Most important takeaways…
- NPs build on a BSN and nursing license, while PA programs accept any bachelor's degree with prerequisite coursework.
- Over 25 states plus Washington, D.C. grant nurse practitioners full practice authority to diagnose, treat, and prescribe independently.
- BLS median salaries for NPs and PAs differ by roughly $5,000 annually, with specialty and location influencing pay far more than credential.
- Working RNs can often complete online NP programs while employed, whereas most PA programs require full-time, in-person attendance.
Nurse practitioners and physician assistants both diagnose conditions, order tests, and prescribe medications, yet the two credentials emerge from entirely different professional traditions and require different entry points.
For working RNs, that distinction carries real weight. The NP route builds directly on your nursing license and clinical experience, while PA school treats applicants from all healthcare backgrounds equally and typically requires completing new science prerequisites regardless of prior training. The admissions gap matters: most accredited PA programs admit fewer than 10 percent of applicants, while many MSN and DNP programs are designed specifically for employed RNs.
As of 2026, over half of U.S. states grant nurse practitioners nurse practitioner practice authority by state, meaning no physician supervision or collaboration agreement is required. PAs, by contrast, practice under physician oversight in nearly every state, a structural difference that shapes hiring flexibility and long-term career independence more than salary data alone ever could.
NP Vs. PA at a Glance: Key Differences
Nurse practitioners and physician assistants fill similar clinical roles but emerge from distinct educational pathways and professional philosophies that shape their entire career.
Care Philosophy
- NP: Rooted in the nursing model, NPs emphasize holistic, patient-centered care that considers physical, emotional, and social factors.
- PA: Trained in the medical model, PAs focus on disease diagnosis and treatment, working closely with physicians in a team-based approach.
Education and Credentialing
- NP: Requires a Master of Science in Nursing (MSN) or Doctor of Nursing Practice (DNP). Most programs admit registered nurses with a Bachelor of Science in Nursing (BSN) and center on a population focus such as family or adult-gerontology. If you are considering the doctoral route, reviewing DNP prerequisites early can help you plan your timeline.
- PA: Requires a master's degree (MPAS, MSPA, or MPA) from an accredited physician assistant program. Admissions typically require a bachelor's degree with specific science prerequisites and direct patient care experience.
Clinical Training Hours
- NP: Clinical hours vary by program and specialization, typically ranging from 500 to 1,000 hours. DNP programs may include additional supervised practice.
- PA: Programs are standardized around 2,000 clinical hours across core rotations in primary care, emergency medicine, surgery, and other specialties.
Supervision and Autonomy
- NP: Scope of practice is determined by state law. Over half of U.S. states grant full practice authority, allowing NPs to evaluate, diagnose, and treat patients without physician oversight. Other states require a collaborative agreement.
- PA: PAs always practice under a supervising physician, though the required level of direct supervision varies by state and practice setting. Some states now use "collaboration" rather than "supervision" to describe the relationship.
Prescriptive Authority
- NP: Can prescribe medications independently in many states, including controlled substances, after obtaining a federal DEA number. In restricted states, a collaborative agreement may be needed for some prescriptions.
- PA: Prescribing authority is delegated by the supervising physician and varies by state. PAs can typically prescribe controlled substances with proper registration and oversight.
Specialization Approach
- NP: Education is population-focused from the start (e.g., family, psychiatric, pediatric). Additional certifications can be added later, but the initial role is narrowly defined.
- PA: Training is generalist, preparing PAs for any medical setting. They can switch specialties throughout their career without additional formal schooling, relying on on-the-job learning.
Understanding these foundational differences helps you choose the path that aligns with your professional values and career goals.
Education and Admissions: What Each Path Requires
Bachelor's in nursing versus bachelor's in any field: that single fork defines your first major decision point. For working RNs, the nurse practitioner route builds on a BSN and active RN license, skipping most prerequisite hoops. For candidates without a nursing degree, the physician assistant path requires a bachelor's in any major plus a rigorous menu of science prerequisites.
