions but still restrict controlled substances, or require a transition-to-practice period (often 1,000 to 4,000 clinical hours) before independence kicks in. Our nurse practitioner practice authority guide breaks down these requirements in more detail.
Cross-Reference With a Second Source
Barton Associates publishes a state-by-state NP scope of practice guide that is useful as a secondary reference, particularly if you want a side-by-side comparison or you practice across state lines. For the most authoritative wording, cross-check against regulations posted by the National Council of State Boards of Nursing (NCSBN) or the actual statute citation from your state board. When three sources agree, you can act on it. When they disagree, the state board language wins. If you want to understand how recent policy momentum, including COVID-era waivers, has reshaped the landscape, our article on whether full practice authority is here to stay offers useful context.
What Services Can an NP Primary Care Provider Offer?
Choosing between a traditional physician primary care provider and a nurse practitioner often hinges on what services you expect from your PCP, but the practical reality is that NP primary care providers deliver nearly the full spectrum of routine and preventive care that patients need.
Core Primary Care Services
Nurse practitioners working in primary care independently perform annual physical exams, wellness visits, and chronic disease management for conditions such as diabetes, hypertension, asthma, COPD, and high cholesterol. They diagnose and treat acute illnesses like strep throat, sinus infections, UTIs, and bronchitis. NP PCPs order and interpret laboratory tests, imaging studies (X-rays, ultrasounds, MRIs), and EKGs, then use those results to guide treatment decisions. This is not collaborative practice shadowing a physician; in full-practice states, NPs manage these cases from intake through follow-up entirely on their own.
Prescriptive Authority
Nurse practitioners hold DEA registrations and prescribe medications across all therapeutic classes, including Schedule II through V controlled substances such as opioids, stimulants for ADHD, and benzodiazepines. The scope of prescriptive authority varies by state. A handful of states still impose collaborative agreement requirements or formulary restrictions, but the majority now grant NPs full prescribing privileges equivalent to physicians. For a detailed breakdown of current regulations, see this nurse practitioner practice authority state-by-state analysis. If you rely on a maintenance medication or periodic controlled-substance prescription, an NP can manage that regimen just as a physician would.
Preventive and Behavioral Health Services
NP primary care providers are trained to deliver comprehensive preventive services: immunizations, cancer screenings (referrals for mammograms and colonoscopies), cardiovascular risk assessments, depression and anxiety screening, and counseling for smoking cessation, weight management, and alcohol use. Many NPs integrate brief behavioral health interventions into routine visits, bridging the gap between primary care and mental health that often goes unaddressed in busy practices.
Referrals and Specialist Coordination
When you need specialty care, an NP PCP issues referrals with the same insurance network authority as a physician. Payers recognize NP referrals for orthopedics, cardiology, gastroenterology, and every other specialty. Understanding how primary care billing and coding works can help NPs ensure those referrals process smoothly. The referral process itself is identical to what a physician would initiate.
Scope-Appropriate Practice
Nurse practitioners refer patients for complex surgical procedures, high-acuity emergency interventions (trauma resuscitation, critical-care ventilator management), and specialist-only procedures (joint injections by orthopedists, endoscopy by gastroenterologists). This is not a limitation but scope-appropriate practice. Physicians in primary care refer the same cases to the same specialists. The difference lies in training focus, not competency within the primary care domain.
NP Vs. Doctor for Primary Care: Training, Cost, and Outcomes
Is an NP as effective as an MD for your day-to-day healthcare?
When you choose a primary care provider, you want someone who can manage your health skillfully without breaking the bank. Research comparing nurse practitioners and physicians in primary care shows remarkably similar results across key measures, with a few nuances worth knowing.
Training Paths: How Many Years?
The journey to independent practice looks different for each role. Nurse practitioners typically complete a Bachelor of Science in Nursing (BSN), gain direct patient care experience as an RN, then earn a Master of Science in Nursing (MSN) or Doctor of Nursing Practice (DNP). This pathway often spans six to eight years. Physicians take a longer route: a bachelor's degree, four years of medical school, and a residency program lasting three or more years. All told, physician training exceeds eleven years before independent practice.