Prerequisites and Admissions Testing
NP programs require an RN license and BSN before you apply. Most ask for a minimum 3.0 GPA, and standardized tests (GRE, MAT) are increasingly optional or waived for experienced nurses. PA programs, by contrast, demand specific undergraduate science courses regardless of your bachelor's major. According to PAEA's 2021 curriculum report, these courses appear in the majority of PA program prerequisites:1
- Anatomy: required by 94 percent of programs
- Chemistry and physiology: each required by about 83 percent
- Microbiology: 80 percent
- Statistics: 74 percent
- Psychology: 61 percent
- Organic chemistry: 55 percent
- Biochemistry: 42 percent
- Genetics: 28 percent
Nearly half of PA programs still require the GRE.2 The University of Wisconsin, Madison PA program, for example, waives the GRE but expects a minimum 3.0 science GPA and a 3.2 overall GPA. The average accepted applicant at UW, Madison holds a 3.7 GPA.3 Nationally, PA matriculants cluster around a 3.5 cumulative average, making PA admissions highly selective.
Patient Care Experience Before Admission
About two-thirds of PA programs require documented patient care hours before you submit an application.2 AAPA data show the average minimum is 890 hours, though individual programs may ask for 1,000 to 3,000 hours. UW, Madison, for instance, requires at least 1,000 hours of hands-on patient care work (EMT, medical assistant, CNA, or similar roles).3 For RNs considering the PA track, your bedside experience usually satisfies this threshold. For non-nurses, this requirement adds months or years of prerequisite employment before you can even apply.
NP programs do not universally require clinical experience beyond the RN license itself, though many favor applicants with one to two years of bedside nursing.
Program Length and Clinical Hours
MSN-level family nurse practitioner programs typically run 2 to 3 years part-time or 18 to 24 months full-time, requiring 500 to 720 supervised clinical hours. DNP program length stretches to 3 or 4 years and may double the clinical requirement. PA programs follow a lockstep, full-time format averaging 27 months with more than 2,000 clinical rotation hours embedded in the curriculum.2 That gap matters: PA students log nearly three times the supervised clinical training of MSN NPs, which shapes both readiness for independent practice and the intensity of your schedule during school.
Which Path Is Faster?
For a working RN, the NP route skips prerequisite coursework and patient care hour accumulation, making it the faster option. If you're weighing whether to pursue a doctoral degree, review the DNP prerequisites before planning your timeline. For a non-nurse with a bachelor's degree and completed science courses, PA school can begin immediately if you meet the patient care threshold. If you lack those prerequisites, expect 12 to 24 months of coursework and clinical work before you qualify to apply.
Questions to Ask Yourself
Can a Nurse Become a Physician Assistant?
The core tradeoff here is straightforward: leverage what you already have, or start fresh on a different model of care. Yes, a registered nurse can absolutely apply to PA school, and many PA programs list RN experience among the clinical backgrounds they accept.1 But "can" and "should" are different questions, and the practical details matter more than most career guides let on.
What PA Programs Actually Require
PA programs operate through the Centralized Application Service for Physician Assistants (CASPA), and admissions requirements are built around a medical, not nursing, framework. Even with a BSN in hand, you will likely need to complete additional science prerequisites. Common requirements include anatomy and physiology, chemistry, microbiology, organic chemistry or biochemistry, statistics, and psychology.2 If your nursing curriculum covered some of these courses, you may be able to check a few boxes, but most RNs find gaps they need to fill before applying.
Beyond coursework, PA programs require direct patient care hours, typically ranging from 500 to over 2,000 depending on the school.3 The University of Wisconsin, Madison, for example, sets a minimum of 1,000 hours.3 The good news is that most programs do count RN clinical experience as qualifying patient care time. However, acceptance of those hours is program-specific, so you will want to verify with each school before assuming your bedside experience transfers.
Other common requirements include a bachelor's degree (which a BSN satisfies) and, at many programs, GRE scores.4 PA programs run as full-time, lockstep cohorts lasting 24 to 36 months, meaning you generally cannot work while enrolled.2
Why Some Nurses Consider the Switch
The most frequently cited reason nurses explore the PA path is lateral specialty mobility. PAs practice under the medical model, and they can switch from family medicine to orthopedic surgery to emergency medicine without earning a new certification each time. For nurses drawn to surgical subspecialties, where PA roles tend to be more prevalent than NP positions, this flexibility is genuinely appealing.
That said, it is worth weighing what you give up. NPs in a growing number of states hold full practice authority, meaning they can evaluate, diagnose, and prescribe independently. The NP path also builds directly on your existing credentials: a BSN feeds into an MSN or DNP program, and your years of RN experience strengthen both your application and your clinical foundation. If you are curious about what that progression looks like in practice, our guide on how to become a nurse practitioner walks through the steps in detail.
A Practical Recommendation for Working RNs
For most working nurses, the NP route is shorter, less expensive, and more logistically manageable. Many online NP programs are designed around the schedules of practicing nurses, letting you continue working while you earn your degree. The RN-to-PA pivot involves more prerequisite coursework, a full-time commitment that typically rules out employment, and the reality that your nursing license does not shorten the PA curriculum.
The RN-to-PA switch makes the most sense in a few specific scenarios:
- You are strongly drawn to the medical model of care and want the ability to move between specialties freely.
- You plan to work in surgical or procedural specialties where PA roles are more established.
- You are early enough in your career that the time and cost of a fresh start feel proportionate to the payoff.
If those scenarios do not describe you, staying on the nursing track and pursuing an NP degree is almost certainly the more efficient path forward. You can explore timeline options, including from RN to NP pathways, and build on credentials you have already earned while maintaining income during school.
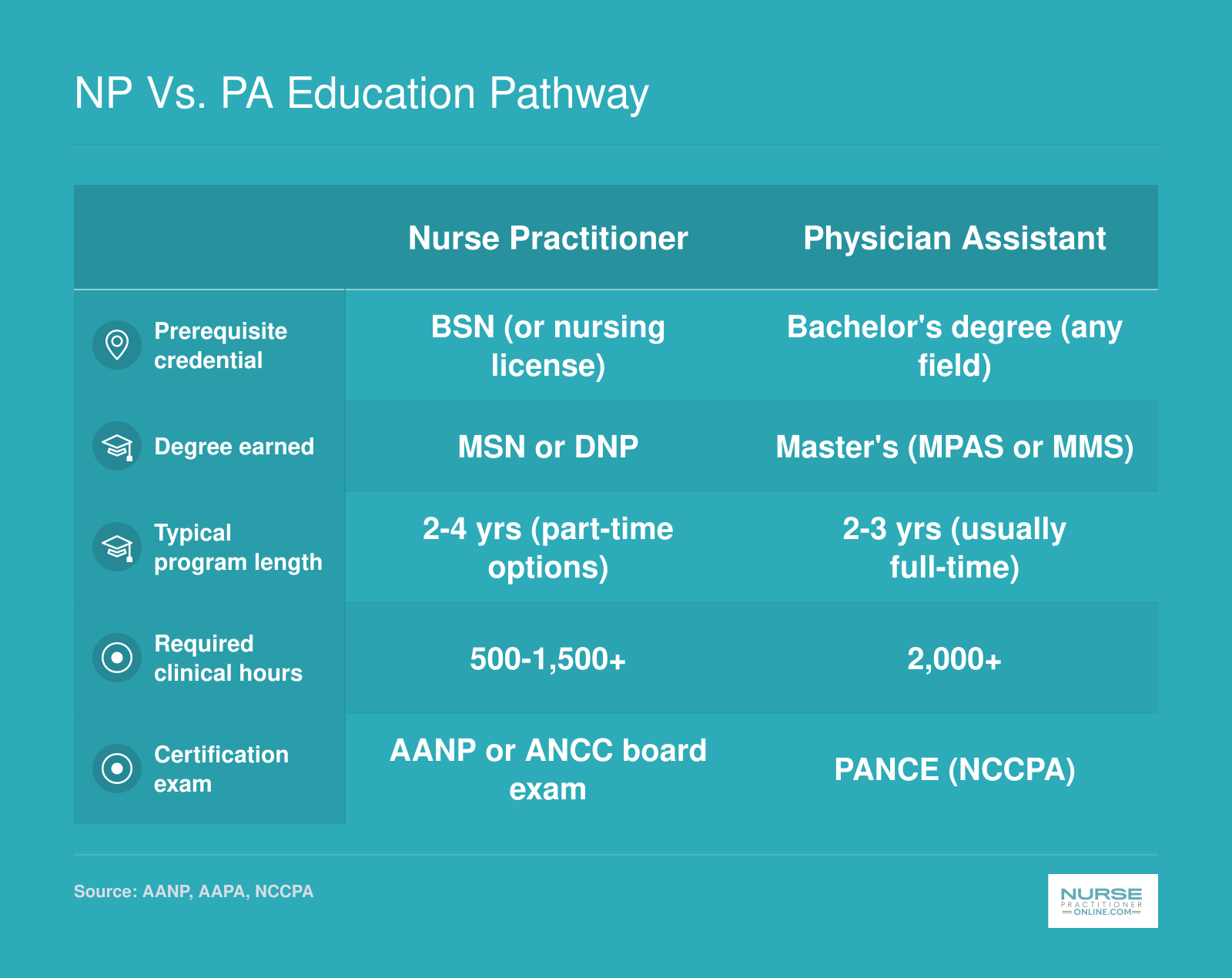
NP Vs. PA Education Pathway
Understanding how these two pathways differ in structure can help you decide which fits your background and goals. Here is a side-by-side look at the key educational milestones for each route.