Patient Outcomes: What the Research Shows
Across multiple studies, NP-led care delivers results on par with physician-led care:
- Blood pressure control: A 2023 analysis found average systolic readings of 133 mmHg for NP patients versus 135 mmHg for physician patients, with diastolic readings of 77 mmHg and 80 mmHg respectively.1
- Hospitalization rates: A 2018 Cochrane review noted no significant difference in how often patients are admitted to the hospital under NP care compared to physician care.3
- Overall quality: A 2023 broad outcome review concluded the quality of care is similar between the two provider types.2
One area where NPs consistently stand out is patient satisfaction. The same 2018 data showed higher satisfaction scores among patients seeing nurse practitioners.3 This often ties back to the nursing model's emphasis on holistic, patient-centered communication.
Cost Comparison: Is There a Difference?
Despite the longer and costlier training physicians undergo, the actual price tag for a primary care visit does not differ significantly between NP and physician providers. A 2023 study found no meaningful gap in visit costs.2 For patients with high-deductible plans or those paying out of pocket, this parity means you can choose based on fit rather than finances.
Once in practice, NPs looking to refine their clinical workflow may benefit from essential projects to improve primary care office flow. The growing body of evidence, including a Cochrane review and studies published through NIH, continues to affirm that NPs are safe, effective, and cost-neutral primary care options. Whether you prioritize a collaborative approach or simply need a trusted clinician, the research supports that an NP can meet your needs without compromise.
Related Articles
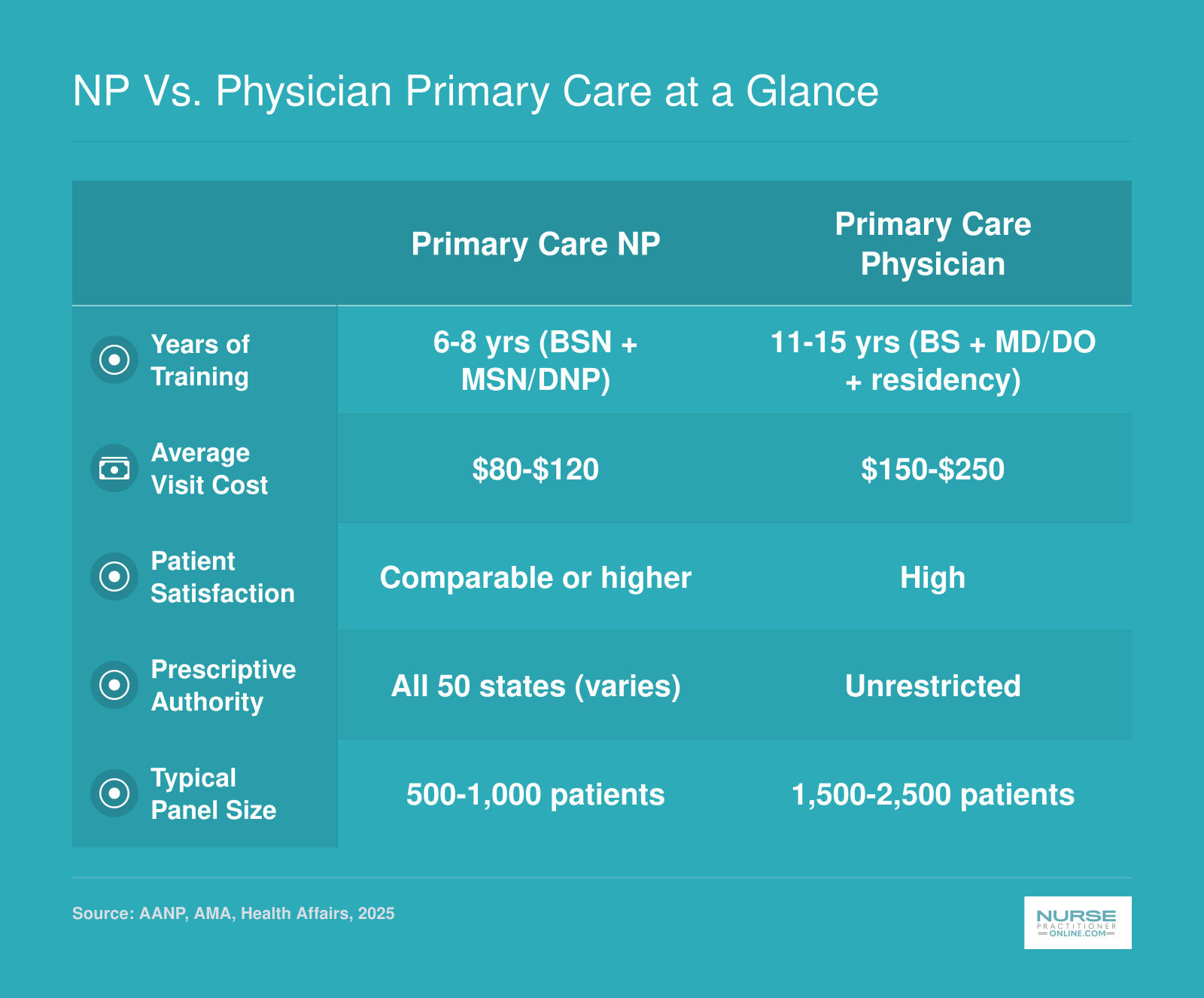
NP Vs. Physician Primary Care at a Glance
Nurse practitioners and physicians both deliver high-quality primary care, but they differ in training pathways, costs, and practice structure. This snapshot highlights the key distinctions to help you weigh your options.
Insurance, Medicare, and Medicaid: How to Designate an NP as Your PCP