Scope of Practice and Autonomy by State
Scope of practice defines exactly what you can legally do as an NP or PA: diagnose conditions, order tests, prescribe medications, and whether a physician must sign off on your work. For nurses weighing these two paths, state-by-state autonomy is often the deciding factor because it directly shapes your day-to-day independence and career flexibility.
NP Practice Authority: Full, Reduced, and Restricted
Nurse practitioners work under one of three practice environments. In full practice authority states, NPs evaluate patients, diagnose, interpret tests, and initiate treatment, including prescribing Schedule II controlled substances, without any required physician contract or supervision. As of 2026, 27 states plus the District of Columbia grant this complete autonomy, with new additions like New York and Kansas (2022), Utah (2023), and Delaware and Massachusetts (2021-2023) joining the fold.1 No additional states adopted FPA during the 2025-2026 cycle, but the long-term direction is clearly expanding.2
Reduced practice states, currently 12, limit at least one element of NP practice, often requiring a collaborative agreement with a physician for prescribing or some aspects of care. Restricted practice states (11 total) mandate direct physician supervision and delegation for most patient-care decisions.2
Even within restricted states, alternative pathways are emerging. California, for example, remains a restricted state but now offers an independent practice pathway for NPs who complete a specified number of clinical hours under supervision.3 This nuance underscores the gradual shift: the landscape is not static, and an NP's initial licensing state may not define the rest of their career. For a deeper look at what's changing, see our guide to nurse practitioner scope of practice.
PA Collaboration: Moving Toward Team-Based Care
Physician assistants traditionally practiced under a supervisory model. In most states, a PA must maintain a collaborative or supervision agreement with a physician, which outlines the scope of practice and often dictates that the physician review a percentage of charts or co-sign certain prescriptions. However, the push for Optimal Team Practice (OTP) by the American Academy of PAs is changing that. Several states have modernized their laws to eliminate the requirement for a specific supervising physician, instead allowing PAs to practice based on their own education and competency, in collaboration with their employer or healthcare team.
- States leading OTP adoption: North Dakota removed the mandatory physician agreement in 2019, shifting to a collaborative practice model where the employer determines oversight. Wyoming and Montana followed with similar reforms, giving PAs more flexibility to be hired and deployed without tying them to an individual physician.
These changes mean that in a growing number of states, a PA can work with the same day-to-day independence as an NP in a reduced or even full practice authority setting, though subtle legal differences around prescriptive authority and record review often remain.
Day-to-Day Impact: What Autonomy Looks Like on the Job
In a full practice authority state, an NP can open an independent primary care clinic, prescribe Schedule II drugs like ADHD medication, and sign home health orders, all without a physician's countersignature. In the same state, a PA might still need a collaborative agreement on file requiring a physician to periodically review charts, even if day-to-day interactions are minimal. For the PA, this can mean practical hurdles when starting a telemedicine practice or staffing a rural clinic where a physician is rarely on site.
Prescriptive authority adds another layer. Even in FPA states, some jurisdictions limit an NP's ability to prescribe controlled substances independently. For PAs, a physician's name is often required on controlled substance prescriptions even where the practice agreement is flexible. This scattershot regulation means you need to look at your specific state's rules, not just the broad category.
Choosing Autonomy: Which Path Gives You More Independence?
If complete professional independence is your priority, the NP path offers a clearer, more widespread route today. With over half the country granting full practice authority and momentum favoring expansion, an NP education positions you to practice at the top of your license immediately after licensure in many places. The PA path is catching up rapidly; states with modernized PA legislation now allow autonomy levels that rival NP reduced practice. For nurses already holding RN licensure, the NP route builds on nursing principles, and the transition to independent practice feels like a natural extension of nursing judgment. For those entering healthcare without a nursing background, a PA program followed by work in an OTP-friendly state can yield comparable autonomy over time.
The key is to check your home state's current rules and consider where you want to practice long term. Both professions are moving toward greater independence, and the gaps are narrowing every legislative session.
Salary Comparison: NP Vs. PA Pay and Earnings Outlook
When comparing nurse practitioner and physician assistant compensation, the numbers are closer than many nurses expect. Both roles represent a significant earnings jump over registered nursing, and each offers strong mid-career and upper-range earning potential. Below is a side-by-side look at national salary benchmarks from the Bureau of Labor Statistics.
| Role | Total Employed | 25th Percentile | Median Salary | 75th Percentile | Mean Salary |
|---|---|---|---|---|---|
| Nurse Practitioners | 307,390 | $109,940 | $129,210 | $149,570 | $132,000 |
| Physician Assistants | 155,540 | $113,770 | $133,260 | $160,160 | $136,900 |
| Registered Nurses (for comparison) | 3,282,010 | $78,610 | $93,600 | $107,960 | $98,430 |
Related Articles
Tuition, Debt, and Long-Term ROI
What will the total price tag be for an NP versus a PA degree, and which investment pays off faster? The answer depends heavily on the program you choose, your ability to work during school, and the specialty you pursue. Let's break down the numbers.
Tuition Ranges for NP and PA Programs
- MSN-FNP: Public universities typically charge $30,000, $50,000; private schools may reach $80,000.
- BSN-to-DNP: In-state public programs cost around $41,000, while out-of-state and private programs average $70,000, $75,000.1 Per-credit rates range from $561 (public in-state) to $1,024 (private).1 A handful of private DNP programs can exceed $200,000.2
- PA master's: Full program tuition commonly falls between $90,000 and $120,000.
The Opportunity Cost of Full-Time Study
- PA programs are rigorous and full-time, making it nearly impossible to hold a job. Students forgo two to three years of income, which could average $70,000, $90,000 annually for registered nurses.
- NP programs, especially MSN tracks, often accommodate working nurses with part-time, evening, or online formats. Many students maintain their nursing salaries, reducing the net cost of education dramatically.
Student Debt: Who Carries the Heavier Load?
- PA graduates leave school with an average debt of $110,000 to $130,000.
- NP debt is more nuanced. While national median graduate debt for NPs was reported at over $154,000, this figure includes high-cost DNP and private programs.2 MSN-prepared NPs who worked during school often finish with $40,000, $80,000 in loans.
- The path you choose matters: a working nurse in a public BSN-to-DNP program may borrow far less than a full-time private PA student.
Long-Term Earnings and Break-Even Points
Both professions enjoy similar median salaries, typically $125,000 to $130,000, with NPs in 2024 reporting a national mean of $150,000.2 Lower upfront debt and the ability to earn while learning give NPs a potential edge. One analysis pegs the NP break-even at roughly 10 years, with loan payments consuming 21% of income.2 PAs who enter surgical or specialty fields may outearn primary care NPs (see our breakdown of highest paid NP specialties), but for many nurses, the faster ramp to positive net worth favors the NP route.
It's also worth noting that many NP graduates pursue a DNP online as a terminal degree, which can increase total program cost but may open doors to leadership roles. For PAs, additional certifications or a surgical residency can boost income but may delay full earnings. Overall, the NP path, particularly for nurses already holding a BSN, can yield a quicker return on investment when factoring in lower tuition at public schools, part-time study options, and the ability to keep a paycheck throughout training.