Designating a nurse practitioner as your primary care provider means formally registering that NP with your health insurance plan so they become your go-to clinician for routine care, referrals, and care coordination. The process varies depending on whether you have Medicare, Medicaid, or private insurance, but the good news is that most plans now support NP designation.
Medicare Coverage for NP Services
Medicare Part B covers NP services at 85% of the physician fee schedule when the NP bills under their own National Provider Identifier.1 This means Medicare pays slightly less for the same service when an NP provides it independently compared to a physician. However, if an NP provides care under "incident-to" billing arrangements, where direct physician supervision is present in the office suite, Medicare reimburses at 100% of the physician rate.2
For Medicare Advantage plans, you can designate an NP as your primary care provider. CMS policy allows this designation, giving beneficiaries flexibility to choose the clinician who best fits their needs.3 If you prefer working with an NP for your ongoing care, confirm with your specific Medicare Advantage plan that the NP you want is listed as an available PCP option.
Medicaid Recognition Across States
All state Medicaid programs recognize nurse practitioners as primary care providers, though reimbursement rates differ significantly.3 Some states have enacted reimbursement parity mandates that require commercial insurers, and sometimes Medicaid, to pay NPs at the same rate as physicians for equivalent services. Oregon, Washington, New Mexico, Colorado, Nevada, and Arizona all have mandated parity for state-regulated commercial plans.3 If you receive Medicaid, check with your state's program to understand how NP visits are covered and whether any restrictions apply to your managed care plan. For a broader look at where NPs face the greatest demand, see states with the most need for nurse practitioners.
Private Insurance Policies
Most major private insurers allow members to designate an NP as their PCP. UnitedHealthcare, Anthem, Aetna, and Cigna all include NPs in their provider networks and typically permit PCP designation. The easiest way to verify is through your insurer's online provider directory, where you can filter specifically for nurse practitioners accepting new patients.