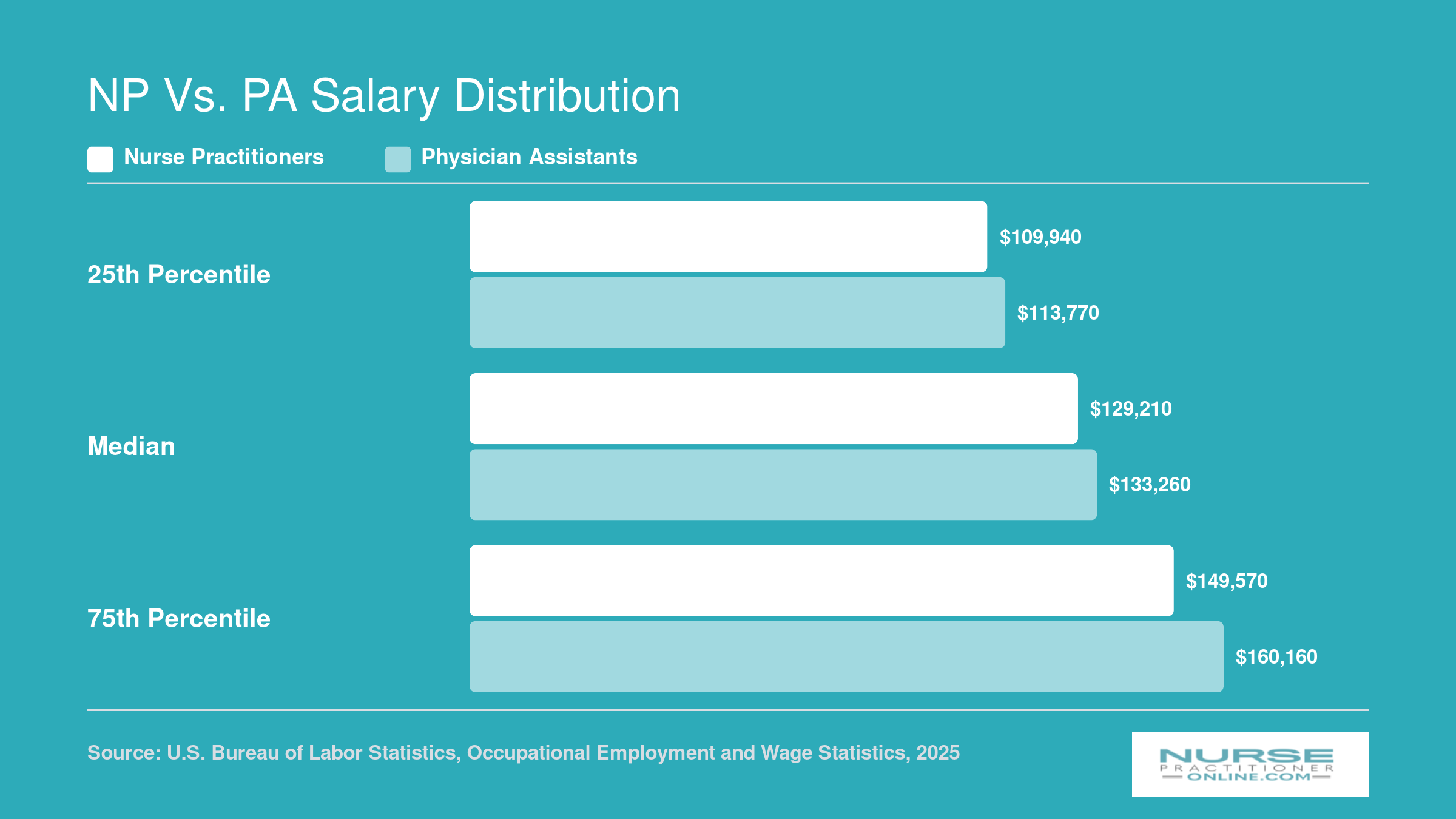
NP Vs. PA Salary Distribution
Nurse practitioners and physician assistants earn comparable salaries across the pay spectrum. As the chart below shows, the overlap is substantial, and factors like specialty, geographic location, and practice setting tend to influence earnings far more than the credential itself.
Job Growth and Employment Settings
Both nurse practitioners and physician assistants rank among the fastest-growing occupations in American healthcare, but they differ in where they work and how easily they can pivot between specialties. Understanding these distinctions can help you choose the path that aligns with your long-term career goals.
Projected Growth Rates
The Bureau of Labor Statistics projects that nurse practitioner employment will grow 40 percent between 2024 and 2034, adding approximately 128,400 new positions to a base of 320,400 NPs currently working.1 That is 13 times faster than the 3.1 percent average growth rate for all U.S. occupations. Physician assistants will see 28 percent growth over the same decade, adding between 41,000 and 42,000 positions to a 2024 workforce of roughly 149,000 PAs.1 That translates to nine times the all-occupation average. Both professions are experiencing explosive demand driven by physician shortages, aging populations, and expanded insurance access.