Regarding copays, patients generally pay the same amount whether they see an NP or a physician for a primary care visit. This copay parity is plan-dependent, so review your specific benefits summary or call member services to confirm.
Three Steps to Designate Your NP as PCP
- Search your plan's provider directory: Look up nurse practitioners in your area who are accepting new patients and participating in your network.
- Call your insurer to confirm: Reach member services to officially designate the NP as your primary care provider and verify there are no plan-specific restrictions.
- Schedule your first visit: Contact the NP's office to establish care, bring your insurance card, and request that your records transfer from any previous provider.
Questions to Ask Yourself
Which NP Specialties Work in Primary Care?
Four nurse practitioner specialties account for the vast majority of NPs serving as primary care providers in the United States, each with distinct patient populations and scopes of practice that determine who they can treat. For a broader look at all available tracks, explore Nurse Practitioner Specialties & Careers.
Family Nurse Practitioner: The Full-Lifespan Standard
The Family Nurse Practitioner is the most versatile and highest-demand primary care specialty. FNPs are trained to care for patients across the entire lifespan, from newborns to older adults, making them the only NP specialty that can serve as a primary care provider for an entire family. This full-spectrum scope explains why FNP programs consistently enroll more students than any other track and why most job postings for primary care NPs specify FNP certification. If your goal is to work as a PCP in the broadest range of settings with the fewest patient-age restrictions, FNP is the most common and most flexible pathway.
Adult-Gerontology Primary Care NP: Adolescents Through Seniors
The Adult-Gerontology Primary Care NP specialty prepares you to care for patients from adolescence through the end of life, typically starting around age 13. AGPCNPs cannot see young children, which limits their scope in family practice settings but makes them ideal for adult medicine clinics, geriatric practices, and primary care roles focused on chronic disease management in older populations. This specialty is a strong fit if you prefer working with adult and senior patients exclusively.
Pediatric Primary Care NP: Birth Through Young Adulthood
Pediatric NPs who complete the primary care track (PNP-PC) serve patients from birth through young adulthood, often into the early twenties. PNPs cannot see adult patients, so they work in pediatric clinics, school-based health centers, and family practices that have separate pediatric providers. If your passion is child health and development, the PNP-PC track positions you to be a primary care provider for children and teens.
Women's Health NP: Reproductive and Primary Care for Women
Women's Health NPs provide both reproductive health services and general primary care for women, typically from adolescence onward. WHNPs cannot serve male patients or young children, which narrows their PCP scope, but they are a vital part of primary care in women's health clinics and practices that integrate gynecological and preventive care. You can learn more about this track in our guide on the essential role of Women's Health Nurse Practitioners.
Specialties That Do Not Typically Serve as PCPs
Psychiatric-Mental Health NPs and Acute Care NPs generally do not function as primary care providers. PMHNPs focus on mental health diagnosis and medication management, though in some rural or underserved areas they may co-manage primary care needs when no other provider is available. In fact, NPs of all specialties are increasingly vital in those communities, as detailed in our article on how Nurse Practitioners are closing the healthcare gap in rural America. ACNPs are trained for hospital and critical care settings, not the outpatient continuity model that defines primary care.
Primary Care NP Salary and Job Outlook
Nurse practitioners are among the fastest growing occupations in the U.S., with the Bureau of Labor Statistics projecting 40% job growth for NPs between 2024 and 2034. That pace far outstrips the average for all occupations and reflects surging demand for primary care providers nationwide. The national median annual wage for nurse practitioners stood at $129,210 as of 2024, though earnings vary by specialty, setting, and geographic region. Primary care focused NPs may earn somewhat differently than NPs in acute or specialty settings, but detailed breakdowns by practice area are not yet published in federal wage data. The table below compares NP compensation with related nursing and healthcare roles to help you gauge the financial impact of advancing your career.
| Occupation | Total U.S. Employment | 25th Percentile Wage | Median Annual Wage | 75th Percentile Wage | Mean Annual Wage | Projected Growth (2024 to 2034) |
|---|---|---|---|---|---|---|
| Nurse Practitioners | 307,390 | $109,940 | $129,210 | $149,570 | $132,000 | 40% |
| Registered Nurses | 3,282,010 | $78,610 | $93,600 | $107,960 | $98,430 | N/A |
| Medical and Health Services Managers | 565,840 | $88,560 | $117,960 | $162,420 | $137,730 | N/A |
| Nursing Instructors and Teachers, Postsecondary | 74,250 | $62,210 | $79,940 | $102,020 | $87,090 | N/A |
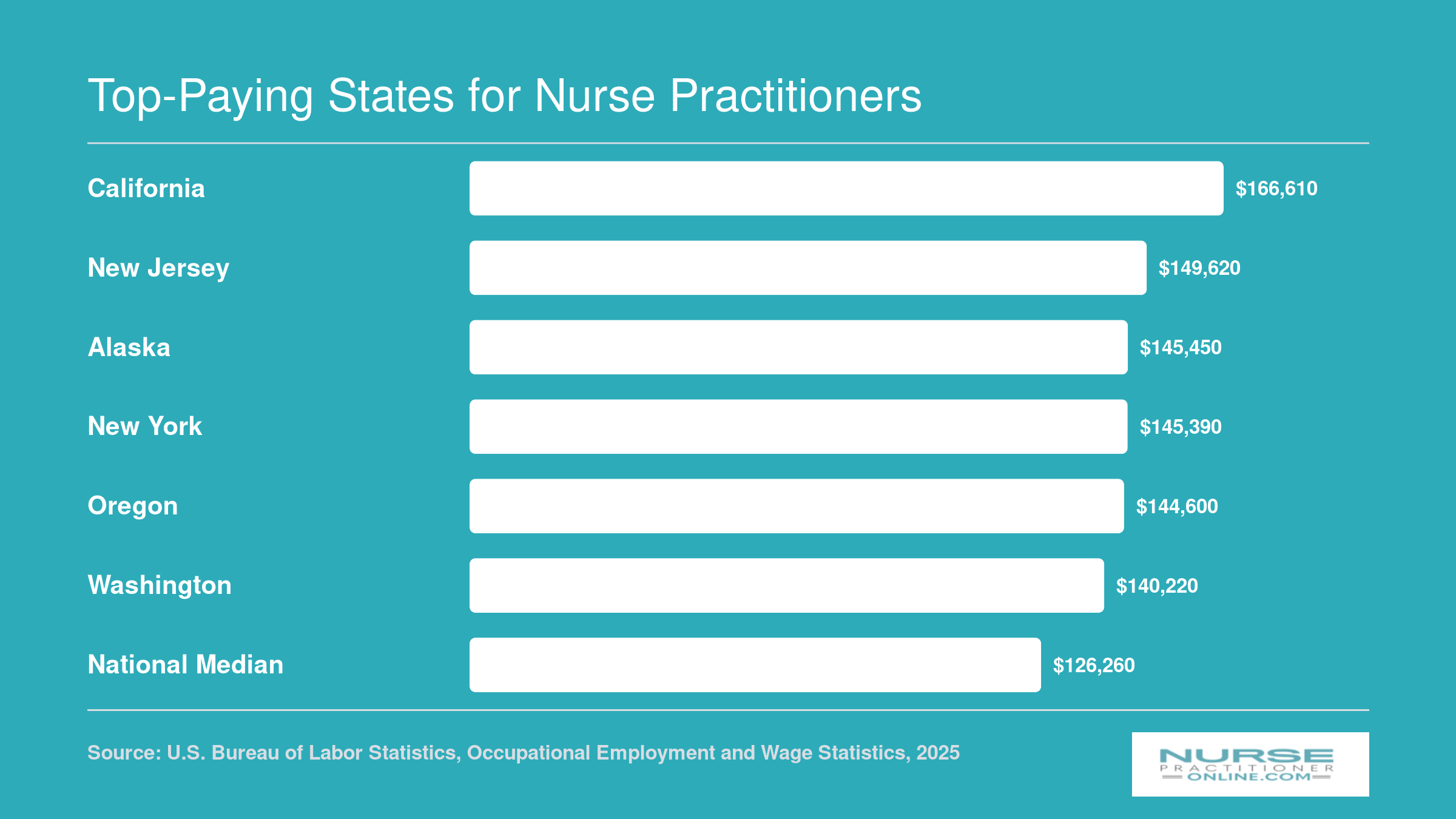
Top-Paying States for Nurse Practitioners
Where you practice can make a significant difference in your earning potential as a primary care NP. The following chart highlights the six highest-paying states for nurse practitioners by median annual salary, with the national median included as a baseline for comparison.