Where NPs and PAs Work
Nurse practitioners concentrate heavily in outpatient settings. Between 45 and 55 percent work in physician offices, with another 15 to 20 percent in dedicated outpatient clinics and 15 to 25 percent in hospitals.2 Family nurse practitioners are especially prevalent in acute care vs primary care settings such as community health centers, reflecting the nursing model's emphasis on patient education, chronic disease management, and longitudinal care. Physician assistants are more evenly distributed across work environments. You will find PAs in surgical suites, emergency departments, hospital inpatient teams, and primary care clinics in roughly equal measure. This broader spread reflects the generalist training model that allows PAs to integrate into almost any medical specialty.
Employer Preferences and Specialty Mobility
Many health systems prefer PAs for surgical and procedural teams because PAs can be supervised by any attending physician and their generalist education prepares them to function across specialties without additional certification. Other organizations favor NPs for primary care panels and chronic disease programs, valuing the nursing framework and its focus on patient-centered communication. One critical difference: physician assistants can switch specialties with on-the-job training alone, moving from orthopedic surgery to cardiology with no credential change required. Nurse practitioners must earn a new population-focus certification to change specialties. Transitioning from family nurse practitioner to psychiatric-mental health nurse practitioner, for example, requires additional graduate coursework and hundreds of supervised clinical hours. For NPs interested in aging populations, pursuing an adult gerontology nurse practitioner credential is one common pathway. If you prize maximum career flexibility and want the option to explore multiple specialties over a 30-year career, the PA model offers fewer administrative barriers to reinvention.
FNP Vs. PA in Primary Care: A Closer Look
Primary care is where the FNP versus PA debate gets most interesting, because both roles have carved out strong footholds in the same clinical territory through distinctly different routes.
How the FNP Role Is Built for Primary Care
The Family Nurse Practitioner credential was designed from the ground up for lifespan primary care. FNP programs weave health promotion, preventive screenings, chronic disease management, and patient education into every clinical encounter. The nursing model frames the patient as a whole person embedded in family and community context, which shapes not just what an FNP does, but how they approach the relationship. That philosophy translates directly into the kinds of practice FNPs gravitate toward: managing hypertension over years, counseling families on lifestyle change, coordinating care for patients juggling multiple chronic conditions.
The PA's Generalist Advantage
PAs entering family medicine come through a different door. Their training rotates through multiple specialties, building broad diagnostic exposure and grounding them firmly in the medical model: identify the problem, work through a differential, select a treatment. That breadth is genuinely useful in primary care, where anything can walk through the door. The trade-off is that the preventive and wellness-focused depth FNP programs emphasize is not the center of gravity in PA school. It is present, but it competes with training time across surgery, psychiatry, emergency medicine, and other fields.
Day-to-Day Overlap and Real-World Differences
In practice, a patient sitting across from an FNP or a PA in a family medicine clinic will experience a very similar visit. Both providers take histories, order labs, diagnose, prescribe, and follow up. The practical differences surface in two places. First, autonomy: in states with full practice authority, FNPs can operate independent practices without a physician collaboration agreement, while PAs work under supervision requirements in every state. Second, framing: FNPs tend to structure encounters around wellness and prevention as primary goals, while PAs often lead with the diagnostic framework.
Why Rural and Underserved Communities Lean on FNPs
In rural areas and federally designated health professional shortage areas, FNPs are disproportionately represented as primary care nurse practitioners. Full practice authority makes this possible: an FNP can serve as the sole licensed provider in a rural clinic, opening independently without a physician on-site or under contract. PAs cannot replicate that model under current law. For nurses drawn to community health, underserved populations, or rural service, this distinction is not a minor footnote. It is often the deciding factor.
Which Path Is Right for You? A Decision Framework
Both the nurse practitioner and physician assistant paths lead to rewarding, well-compensated careers in advanced clinical practice. The best choice depends on your professional background, career goals, and how you prefer to learn and practice. Use the framework below to weigh the strengths of each route.
Pros
- NP programs build on existing nursing experience, letting RNs leverage years of patient care knowledge and clinical intuition.
- Online and hybrid NP programs offer flexible scheduling designed for working nurses who need to maintain income during school.
- Full practice authority is available in a growing number of states, giving NPs independent prescribing and diagnostic privileges.
- NPs choose a population focus early (such as family, adult gerontology, or psychiatric mental health), allowing deep specialization from the start.
- The nursing philosophy emphasizes holistic, patient centered care, which appeals to clinicians who value long term wellness partnerships.
- FNP graduates can move directly into primary care roles with strong demand and competitive salaries across rural and urban settings.
Cons
- PA programs accept candidates from diverse undergraduate backgrounds, making the path accessible to non nurses with healthcare experience.
- The PA medical model training covers a broad generalist foundation, offering flexibility to switch specialties without additional certification.
- PA clinical rotations span multiple disciplines during the program, providing wide exposure before graduation.
- PAs may find faster entry into surgical and procedural specialties compared to most NP tracks.
- PA programs are typically completed in a continuous, full time format of about 27 months, which can mean a quicker start to earning an advanced practice salary.
- Employer perception in some hospital systems treats PA and NP roles interchangeably, so either credential can open similar doors.
Frequently Asked Questions About NPs and PAs
Choosing between the nurse practitioner and physician assistant paths raises plenty of practical questions, from certification exams to scope of practice. Below are answers to the questions working nurses ask most often, along with tips on where to verify the latest details.
- Is a physician assistant the same as a nurse practitioner?
- No. Although NPs and PAs often treat similar patient populations and may work side by side, they follow different educational models and licensing frameworks. NPs are trained in a nursing model that emphasizes holistic, patient-centered care and must hold an active RN license before entering a graduate program. PAs are trained in a medical model and complete a generalist curriculum open to applicants from various healthcare backgrounds. Their certifying bodies, scope-of-practice rules, and continuing education requirements also differ.
- Can a nurse become a physician assistant?
- Yes, a registered nurse can apply to a PA program. Most PA programs require a bachelor's degree and prerequisite science courses, plus direct patient care hours, which nurses typically have in abundance. Keep in mind that switching to the PA track means completing an entirely new clinical curriculum rather than building on your nursing credentials. If you already hold a BSN, pursuing an MSN or DNP to become an NP may be a more direct route to advanced practice.
- Which has more autonomy, an NP or a PA?
- It depends on the state. As of 2026, more than half of U.S. states and Washington, D.C., grant NPs full practice authority, meaning they can evaluate, diagnose, and prescribe without a collaborating physician. PA practice, by contrast, still requires a collaborative or supervisory agreement with a physician in most states, although several states have recently moved toward Optimal Team Practice arrangements that reduce those requirements. Always check your state board of nursing or medical board for the most current rules.
- How do NP and PA certification exams compare?
- NPs choose a population-focused certification exam through either the American Nurses Credentialing Center (ANCC) or the American Academy of Nurse Practitioners Certification Board (AANP). Each organization publishes exam format details and renewal timelines on its website (nursingworld.org for ANCC, aanp.org for AANP). PAs take the Physician Assistant National Certifying Exam (PANCE) administered by the NCCPA, then maintain their PA-C credential through continuing medical education and periodic recertification via the PANRE. Current PANCE format, pass rates, and maintenance requirements are available at nccpa.net under the exam resources and certification maintenance sections.
- Where can I find unbiased pass rate and certification data?
- For aggregated exam statistics across healthcare professions, look at reports from the National Commission for Certifying Agencies (NCCA), which accredits the certifying bodies for both NPs and PAs. The Bureau of Labor Statistics (bls.gov) also publishes data on how certification influences employment outcomes and median earnings. These sources can help you compare the two credentials on a level playing field without relying solely on marketing materials from either profession.
- Do NPs or PAs make more money?
- Nationally, median salaries for NPs and PAs are remarkably close. The Bureau of Labor Statistics reports median annual wages in a similar range for both professions, with exact figures varying by specialty, geographic region, and practice setting. In some markets PAs edge ahead; in others, especially where NPs hold full practice authority and run independent practices, NPs may earn more. Specialty certifications, years of experience, and willingness to work in underserved areas also influence pay.
- Who should I contact for personalized guidance on choosing between the NP and PA paths?
- Start with your school's pre-health or nursing advisor, who can map your current coursework to each program's prerequisites. Professional associations are another excellent resource. The American Association of Nurse Practitioners (AANP) and the American Academy of Physician Associates (AAPA) both publish fact sheets, recertification guides, and career planning tools on their websites. Speaking with practicing NPs and PAs in your area of clinical interest can also give you a realistic picture of day-to-day responsibilities and long-term career satisfaction.