Did you know? As of 2026, 29 percent of nurse practitioners provide primary care, per Barton Associates. This underscores the vital role NPs play in expanding access, particularly in underserved areas where they often serve as the main healthcare provider.
Frequently Asked Questions About NPs as Primary Care Providers
Choosing a primary care provider is a big decision, and it is natural to have questions about what nurse practitioners can and cannot do in that role. Below are straightforward answers to the questions patients and nurses ask most often.
- Can a nurse practitioner be your primary care physician?
- A nurse practitioner can serve as your primary care provider, though the correct title is primary care provider rather than primary care physician. In states with full practice authority, NPs independently diagnose, treat, and manage ongoing health conditions without physician oversight. In restricted or reduced practice states, a collaborative agreement with a physician may be required, but the NP still functions as your day to day primary care clinician.
- Can nurse practitioners prescribe medication, including controlled substances?
- Yes. All 50 states and the District of Columbia grant nurse practitioners some level of prescriptive authority. In full practice authority states, NPs prescribe medications, including Schedule II through V controlled substances, independently. In states with reduced or restricted practice, a physician's involvement or a collaborative agreement may be needed for certain controlled substance prescriptions. Always confirm your state's current rules.
- What is the difference between a nurse practitioner and a doctor for primary care?
- Physicians complete medical school and residency, typically logging over 12,000 clinical hours before independent practice. Nurse practitioners earn a master's or doctoral nursing degree with roughly 500 to over 1,000 supervised clinical hours, then build expertise through practice. Research consistently shows comparable patient outcomes in primary care for both provider types, including patient satisfaction, chronic disease management, and preventive screening rates.
- Does insurance cover a nurse practitioner as your PCP?
- Most private insurers, Medicare, and Medicaid plans allow you to designate a nurse practitioner as your primary care provider. Medicare reimburses NPs at 85 percent of the physician fee schedule, though patients typically do not see a cost difference in their copays. Check your specific plan's provider directory to confirm your chosen NP is listed as an eligible PCP.
- What can a nurse practitioner do that a doctor cannot?
- Both providers share a wide overlap in primary care capabilities. However, NPs are specifically trained in a nursing model that emphasizes holistic, patient centered care, health promotion, and disease prevention education. Studies suggest NP visits often include more time spent on counseling, lifestyle guidance, and coordinating community resources. That said, physicians may offer broader procedural training in certain specialty areas.
- How do I find an NP accepting new patients as a PCP near me?
- Start with your insurance company's online provider directory and filter for nurse practitioners. You can also search the American Association of Nurse Practitioners' provider locator tool. Your state's board of nursing website lists licensed NPs, and many health system websites let you filter clinicians by provider type, specialty, and availability for new patients.
- Do NP primary care visits cost less than physician visits?
- In many cases, yes. NP led clinics and practices often have lower overhead, which can translate into reduced visit fees or copays. Medicare reimburses NPs at 85 percent of the physician rate, though patient out of pocket costs vary by plan. Multiple studies have found that NP provided primary care can lower overall healthcare spending, particularly through fewer emergency department referrals and shorter hospital stays.